Comparison of Endarterectomy and Stenting in the Treatment of Carotid Artery Stenosis: A Real-World Nationwide, Total Population-Based Study from Korea
Sang Ah Lee, Dong-Hyuk Cho, Jimi Choi, Jun Gyo Gwon

TL;DR
This study compares carotid endarterectomy and stenting for carotid artery stenosis in Korea, finding different risks and outcomes for symptomatic and asymptomatic patients.
Contribution
A nationwide, real-world comparison of CEA and CAS outcomes using propensity score matching in a large Korean population.
Findings
Symptomatic CAS patients had lower early stroke risk but higher CVD mortality.
Asymptomatic patients showed similar outcomes between CEA and CAS.
Long-term mortality remained higher for CAS in symptomatic patients.
Abstract
Purpose: Carotid endarterectomy (CEA) and carotid artery stenting (CAS) are both well-established treatments for carotid artery stenosis. We analyzed real-world data from the Korean National Health Insurance Service (NHIS) database to compare the clinical outcomes. Methods: This retrospective cohort study included patients with carotid artery stenosis registered in the NHIS from 2008 to 2018. Patients who underwent either treatment were divided into CEA or CAS groups and subjected to 1:4 propensity score matching. Results: The study cohort included 1521 CEA and 6768 CAS patients. In symptomatic patients, the stroke rate within 1 month was lower in the CAS group (hazard ratio [HR], 0.61). However, the incidence of cardiovascular disease (CVD) death was higher in the CAS group at 1 month, 1 year, and during the total follow-up (HRs, 4.18, 2.43, and 1.50). There were no significant…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
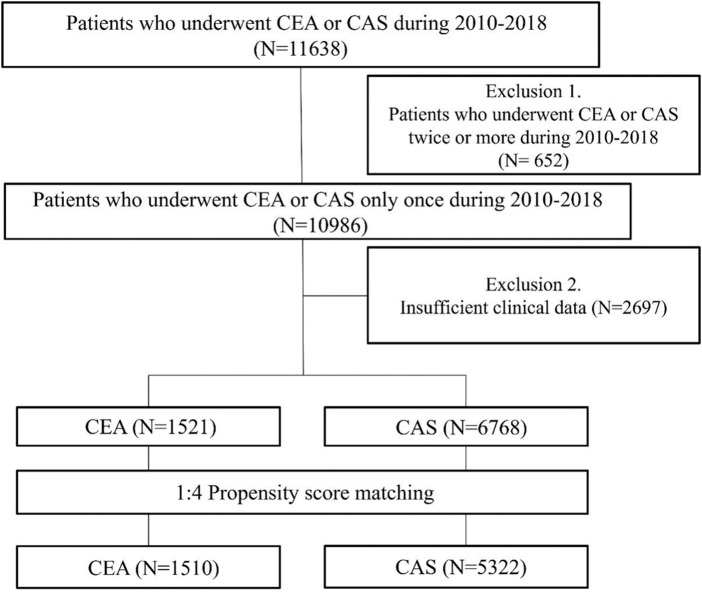 Fig. 1
Fig. 1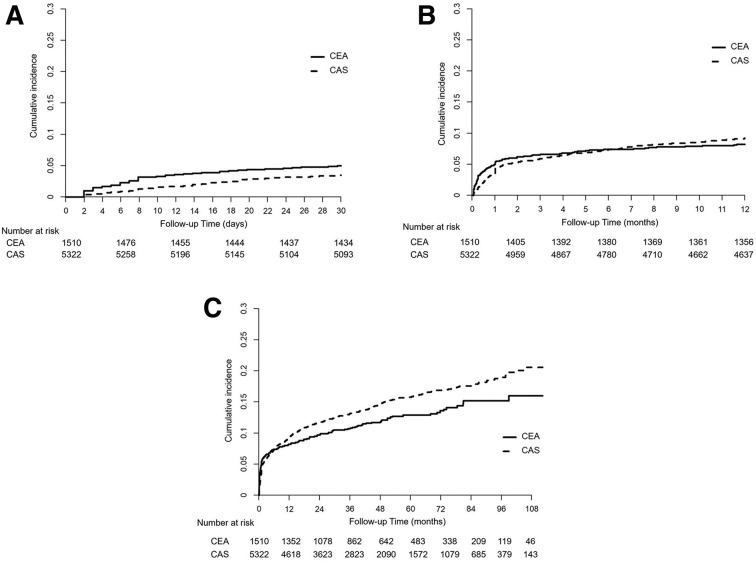 Fig. 2
Fig. 2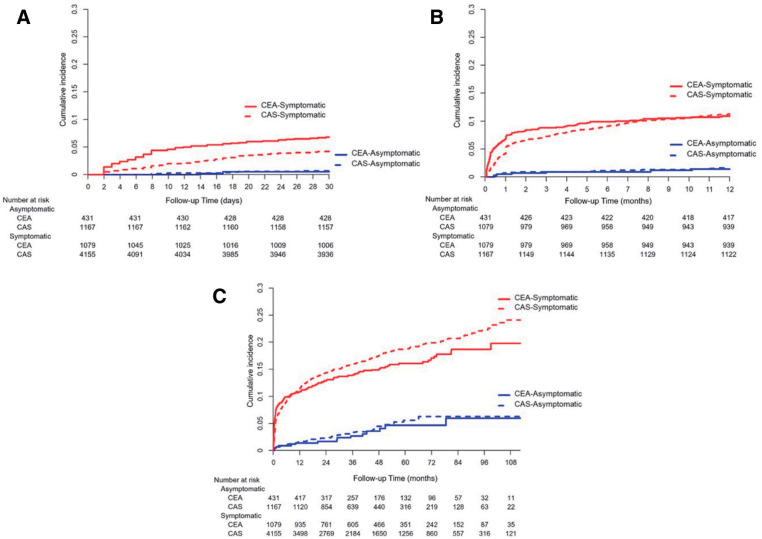 Fig. 3
Fig. 3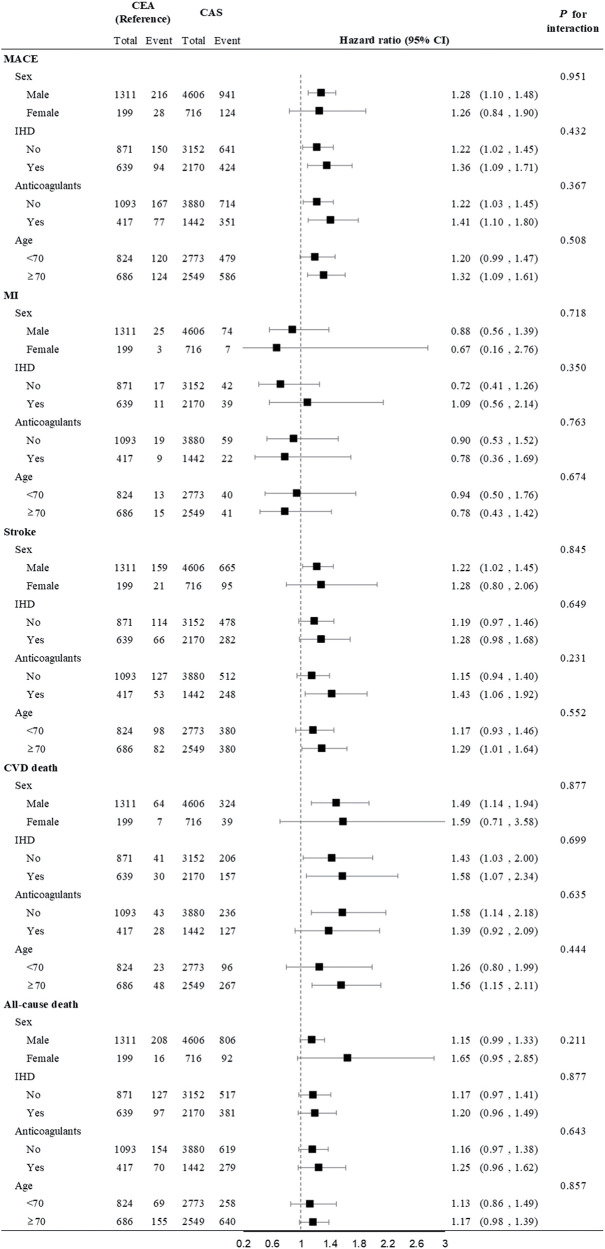 Fig. 4
Fig. 4| Mean ± SD or n (%) | Before PS matching | After PS matching | ||||
|---|---|---|---|---|---|---|
| CEA | CAS | SMD | CEA | CAS | SMD | |
