Pulmonary embolism with pulmonary hypertension or something far worse? Unveiling a rare and lethal pulmonary artery angiosarcoma: a case report
Gianluca Guarnieri, Daniele Briguglia, Edoardo Conte, Daniele Andreini

TL;DR
A rare and deadly tumor in the pulmonary artery was misdiagnosed as a pulmonary embolism, highlighting the need for careful differential diagnosis.
Contribution
This case report highlights the diagnostic challenges and clinical importance of pulmonary artery angiosarcoma.
Findings
Pulmonary artery angiosarcoma can mimic pulmonary embolism on imaging, leading to diagnostic delays.
Early recognition and multidisciplinary management may improve outcomes in this aggressive malignancy.
Abstract
Pulmonary artery angiosarcoma is a rare and highly malignant tumour. Its clinical presentation often mimics common pulmonary disorders such as pulmonary embolism or pneumonia, which frequently leads to misdiagnosis. Due to its aggressive nature and typical diagnostic delay, prognosis is generally poor, with survival often limited to a few months post-diagnosis. A 70-year-old female with a history of hypertension and no previous cardiac issues presented with progressive exertional dyspnoea unresponsive to anticoagulation after a diagnosis of pulmonary embolism. A chest computed tomography (CT) initially suggested a pulmonary embolism with an endoluminal filling defect in the right pulmonary artery. However, further investigation revealed a mass in the right pulmonary artery with a subsequent obliteration of the perihilar fat spaces, leading to a diagnosis of pulmonary artery…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
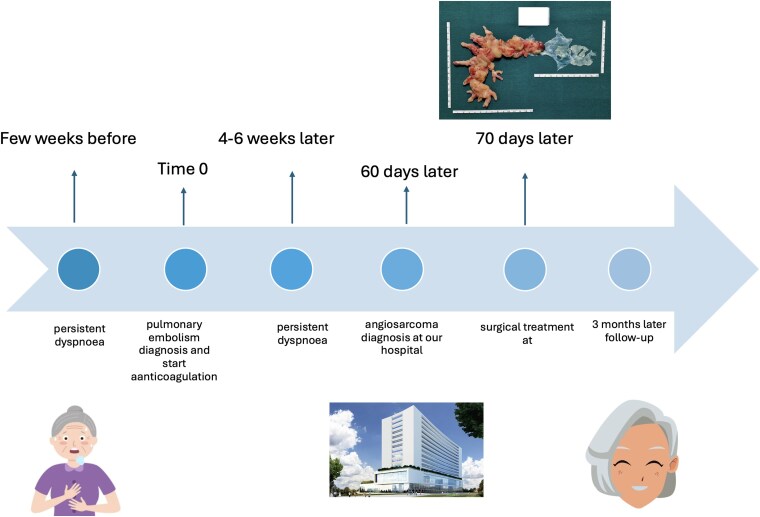 Figure 1
Figure 1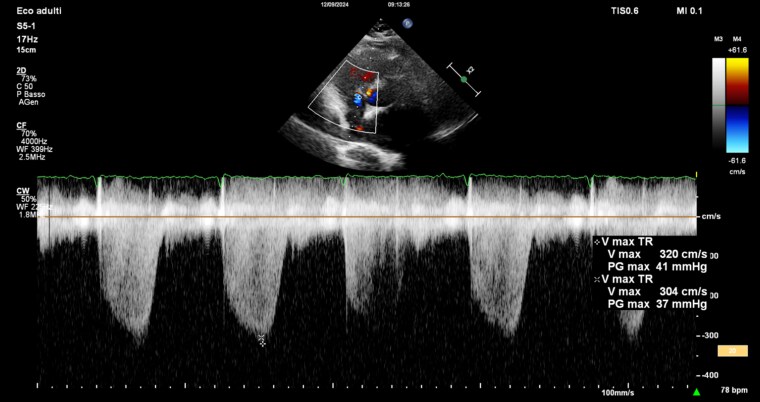 Figure 1
Figure 1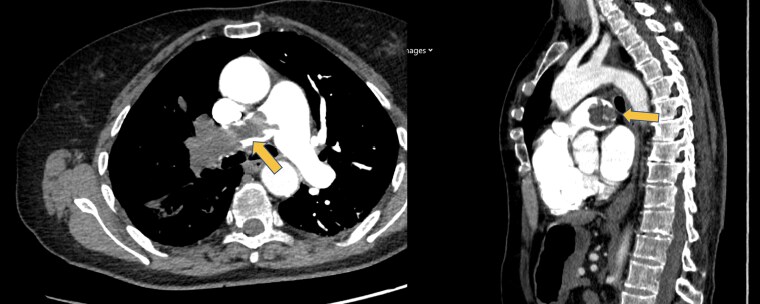 Figure 2
Figure 2 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac tumors and thrombi · Vascular Tumors and Angiosarcomas · Medical Imaging and Pathology Studies
Background
Pulmonary artery angiosarcoma is a highly malignant and rare form of cancer that arises from the endothelial cells of the pulmonary arteries. This tumour is notoriously aggressive, often presenting with nonspecific symptoms including chest pain, coughing, and sometimes haemoptysis that mimic more common pulmonary disorders such as thromboembolism and pneumonia, which leads to frequent misdiagnoses.^1^
