Severe Maternal Outcome in Women Admitted to an Obstetric Intensive Care Unit in the Northeast of Brazil: A Cross-Sectional Study
Flávio Xavier da Silva, Ryta de Kássia Andrade Rufino, Micaelly Barbosa Padilha, Stephanie Karoline Santos Bezerra, Mario Diego Teles Correia, Leila Katz

TL;DR
This study examines the causes and outcomes of severe maternal complications in a Brazilian obstetric ICU, finding that infections and other direct obstetric issues are major contributors.
Contribution
The study identifies puerperal infection as the most significant factor associated with severe maternal outcomes in a specific Brazilian region.
Findings
48.5% of women admitted to the ICU experienced severe maternal outcomes.
Puerperal infection was most strongly associated with severe maternal outcomes.
Hypertensive syndromes and postpartum haemorrhage were also major causes of severe maternal outcomes.
Abstract
Objective: The objective of this study is to describe the characteristics of women who experienced severe maternal outcomes (SMO: maternal near-miss or maternal death) in an obstetric intensive care unit (ICU). Methods: A cross-sectional study was carried out including pregnant or postpartum women up to 42 days of childbirth admitted to the obstetric ICU at one reference centre in the northeast of Brazil, for any clinical, surgical, or obstetric complication, with data collected between October 29, 2018, and September 30, 2019. Maternal characteristics, details on admission to the ICU, pregnancy outcomes, and causes for ICU admission were compared between groups with SMO or with the remaining group, potential life-threatening conditions (PLTCs). A significance level of 5% was adopted. Results: During the study period, 309 women were admitted to the obstetric ICU and considered…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
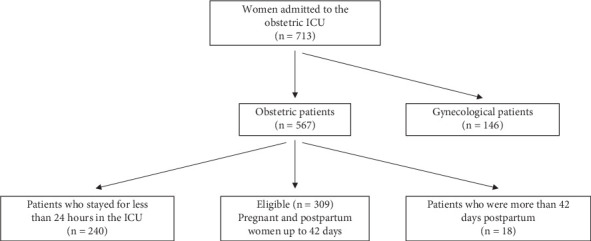 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMaternal and fetal healthcare · Maternal and Perinatal Health Interventions · Pregnancy and preeclampsia studies
1. Introduction
Maternal near-miss and maternal death together, according to the World Health Organization (WHO), are considered as a severe maternal outcome (SMO) [1, 2]. The WHO refers to maternal morbidity as a continuum from minor to SMO, and on this continuum, there are potential life-threatening conditions (PLTCs) [3, 4]. Many maternal PLTCs are preventable and treatable. Postpartum haemorrhage, hypertensive syndromes, and infection are the most common causes of death, and when death is avoided, they can result in serious health injury [5–7].
Maternal death, according to the WHO [8, 9], is defined as the death of a woman while pregnant or within 42 days after childbirth, irrespective of duration or site of the pregnancy, due to any cause related to or aggravated by the pregnancy or its management, but not from unintentional or incidental causes. It is an important health indicator which reflects socioeconomic and ethnic deprivation of women, conditions that are difficult to change [10]. However, its prevention is extremely sensitive to obstetric care, and these may be changeable [11].
Additionally, other important definition is severe maternal morbidity (SMM) or “maternal near-miss” as the term recommended by WHO, which refers to a woman who survived very serious complications, during pregnancy, childbirth, or within a subsequent period of 42 days [12]. These women share many aspects with those who die, and they are in greater quantity, thus being an important predictor for the assessment of the quality of healthcare. There is no consensus on a single definition of SMM. However, it is based on clinical, intervention, and laboratory markers in accordance with the WHO [12].
Intensive care units (ICUs) represent an opportunity of protection for women who, in several cases, had their healthcare delayed: delay in deciding to seek care, delay in arriving at a health facility, and delay in the provision of adequate care [13]. There is evidence about their benefits in reducing maternal morbidity and mortality [14]. The advantages of an obstetric ICU within an obstetric setting are numerous, for instance, the concurrent availability of expert obstetric care and critical care management. Antenatal patients admitted to the obstetric ICU have the possibility of continuous fetal monitoring with on-hand expertise in its interpretation [15].
In the world, 287,000 maternal deaths were estimated for the year 2020, the first year of the COVID-19 pandemic, resulting in a maternal mortality ratio (MMR: maternal deaths per 100,000 live births (LBs)) of around 223 maternal deaths per 100,000 LBs [8]. The proportion of all COVID-19 deaths was uncertain [8]. The great majority of these deaths occurred in low-income countries as a result of complications related to pregnancy and childbirth [9]. High parity, poverty, difficult access to health facilities, and social and regional discrepancies have been some of the challenges faced by many countries in reducing maternal death [16, 17].
Maternal mortality (MM) in Brazil has not decreased enough in recent years. According to data available in the Brazilian information system about mortality (SIM), 1640 deaths of this nature occurred in the year 2020, which represents an MMR of 64 deaths per 100,000 LBs, almost five times higher than rich countries [18]. Of this total, 32% occurred in the northeast region [18]. These data will probably increase in coming years as a consequence of the pandemic caused by the SARS-CoV-2 virus, which in 2021 had already reached an alarming lethality rate of 7.2% in pregnant and postpartum women, more than double the lethality of the general population of the country (2.8%) [19].