| Male | 1321 (86.9) | 5744 (84.9) | 0.057 | 1311 (86.8) | 4606 (86.5) | |
| Age (years) | 68.0 ± 86.9 | 68.5 ± 9.3 | 0.050 | 68.0 (8.4) | 68.3 (9.2) | 0.027 |
| Smoking | 0.110 | 0.043 | ||||
| Never | 533 (32.5) | 2500 (36.9) | 529 (35.0) | 1900 (35.7) | ||
| Ex-smoker | 495 (32.4) | 1928 (28.5) | 489 (32.4) | 1623 (30.5) | ||
| Current | 493 (36.9) | 2340 (34.6) | 492 (32.6) | 1799 (33.8) | ||
| Alcohol consumption | 0.019 | 0.011 | ||||
| <1 time per week | 828 (54.4) | 3748 (55.4) | 822 (54.4) | 2926 (55.0) | ||
| ≥1 time per week | 693 (45.6) | 3020 (44.6) | 688 (45.6) | 2396 (45.0) | ||
| Body mass index (kg/m2) | 23.9 ± 2.9 | 23.9 ± 2.9 | 0.010 | 23.9 ± 3.0 | 23.9 ± 2.9 | 0.009 |
| HDL-cholesterol (mg/dL) | 50.0 ± 15.6 | 49.7 ± 13.5 | 0.023 | 50.0 ± 15.6 | 49.8 ± 13.1 | 0.017 |
| LDL-cholesterol (mg/dL) | 111.2 ± 41.2 | 113.6 ± 41.8 | 0.058 | 111.2 ± 40.7 | 112.1 ± 41.4 | 0.022 |
| Triglyceride (mg/dL), median (IQR) | 127 (90–185) | 132 (93–190) | 0.073 | 127 (90–185) | 130 (90–190) | 0.015 |
| Comorbidity | ||||||
| Diabetic mellitus | 561 (36.9) | 2434 (36.0) | 0.019 | 558 (37.0) | 1958 (36.8) | 0.003 |
| Hypertension | 1261 (82.9) | 5493 (81.2) | 0.046 | 1252 (82.9) | 4376 (82.2) | 0.018 |
| Atrial fibrillation | 139 (9.1) | 486 (7.2) | 0.072 | 132 (8.7) | 408 (7.7) | 0.039 |
| Dyslipidemia | 1366 (89.8) | 5821 (86.0) | 0.117 | 1356 (89.8) | 4808 (90.3) | 0.018 |
| Peripheral artery disease | 588 (38.7) | 2632 (38.9) | 0.005 | 584 (38.7) | 2060 (38.7) | 0.001 |
| Ischemic stroke or transient ischemic attack | 0.234 | 0.153 | ||||
| Asymptomatic | 438 (28.8) | 1279 (18.9) | 431 (28.5) | 1167 (21.9) | ||
| Symptomatic | 1083 (71.2) | 5489 (81.1) | 1079 (71.5) | 4155 (78.1) | ||
| Ischemic heart disease | 647 (42.5) | 2559 (37.8) | 0.097 | 639 (42.3) | 2170 (40.8) | 0.031 |
| Medication | ||||||
| Statins | 1422 (93.5) | 6092 (90.0) | 0.127 | 1412 (93.5) | 5013 (94.2) | 0.029 |
| Anticoagulants | 422 (27.7) | 1922 (28.4) | 0.015 | 417 (27.6) | 1442 (27.1) | 0.012 |
| Antiplatelets | 1516 (99.7) | 6756 (99.8) | 0.030 | 1506 (99.7) | 5319 (99.9) | 0.052 |