Due to its aggressive nature and the typical delay in diagnosis, the prognosis for patients with pulmonary artery angiosarcoma is generally poor, with survival times often not extending beyond seven months after diagnosis.^2^ Treatment options are limited but can include surgical resection, chemotherapy, and radiation therapy, though their efficacy is often restricted by the advanced stage of the disease at diagnosis.^3^ The rarity and severity of pulmonary artery angiosarcoma underscore the importance of considering it in differential diagnoses for pulmonary symptoms and utilizing advanced imaging and histopathological examination to confirm the diagnosis.
Summary Figure
**
Case description
A 70-year-old female patient presented with a history of hypertension and no previous cardiac issues. One year prior, she had undergone decompression surgery of L4-L5 and arthrodesis, and a few years earlier, she had a hysterectomy with annexectomy for a benign ovarian cyst.
A month before her current presentation, the patient was hospitalized for exertional dyspnoea that had been present for several weeks. A tomography (CT) scan revealed a significant endoluminal filling defect in the right pulmonary artery, suggestive of pulmonary thromboembolism. Echocardiography showed slightly dilated right heart chambers but a normally functioning ventricle with tricuspid annular plane systolic excursion (TAPSE) of 28 mm, fractional area change (FAC) of 40%, systolic velocity of the tricuspid annulus (S’TDI) 10 cm/s, and an indirect increase in systolic pulmonary artery pressure (sPAP, 45 mmHg). The patient was then started on therapeutic low molecular weight heparin followed by discharge with a prescription for oral anticoagulation with rivaroxaban 20 mg/day.
The patient visited two months later our emergency department (ED) due to a syncopal episode and reported persistent dyspnoea despite being on oral anticoagulant therapy. At the ED the patient presented with tachypnoea with minimal basal crackles on chest auscultation and in the absence of peripheral oedema. Her blood pressure was 110/70 mmHg and her heart rate was 95 bpm, with an oxygen saturation of 90%. The ECG showed sinus rhythm, normal atrio, and intra-ventricular conduction with nonspecific repolarization abnormalities. The blood tests revealed high-sensitivity troponin I (hsTnI) at 389 ng/L (reference range up to 53 ng/L) and Pro-Brain Natriuretic Peptide (proBNP) at 184 ng/mL (reference range up to 125 pg/mL); other results within normal limits. The transthoracic-echocardiogram showed normal biventricular systolic function, with a slight increase in right ventricle volumes, with systolic function (TAPSE, 25 mm; FAC, 37%) and mild tricuspid regurgitation with a velocity of 3 cm/s as shown in Figure 1 with sPAP at 46 mmHg.