This study described the characteristics of women who experienced SMO in accordance with the WHO criteria, in an obstetric ICU, in the northeast of Brazil, providing the understanding of demographic and obstetric characteristics of hospitalized women who had complications during pregnancy, during delivery, or in the postpartum period. Data are presented from a database collected between October 29, 2018, and September 30, 2019, before the COVID-19 pandemic.
2. Methods
2.1. Study Design
This research is a cross-sectional study conducted at a public hospital, a referral obstetric centre, located in the city of Recife, state of Pernambuco, northeast region of Brazil: the Instituto de Medicina Integral Prof. Fernando Figueira (IMIP), with data collected between October 29, 2018, and September 30, 2019. This unit is an academic tertiary centre equipped with an obstetric ICU.
2.2. Sample of Participants
The study population consisted of pregnant and postpartum women up to the 42nd day after childbirth admitted to the obstetric ICU for any serious clinical, surgical, or obstetric complication for at least 24 h. A database had been previously built on the Research Electronic Data Capture (REDCap) secure web platform to enter data for all ICU patients. This database was used in the external validation study of the CIPHER model in Brazil [20, 21]. Patients previously entered in this database were included in the current study.
2.3. Data Collection (Measurement of Results)
We used information on maternal age (years), marital status (with or without partner), body mass index (kg/m^2^), number of prenatal visits, number of pregnancies and parity, reason for admission (direct obstetric, indirect obstetric, and both), time of admission (antepartum or postpartum), gestational age on admission (weeks), length of stay in the ICU (days), early miscarriage, stillbirth, early neonatal death (from birth up to the seventh day of life), type of delivery (vaginal or cesarean), birth weight (g), hospital discharge while pregnant, and number of maternal near-miss and maternal deaths. Women with missing control or demographic variables were included.
2.4. Statistical Methods
For statistical analysis, Statistical Package for the Social Sciences (SPSS program) version Statistics 28 was used. For comparison of baseline characteristics of groups with and without the composite outcome, the chi-square test was used for categorical variables, and Fisher's exact test was used for expected values less than 5. It was only possible to use parametric Student's T-test for only age and birth weight. For the others, which did not have normal distribution, the test used was the Mann–Whitney U test (nonparametric). A significance level of 5% was adopted.
2.5. Ethics Approval and Consent to Participate
Institutional Review Board (IRB) approval was obtained at the Instituto de Medicina Integral Prof. Fernando Figueira (IMIP) (CAAE: 52164121.4.0000.5201). This retrospective data collection was considered exempt from requiring a written informed consent.
3. Results
Over the study period, 309 women were admitted to the obstetric ICU and considered eligible for the study (Figure 1). Characteristics of the study population are presented in Table 1, comparing women with SMO and with PLTC. Most of the women with SMO were admitted to the ICU for longer and had a shorter gestational period at ICU admission for women admitted antepartum. SMO was observed in 150 (48.5%) women. Of these, 8 (2.6%) were maternal deaths, and 142 (45.9%) had one or more near-miss criteria (Table 2). The condition most associated with SMO was puerperal infection (Table 3).
Causes of maternal death were cerebral haemorrhage after eclampsia, acute pulmonary edema after severe preeclampsia, septic shock after bacterial meningitis, acute pulmonary thromboembolism, peripartum cardiomyopathy, septic shock after systemic infection in an HIV-infected patient, shock in a patient with advanced cervical cancer, and shock after puerperal haemorrhage.
4. Discussion
In this study, 150 (48.5%) patients were identified as SMO. However, only 8 (2.6%) women died. In a study conducted in a general ICU in Nigeria [22], the number of maternal deaths was significantly higher compared to the current study (43 from 101 obstetric patients, 42.6%). It is believed that general ICUs adopt different criteria of admission. Obstetric patients admitted to general ICUs tend to have a more severe condition, requiring advanced support such as advanced respiratory support, two or more organ system support, and support for acute reversible failure of another organ system in those with chronic system insufficiency, whereas patients admitted to obstetric ICUs present conscious and have single-organ dysfunction; in fact, obstetric ICUs have incorporated admission criteria from intermediate or high-dependency care units [15]. However, it is possible that many patients admitted to the obstetric ICU were using magnesium sulfate exclusively without any organ dysfunction.
Most women with a SMO were admitted for direct obstetric causes such as hypertensive syndromes, postpartum haemorrhage, and puerperal infection. Also, direct obstetric causes were the most prevalent cause of maternal deaths (5/8). Direct obstetric causes are those resulting from obstetric complications during pregnancy, labour, and puerperium, from interventions, omissions, or incorrect treatment or from a chain of events occurring from any of the above [23]. As a comparison, indirect obstetric causes such as community-acquired pneumonia, acute cardiogenic lung edema, and decompensated diabetes mellitus were less prevalent. Indirect obstetric causes are those resulting from previous existing disease or disease that developed during pregnancy and which was not due to direct obstetric causes but was aggravated by physiologic effects of pregnancy [3, 4]. These findings are in line with data from other studies [5–7], including a study conducted in the southeast of Brazil, which found that direct obstetric causes are the predominant reasons for admission to the ICU and the main causes of maternal death [24].