| CEA (n = 1510) | CAS (n = 5322) | Hazard ratio | P | |
|---|---|---|---|---|
| Event (%) | Event (%) | |||
| Within 1 month | ||||
| MACE | 77 (5.1) | 235 (4.4) | 0.86 (0.67, 1.11) | 0.239 |
| MI | 0 (0) | 7 (0.1) | — | |
| Stroke | 75 (5.0) | 183 (3.4) | 0.69 (0.53, 0.89) | 0.005 |
| CVD death | 4 (0.3) | 49 (0.9) | 3.49 (1.26, 9.68) | 0.016 |
| All-cause death | 7 (0.5) | 60 (1.1) | 2.44 (1.16, 5.35) | 0.026 |
| Within 1 year | ||||
| MACE | 140 (9.3) | 625 (11.7) | 1.27 (1.06, 1.53) | 0.011 |
| MI | 5 (0.3) | 28 (0.5) | 1.61 (0.62, 4.21) | 0.328 |
| Stroke | 123 (8.1) | 479 (9.0) | 1.11 (0.91, 1.35) | 0.318 |
| CVD death | 21 (1.4) | 168 (3.2) | 2.29 (1.45, 3.63) | <0.001 |
| All-cause death | 46 (3.0) | 279 (5.2) | 1.74 (1.28, 2.38) | 0.001 |
| Overall | ||||
| MACE | 244 (16.2) | 1065 (20.0) | 1.27 (1.11, 1.47) | 0.001 |
| MI | 28 (1.9) | 81 (1.5) | 0.86 (0.56, 1.32) | 0.486 |
| Stroke | 180 (11.9) | 760 (14.3) | 1.23 (1.04, 1.44) | 0.016 |
| CVD death | 71 (4.7) | 363 (6.8) | 1.49 (1.16, 1.92) | 0.002 |
| All-cause death | 224 (14.8) | 898 (16.9) | 1.18 (1.02, 1.36) | 0.025 |
| Asymptomatic | Symptomatic | P for | |||||||
|---|---|---|---|---|---|---|---|---|---|
| CEA | CAS | HR | P | CEA | CAS | HR | P | ||
| Event (%) | Event (%) | Event (%) | Event (%) | ||||||
| Within 1 month | |||||||||
| MACE | 2 (0.5) | 13 (1.1) | 2.40 (0.59, 9.78) | 0.220 | 75 (7.0) | 222 (5.3) |
|
| 0.113 |
| MI | 0 (0) | 4 (0.3) | — | 0 (0) | 3 (0.1) | — | — | ||
| Stroke | 2 (0.5) | 8 (0.7) | 1.47 (0.37, 5.87) | 0.582 | 73 (6.8) | 175 (4.2) |
|
| 0.223 |
| CVD death | 1 (0.2) | 1 (0.1) | 0.37 (0.02, 5.89) | 0.481 | 3 (0.3) | 48 (1.2) |
|
| 0.114 |
| All-cause death | 2 (0.5) | 2 (0.2) | 0.37 (0.05, 2.62) | 0.319 | 5 (0.5) | 58 (1.4) |
|
| 0.056 |
| Within 1 year | |||||||||
| MACE | 9 (2.1) | 32 (2.7) | 1.32 (0.64, 2.73) | 0.459 | 131 (12.1) | 593 (14.3) | 1.17 (0.97, 1.42) | 0.111 | 0.760 |
| MI | 1 (0.2) | 5 (0.4) | 1.85 (0.20, 17.01) | 0.587 | 4 (0.4) | 23 (0.6) | 1.52 (0.53, 4.41) | 0.439 | 0.877 |