Doppler echocardiography showing a right ventricle-to-atrium pressure gradient of 37 mmHg and a regurgitation velocity greater than 2.8 m/s.
The contrast-enhanced chest CT showed an expanded filling defect in the right pulmonary artery.
The patient was initially admitted to the coronary care unit under the suspicion of a recurrent pulmonary embolism; however, a few hours later, the radiologist informed us that in the venous phase, there was an obliteration of the perihilar spaces, forming a mass-like appearance at this level and that these findings were suggestive of a vascular-origin neoplasia (less likely a diagnosis of pulmonary embolism), as shown in Figure 2.
Computed tomography scan showing the pulmonary angiosarcoma, indicated with the yellow arrows.
The images were then shown to an in-house thoracic surgeon, who leaned towards a diagnosis of pulmonary embolism and recommended continuing the anticoagulant therapy. However, we decided to have the images reviewed by a second centre, known for its expertise in treating pulmonary vascular-origin neoplasms. The surgeon at this centre agreed with our radiologist’s diagnosis of pulmonary vascular-origin neoplasm. The patient also underwent a venous colour Doppler ultrasound of both the upper and lower limbs, which did not show any thrombotic formations.
The patient was subsequently transferred to this secondary level centre, where she underwent an open surgical resection of the mass, as shown in Figure 3. The lesion appeared macroscopically with protrusions measuring 15/14 mm. The histological examination of the resected lesion confirmed the presence of an angiosarcoma of the pulmonary artery. After some days of rehabilitation, the patient was discharged and started chemotherapy with doxorubicin administered at a standard dose of 60 mg/m² intravenously every 3 weeks, with a cumulative maximum dose of 450 mg/m, and after 3 months, is still alive.
Histological examination of the resected pulmonary angiosarcoma.
Discussion
Sarcomas originating from endothelial cells constitute two % of all sarcomas, which are themselves very rare tumours. The primary manifestation is dyspnoea, followed by chest pain; these patients may develop symptoms of pulmonary hypertension.^4^ Indeed, if the lesion grows over months, the patient may not only experience dyspnoea but also symptoms of right heart failure. Moreover, the patient may exhibit an increase in systolic pulmonary pressure and dilation of the right cardiac chambers, as was the case with our patient; indeed, she had been experiencing dyspnoea for several months, and two echocardiograms conducted about a month apart showed dilation of the right chambers with increased sPAP.
Diagnosis is challenging, and cases of misdiagnosis are already reported in the literature.^5^ Our patient was initially misdiagnosed at the first centre that admitted her, mistaking this neoplasm for a pulmonary embolism. Our diagnosis was facilitated by the fact that the patient remained persistently symptomatic despite anticoagulant therapy. According to literature data, the recurrence of pulmonary embolism despite anticoagulant therapy is a very rare event, affecting about two % of all venous thromboembolisms (VTEs).^6^ Moreover, embolism may coexist with malignancies arising from the heart and vessels, and anticoagulation is frequently considered in clinical practice also for this reason.
What should guide the diagnosis are both clinical and radiological characteristics; on the one hand, our patient was already on anticoagulant therapy and did not have deep vein thrombosis of distant vessels, and on the other hand, the radiological images were more suggestive of a primary form of neoplasia.
Radiologically, pulmonary artery angiosarcoma on CT imaging often presents as an intraluminal mass extending along the pulmonary artery with irregular or lobulated margins and possible infiltration of the vessel walls. These tumours can show heterogeneous enhancement following contrast administration due to their vascular nature. This contrasts with pulmonary embolism, which typically appears as filling defects confined to the vascular lumen and shows minimal or no enhancement. Additional malignant features such as local tissue invasion and metastases may also be present with angiosarcomas, unlike in cases of pulmonary embolism. The fact that the patient had this significant filling defect on only one side made the diagnosis of pulmonary embolism less likely.