One or more near-miss criteria were present in 142 (45.9%) women. Near-miss morbidity, which refers to woman who almost died, was more characterised by cardiovascular dysfunction. The use of continuous vasoactive drugs, such as vasodilators and vasoconstrictors, was the most common reason for cardiovascular dysfunction. Vasodilators were administered in severe hypertension and vasoconstrictors in severe hypotension by, for example, septic shock. Other very common criteria were intubation, thrombocytopenia, and hysterectomy.
Puerperal infection was the cause most associated with SMO. Infections and sepsis have historically been linked to maternal deaths and continue to be leading causes of morbidity and mortality among women during and after pregnancy [25]. However, it is noteworthy that maternal death was not observed in these cases, probably because this infection tends to affect a younger, healthier population and, with adequate treatment, has lower mortality rates [26]. Our finding supports previous work by Igbaruma et al. in Nigeria [22], who have argued that infection ranked high in the near-miss morbidity subgroup with reduced mortality rates. Emergency obstetric hysterectomy is recognized as a life-saving intervention responsible for reducing MM related to both haemorrhage and infection [27–29].
Most of the women with SMO were admitted to the ICU for longer and had a shorter gestational period at ICU admission for women admitted antepartum. For obvious reasons, women who had more severe complications needed to stay longer in the ICU. We hypothesize that pregnant women with a shorter gestational period had comorbidities and probably were high-risk pregnancies, thereby increasing the number of severe complications.
4.1. Study Limitations
We believe that a larger sample size would demonstrate an association between haemorrhage and SMO. However, this work highlighted the need for a specialised obstetric ICU and aimed to raise awareness about the characteristics of SMO to improve strategies especially related to the prevention of hypertensive syndromes, postpartum haemorrhage, and puerperal infection.
5. Conclusion
SMO is a commonly occurring outcome in an obstetric ICU with a great possibility of treatment. The high prevalence of direct obstetric causes such as hypertension, haemorrhage, and infection was relevant in the development of SMO. Puerperal infection was the most significant cause of SMO, reiterating the need for preventive obstetric care during the antepartum, intrapartum, and postpartum periods.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Souza J. P. Cecatti J. G. Haddad S. M. The WHO Maternal Near-Miss Approach and the Maternal Severity Index Model (MSI): Tools for Assessing the Management of Severe Maternal Morbidity P Lo S One 201278 e 4412910.1371/journal.pone.00441292-s 2.0-8486558495422952897 PMC 3430678 · doi ↗ · pubmed ↗
- 2Say L. Souza J. P. Pattinson R. C. WHO working group on Maternal Mortality and Morbidity classifications Maternal Near Miss -- Towards a Standard Tool for Monitoring Quality of Maternal Health Care Best Practice & Research Clinical Obstetrics & Gynaecology 200923328729610.1016/j.bpobgyn.2009.01.0072-s 2.0-6734925226619303368 · doi ↗ · pubmed ↗
- 3Adeniran A. S. Ocheke A. N. Nwachukwu D. Non-Obstetric Causes of Severe Maternal Complications: A Secondary Analysis of the Nigeria Near-Miss and Maternal Death Survey BJOG 2019126 S 3414810.1111/1471-0528.156232-s 2.0-8506792324130897278 · doi ↗ · pubmed ↗
- 4Silva F. X. Katz L. Cecatti J. G. Prognostic Scores for Prediction of Maternal Near Miss and Maternal Death After Admission to an Intensive Care Unit: A Narrative Review Health Care for Women International 20234410-111558157210.1080/07399332.2022.213439136256459 · doi ↗ · pubmed ↗
- 5Adeoye I. A. Ijarotimi O. O. Fatusi A. O. What Are the Factors That Interplay From Normal Pregnancy to Near Miss Maternal Morbidity in a Nigerian Tertiary Health Care Facility? Health Care for Women International 2015361708710.1080/07399332.2014.9438392-s 2.0-8492051920125119488 PMC 4308809 · doi ↗ · pubmed ↗
- 6Chowdhury M. E. Ahmed A. Kalim N. Koblinsky M. Causes of Maternal Mortality Decline in Matlab, Bangladesh Journal of Health, Population and Nutrition 200927210812310.3329/jhpn.v 27i 2.33252-s 2.0-6764982287919489410 PMC 2761779 · doi ↗ · pubmed ↗
- 7Koblinsky M. Chowdhury M. E. Moran A. Ronsmans C. Maternal Morbidity and Disability and Their Consequences: Neglected Agenda in Maternal Health Journal of Health, Population and Nutrition 201230212413010.3329/jhpn.v 30i 2.112942-s 2.0-8486510258922838155 PMC 3397324 · doi ↗ · pubmed ↗
- 8World Health Organization Trends in Maternal Mortality 2000 to 2020: Estimates by WHO 2023 UNICEF, UNFPA, World Bank Group and UNDESA/Population Division https://apps.who.int/iris/handle/10665/327596