| Stroke | 6 (1.4) | 18 (1.5) | 1.11 (0.46, 2.69) | 0.818 | 117 (10.8) | 461 (11.1) | 1.02 (0.83, 1.25) | 0.865 | 0.852 |
| CVD death | 4 (0.9) | 11 (0.9) | 1.02 (0.32, 3.20) | 0.980 | 17 (1.6) | 157 (3.8) |
|
| 0.172 |
| All-cause death | 10 (2.3) | 31 (2.7) | 1.14 (0.56, 2.32) | 0.709 | 36 (3.3) | 248 (6.0) |
|
| 0.251 |
| Overall | |||||||||
| MACE | 28 (6.5) | 89 (7.6) | 1.21 (0.79, 1.85) | 0.374 | 216 (20.0) | 976 (23.5) |
|
| 0.967 |
| MI | 5 (1.2) | 21 (1.8) | 1.67 (0.62, 4.51) | 0.312 | 23 (2.1) | 60 (1.4) | 0.71 (0.44, 1.14) | 0.155 | 0.126 |
| Stroke | 15 (3.5) | 46 (3.9) | 1.16 (0.65, 2.06) | 0.613 | 165 (15.3) | 714 (17.2) | 1.14 (0.96, 1.36) | 0.134 | 0.961 |
| CVD death | 12 (2.8) | 102 (8.7) | 1.03 (0.52, 2.01) | 0.941 | 59 (5.5) | 796 (19.2) |
|
| 0.305 |
| All-cause death | 46 (10.7) | 32 (2.7) | 0.87 (0.62, 1.22) | 0.415 | 178 (16.5) | 331 (8.1) |
|
| 0.089 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCerebrovascular and Carotid Artery Diseases · Cardiovascular Health and Disease Prevention · Oropharyngeal Anatomy and Pathologies
Introduction
There are 7.6 million ischemic strokes reported globally each year, resulting in 3.3 million deaths.^1)^ A prior study from the United States involving 2204 ischemic stroke patients reported that large artery atherosclerosis was the underlying cause in 16.6% of cases and that an ipsilateral 50%–99% carotid stenosis could be identified in 8% of this population.^2)^ Carotid endarterectomy (CEA) and carotid artery stenting (CAS) are both established as effective treatments for symptomatic and asymptomatic carotid artery stenosis.^3,4)^ Multiple studies have compared the outcomes of these 2 approaches. A previous systematic review of 22 randomized controlled trials (RCTs) showed that stenting for symptomatic carotid stenosis is associated with a higher risk of periprocedural stroke or death compared to endarterectomy.^5)^ However, few other reports to date have compared the clinical results of carotid revascularization for carotid stenosis in an Asian population.