This condition, in addition to being rare and challenging to diagnose, also lacks specific management guidelines. As a result, its treatment is often entrusted to highly specialized centres that rely on local expertise and experience. A multidisciplinary approach is essential, involving specialists such as cardiologists, cardiothoracic surgeons, radiologists, thoracic surgeons, and oncologists. Cardiologists play a fundamental role in the management of pulmonary angiosarcomas, particularly due to the necessity of monitoring the cardiotoxic effects associated with anthracycline-based chemotherapy. These drugs carry a significant risk of dose-dependent cardiac toxicity, making continuous cardiac monitoring essential both during and after treatment. Regular assessment of cardiac function is necessary and typically involves echocardiography, biomarker analysis (troponin, proBNP), and, when indicated, cardiac MRI. Early detection of subclinical cardiac impairment allows for the timely implementation of cardioprotective therapies, such as angiotensin-converting enzyme (ACE) inhibitors or beta-blockers, which can help reduce the risk of long-term cardiac complications.^7^
Early diagnosis is crucial; cases with survival beyond 5 years have been reported when the condition is detected in time.^3^ Thus, in instances of persistent dyspnoea, pulmonary hypertension, or recurrent pulmonary embolism unresponsive to anticoagulants with a perfusion defect in the pulmonary artery, this silent killer should always be considered.
Conclusion
In conclusion, pulmonary artery angiosarcoma is a rare, aggressive malignancy often misdiagnosed as pulmonary embolism due to nonspecific symptoms. This case emphasizes the need to consider angiosarcoma in patients with persistent pulmonary symptoms unresponsive to standard therapies. Early diagnosis through a multidisciplinary approach can improve outcomes, highlighting the importance of awareness among clinicians.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Darawsha F, Kramer R, Raanani E, Saute M. Angiosarcoma of the main pulmonary artery-hand-made conduit reconstruction. Interact Cardiovasc Thorac Surg 2022;35:ivac 096.35438178 10.1093/icvts/ivac 096PMC 9419682 · doi ↗ · pubmed ↗
- 2Khalid K, Khan A, Lomiguen CM, Chin J. Clinical detection of primary pulmonary angiosarcoma. Cureus 2021;13:e 17059.34522537 10.7759/cureus.17059 PMC 8428157 · doi ↗ · pubmed ↗
- 3Chaubey S, Benson C, Khan H, Monaghan M, Shah AM, Judson I, et al Six-year survival of a patient with pulmonary artery angiosarcoma. Asian Cardiovasc Thorac Ann 2012;20:728–730.23284122 10.1177/0218492312441780 · doi ↗ · pubmed ↗
- 4Correale M, Tarantino N, Ieva R, Gravina M, Casavecchia G, Strazzella C, et al Don’t stop at first glance: pulmonary artery angiosarcoma mimicking chronic thromboembolic pulmonary hypertension. Pulm Circ 2018;8:2045894018785047.29873586 10.1177/2045894018785047 PMC 6109853 · doi ↗ · pubmed ↗
- 5Desmarais P, Laskine M, Caporuscio C. Primary pulmonary artery angiosarcoma mimicking pulmonary embolism in a 66-year-old man with dyspnea. C Can Med Assoc J = J l’Association medicale Can 2016;188:E 509–E 512.10.1503/cmaj.151417 PMC 513552927527482 · doi ↗ · pubmed ↗
- 6Klamroth R, Riess H, Beyer-Westendorf J, Linnemann B. Recurrent venous thromboembolism in patients on anticoagulation: an update based on the revised AWMF S 2k guideline. Hamostaseologie 2024;44:150–154.38688270 10.1055/a-2173-7729 · doi ↗ · pubmed ↗
- 7Camilli M, Cipolla CM, Dent S, Minotti G, Cardinale DM. Anthracycline cardiotoxicity in adult cancer patients: JACC: Cardio Oncology state-of-the-art review. JACC Cardio Oncol 2024;6:655–677.39479333 10.1016/j.jaccao.2024.07.016PMC 11520218 · doi ↗ · pubmed ↗