The number of carotid revascularization procedures used to treat carotid stenosis is relatively lower in Korea than in Western countries, including the United States and Europe. A prior study calculated that 2800 carotid revascularization procedures were conducted in Korea in 2013, comprising 587 CEA and 2312 CAS cases.^6)^ A study from the United Kingdom, which has a population 1.3 times greater than Korea, described 4356 cases of CEA in that same year.^7)^ When comparing the rate of carotid revascularization procedures per population, the total carotid revascularization rate in Korea was 57 procedures per 1000000 persons in 2013, with CEA accounting for 11 per 1000000 persons. In contrast, based on population estimates, the CEA rate in the United Kingdom in 2013 was approximately 86 per 1000000 adults (aged 16 and older).^8)^ This stark difference highlights the lower utilization of overall carotid revascularization procedures, especially CEA, in Korea.
It is well established that the incidence of cardiovascular disease (CVD) is lower in East Asian countries than among Western populations.^9)^ We speculated, therefore, that the clinical outcomes of carotid revascularization procedures might be different between these populations. Our objective was to examine real-world data on carotid revascularizations and evaluate the clinical outcomes of CEA and CAS in a Korean cohort from the Korean National Health Insurance Service (NHIS) database.
Materials and Methods
Study design and database
This was a retrospective cohort study involving patients registered with the NHIS between 2008 and 2018. Patients who underwent CEA or CAS procedures during this period were included. Subjects who underwent CEA or CAS during the washout period (2008–2009) were excluded. Patients who received CEA or CAS 2 or more times during the study period, as well as those without clinical data in the NHIS database, were also excluded from the analysis (Fig. 1). Patient age, sex, alcohol consumption, cholesterol levels, medications, and diseases according to the 10th edition of the International Classification of Diseases Diagnostic Code (ICD-10) were investigated. This study was conducted in accordance with the principles of the Declaration of Helsinki, with approval from the Ethics Committee of Korea University Anam Hospital (2020AN0279).
Study flowchart for the comparison of patients who underwent CEA or CAS. CEA: carotid endarterectomy; CAS: carotid artery stenting
Study subjects and clinical outcomes
The included study patients were divided into CEA and CAS groups and subjected to 1:4 propensity score matching. The clinical outcomes of the 2 groups were then compared. CEA patients were defined as those entered under NHIS CEA codes O0226, O0227, O2066, and O2063. For CAS cases, the identifying code was M6602. Patients with ischemic stroke, stroke, and transient ischemic attack were defined as those assigned ICD-10 codes I63, I60–I64, and G45, who underwent a computed tomography scan or magnetic resonance imaging at the time they were assigned a disease code. Patients with myocardial infarction (MI) were defined by ICD-10 codes I21–I22, indicating that they underwent hospitalization and coronary artery angiography. CVD death was defined by ICD-10 codes ranging from I00 to I99 as the cause of death. Major adverse cardiovascular events (MACE) were defined as coronary artery disease, stroke, or CVD death. Symptomatic patients were defined as those hospitalized with ischemic stroke or transient ischemic attack within 180 days prior to carotid revascularization. The use of specific drugs was defined as medication prescribed within 1 month of the procedure.
Statistical analysis
Data are presented as means ± standard deviations or as median values (interquartile range) for continuous variables, and as numbers (percentages) for categorical variables. Demographic and clinical characteristics were compared by calculating the standardized mean difference (SMD) between the study groups. We derived propensity scores from a multiple logistic regression model that included sex, age, smoking status (current, former, or never), alcohol consumption (≥1 or <1 times/week), body mass index (BMI), high-density lipoprotein cholesterol, low-density lipoprotein cholesterol, and triglycerides, as well as comorbidities such as diabetes mellitus, hypertension, atrial fibrillation, dyslipidemia, peripheral artery disease, or ischemic heart disease, symptomatic or asymptomatic status, and the use of statins, anticoagulants, or antiplatelet agents. All SMDs between the 2 groups after propensity matching were 0.1 for baseline covariates, except for the symptomatic or asymptomatic status. The cumulative incidence of outcomes was graphically presented using a Kaplan–Meier curve. A Cox proportional hazards regression model with a robust sandwich variance estimator was used to evaluate the relationship between group and study outcomes, accounting for correlations within matched clusters. Symptomatic or asymptomatic status was included as an adjusting factor in the model. The risk of outcomes in the CAS group compared with the CEA group was presented as a hazard ratio (HR) and 95% confidence interval (CI). The same model was used to assess outcomes according to symptomatic or asymptomatic status. Baseline characteristics for subgroup analysis included sex, prior ischemic heart disease, use of anticoagulants, and age (≥75 and <70 years).
All statistical analyses were performed using SAS Enterprise Guide software, version 7.1 (SAS Institute Inc., Cary, NC, USA), and a 2-sided P value of <0.05 was considered statistically significant.
Results
Study population and characteristics
A total of 10986 patients in Korea were registered as having undergone CEA or CAS once during the study period. After excluding cases with insufficient clinical data, 1521 patients received CEA, and 6768 patients received CAS. The median follow-up period was 44 months (interquartile range, 25.1–70.5). The 2 groups differed in terms of smoking, dyslipidemia, statin medication, and the proportion of symptomatic patients in the procedure indication. In the CEA group, 28.8% of the patients were asymptomatic, whereas this proportion was only 18.9% in the CAS group (P <0.001, SMD 0.234). After propensity score matching, no statistically significant differences were found between the 2 groups in any variables, except for the proportion of symptomatic patients in the procedure indication (Table 1).
Clinical outcomes
The stroke incidence was lower in the CAS group within 1 month of the procedure (HR, 0.69; 95% CI, 0.53–0.89; P = 0.005). During the total follow-up period, however, the stroke incidence was higher among the CAS cases (HR, 1.23; 95% CI, 1.04–1.44; P = 0.016). The stroke incidence was 5.0% and 3.4% for the CEA and CAS groups within 1 month of the procedure and 11.9% and 14.3% in the total follow-up period, respectively (Fig. 2). The incidence of CVD death was higher among CAS patients both within 1 month of the procedure and during the total follow-up period (HR, 3.49; 95% CI, 1.26–9.68; P = 0.016 and HR, 1.49; 95% CI, 1.16–1.92; P = 0.002, respectively). All-cause mortality was also higher in the CAS group within 1 month of the procedure and during the total follow-up period (HR, 2.44; 95% CI, 1.16–5.35; P = 0.026 and HR, 1.18; 95% CI, 1.02–1.36; P = 0.025, respectively) (Table 2).
Stroke incidence in the total study cohort of patients who underwent carotid revascularization. (A) Cumulative incidence of stroke in CEA patients (solid line) and CAS patients (dotted line) within 1 month. (B) Cumulative incidence of stroke in CEA patients (solid line) and CAS patients (dotted line) within 1 year. (C) Cumulative incidence of stroke in CEA patients (solid line) and CAS patients (dotted line) during the total follow-up period. CEA: carotid endarterectomy; CAS: carotid artery stenting
Symptomatic and asymptomatic patients
Our study patients were further divided into symptomatic and asymptomatic groups. No differences were observed in the clinical outcomes between the symptomatic cases in the CEA and CAS groups, except for stroke occurrence within 1 month, which was lower in the CAS group (HR, 0.61; 95% CI, 0.47–0.80; P < 0.001). The stroke rates were 6.8% and 4.2% for CEA and CAS, respectively. There was no difference in stroke occurrence between CEA and CAS in the 1-year outcome and total follow-up periods (Fig. 3). The incidence of CVD death among symptomatic patients was higher in the CAS group than in the CEA group at all time points, including 1 month, 1 year, and over the entire follow-up period (HR, 4.18; 95% CI, 1.30–13.43; P = 0.016 at 1 month; HR, 2.43; 95% CI, 1.47–4.03; P = 0.001 at 1 year; and HR, 1.50; 95% CI, 1.14–1.97; P = 0.004 for the total follow-up; Table 3).
Stroke incidence in symptomatic and asymptomatic patients who underwent carotid revascularization. (A) Cumulative incidence of stroke in symptomatic (red solid line) and asymptomatic (blue solid line) CEA patients and symptomatic (red dotted line) and asymptomatic (blue dotted line) CAS patients within 1 month. (B) Cumulative incidence of stroke in symptomatic (red solid line) and asymptomatic (blue solid line) CEA patients and symptomatic (red dotted line) and asymptomatic (blue dotted line) CAS patients within 1 year. (C) Cumulative incidence of stroke in symptomatic (red solid line) and asymptomatic (blue solid line) CEA patients and symptomatic (red dotted line) and asymptomatic (blue dotted line) CAS patients within the total follow-up period. CEA: carotid endarterectomy; CAS: carotid artery stenting
Variables affecting clinical outcomes
When subgroup analysis was performed, ischemic heart disease and pre-procedure anticoagulation were found not to affect the incidence of MACE (P for interaction = 0.432 and 0.367, respectively). Old age (>70 years) did not affect the occurrence of MACE or stroke (P for interaction = 0.508 and 0.552, respectively), but CAS was associated with worse outcomes in this age category in terms of MACE, stroke, and CVD death (Fig. 4).
Forest plot of subgroup analysis with outcomes including MACE and all-cause death. MACE: major adverse cardiovascular event
Discussion
The findings of our study have revealed that the incidence of stroke is higher during the periprocedural period (within 1 month) in symptomatic patients who underwent CEA, but that the rates of mortality and CVD death were lower in both the early and long-term follow-up periods compared to symptomatic patients who underwent CAS. The results were similar in all patients, including both symptomatic and asymptomatic cases, who underwent a carotid revascularization procedure. However, the incidence of MACE and mortality rates did not differ between the CEA and CAS groups among asymptomatic patients.
As mentioned above, a number of RCTs comparing CEA and CAS in the treatment of carotid artery stenosis have been conducted, with some conflicting results.^5)^ A prior meta-analysis of 1-month outcomes in 10 RCTs comparing CAS and CEA found that CAS was associated with higher rates of any stroke.^10)^ In contrast, our study found that the CEA group in symptomatic patients had a higher incidence of stroke within 1 month. Similar results were also reported in another large-scale study of 430000 patients from the Nationwide Readmissions Database in the United States. In that study, CEA patients had a higher rate of periprocedural stroke than CAS cases but a lower rate of overall inpatient mortality.^11)^ These discrepancies may be due to various confounding factors. Compared with the results reported by the CREST trial (Carotid Revascularization Endarterectomy Versus Stenting Trial), a large RCT conducted in 2010, the periprocedural symptomatic stroke risk with CEA in our study was considerably higher (3.2% in the CREST population versus 6.8% in our cohort).^3)^ The periprocedural stroke incidence of CEA may be largely influenced by intra-procedural complications, including technical errors.^12)^ The poor 1-month stroke incidence of CEA observed in our cohort might have been due to the objectively higher procedural stroke risk in the CEA group. These early poor outcomes of CEA in our series may be attributed to a lack of trained vascular surgeons and the limited number of high-volume vascular centers in Korea. As of 2022, according to the Korean Surgical Society, there were only 138 authorized vascular surgeons in Korea. Several previous studies have suggested that higher surgical volume is associated with lower complication rates in CEA and that the surgeon’s specialty may also influence outcomes.^13–15)^ The improved outcomes in terms of 30-day mortality and stroke rates in our CAS patients may have contributed to the superior early outcomes in this group compared to the CEA group. Other studies have reported that the 30-day mortality and stroke rates following CAS have improved over the past 10 to 15 years.^11,16,17)^ Similarly, in our study, the periprocedural stroke rates in symptomatic patients who underwent CAS were lower than those reported in the CREST study (5.5% vs. 4.2%).^3)^ In conclusion, it is believed that the poor outcomes of CEA, driven by the shortage of vascular surgeons in Korea, along with improvements in CAS outcomes, contributed to the higher early stroke risk observed in our study. However, in terms of 1-year outcomes, the stroke risk was not significantly different between the 2 study groups, consistent with findings from other studies. In a pooled analysis of the 4 largest RCTs, the long-term incidence of stroke, beyond the periprocedural period, was found to be similar between the 2 revascularization procedures.^18)^
Unlike stroke risk, the rates of all-cause death and CVD death were higher in our symptomatic CAS group during both the early and long-term follow-up periods. These findings are consistent with previous RCTs, which reported that CAS was associated with higher post-procedural rates of death and MI, and that periprocedural MI contributed to increased long-term mortality.^10)^ The higher mortality observed in our symptomatic CAS group may be attributed to the relatively higher pre-procedural comorbidity among these patients. Although no significant differences were observed in the baseline characteristics between the 2 groups in our study, the number of comorbidities included in our analysis was limited, making an accurate comparison of comorbidity and surgical risk between the 2 groups difficult. However, many clinicians generally prefer CAS over CEA in patients who are at high surgical risk.^19)^ Similarly, in a previous study, the proportion of patients with extreme or major mortality risk prior to the procedure was higher among CAS patients compared to CEA patients.^11)^
In asymptomatic patients, no significant difference was observed between the 2 carotid revascularization methods. These findings are consistent with those of a previous study using a German mandatory registry, which analyzed 104000 individuals and found no major difference in the risk of disabling stroke or death, or any stroke or death.^20)^ Therefore, the choice of revascularization method should be individualized for asymptomatic patients.^21)^
In further subgroup analysis stratified by age (≥70 years), we found that age was not a contributing factor to differences in outcomes between the CAS and CEA groups. However, in subjects older than 70 years, we observed that the incidence of MACE, stroke, and CVD death was higher in the CAS group. This result is consistent with previous findings from the Carotid Stenosis Trialists’ Collaboration, which reported that age >70 years is associated with higher perioperative stroke rates after CAS, but not after CEA. This may be due to an increased atherosclerotic burden, aortic arch calcification, challenges in vascular anatomy, and greater plaque vulnerability.^4,22,23)^
Another subgroup analysis showed no interaction effects of anticoagulant use between the 2 groups. Recently, several studies have reported the beneficial effects of anticoagulants in atherosclerotic disease.^24,25)^ Notably, the Cardiovascular Outcomes for People Using Anticoagulation Strategies (COMPASS) trial found that a daily combination of low-dose rivaroxaban and 100 mg aspirin significantly lowered the rate of stroke, MI, or cardiovascular death.^25)^ However, an analysis within COMPASS of 1919 patients with carotid disease revealed that a higher dose of rivaroxaban did not reduce major vascular events in these patients but increased the risk of major bleeding.^25)^ Similarly, our current subgroup analysis found that anticoagulant use did not impact outcomes between the CAS and CEA groups. Further trials on the use of anticoagulants for carotid stenosis are needed.
This study was a nationwide, population-based analysis using patients registered in the Korean NHIS database. Unlike previous large studies that analyzed only Western populations, our findings are likely applicable to other East Asian countries due to commonalities in several ethnic and demographic characteristics, such as lower BMI and the unique epidemiology of CVD, both of which differ from those in Western populations.^9,26)^ Therefore, our study provides valuable information on the clinical outcomes of carotid stenosis treated with 2 different revascularization methods in Asian populations.
The number of carotid revascularization procedures increased in Korea during our study period (2010–2018). The total number of procedures in our study series, including both CAS and CEA cases, rose from 349 in 2010 to 1564 in 2018. These findings may also be valuable for clinicians in developing countries where carotid revascularization cases are increasing. Lastly, with higher surgical volumes and growing surgeon experience, better clinical outcomes are expected, and further studies are needed to confirm these trends.
There were several limitations of our study. First, patients who underwent transcarotid artery revascularization with flow reversal (TCAR), a novel hybrid procedure, were not included in the current analysis because this treatment is not yet available in Korea. Although no RCTs have compared TCAR with other carotid revascularization methods, a systematic review of TCAR involving 18 observational studies reported low 30-day rates of stroke, MI, and death.^27)^ Second, several pieces of clinical information that could have impacted our findings were not included in the analysis due to data limitations in the Korean NHIS database. Specifically, we were unable to assess pre-procedural tandem lesions or the laterality of post-procedure stroke, which may have influenced outcomes such as stroke incidence and cardiovascular death.
Conclusion
Our population-based analysis of patients in the Korean NHIS database found that in symptomatic carotid stenosis patients, the periprocedural stroke rate was higher after CEA, while the mortality rate was higher after CAS, both in the early postoperative stages and over the long term. In asymptomatic patients, however, the incidences of MACE and mortality were comparable between CEA and CAS. Further studies are needed as surgical volume increases and surgical/clinical experience with both CEA and CAS continues to grow.
Declarations
Consent for publication
This manuscript does not contain any individual person’s data in any form.
Ethics approval and consent to participate
This study was conducted in accordance with the principles of the Declaration of Helsinki and was approved by the Ethics Committee of Korea University Anam Hospital (2020AN0279). Informed consent from patients was waived due to the retrospective design of the study.
Funding
This study was supported by a grant from Asan Institute for Life Sciences and Corporate Relations of Asan Medical Center, Seoul, Korea.
Data availability
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Author contributions
Data collection, data analysis, writing: SAL
Data collection, data analysis, writing: DHC
Data collection, data analysis: JMC
Study design, data collection, data analysis, writing: JGG
All authors have reviewed and approved the final version of this manuscript.
Disclosure statement
The authors declare that they have no competing interests.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1GBD 2019 Stroke Collaborators. Global, regional, and national burden of stroke and its risk factors, 1990–2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet Neurol 2021; 20: 795–820.34487721 10.1016/S 1474-4422(21)00252-0PMC 8443449 · doi ↗ · pubmed ↗
- 2Flaherty ML Kissela B Khoury JC Carotid artery stenosis as a cause of stroke. Neuroepidemiology 2013; 40: 36–41.23075828 10.1159/000341410 PMC 3626492 · doi ↗ · pubmed ↗
- 3Brott TG Hobson RW 2nd Howard G Stenting versus endarterectomy for treatment of carotid-artery stenosis. N Engl J Med 2010; 363: 11–23.20505173 10.1056/NEJ Moa 0912321 PMC 2932446 · doi ↗ · pubmed ↗
- 4Naylor A Rantner B Ancetti S European society for vascular surgery (ESVS) 2023 Clinical practice guidelines on the management of atherosclerotic carotid and vertebral artery disease. Eur J Vasc Endovasc Surg 2023; 65: 7–111.35598721 10.1016/j.ejvs.2022.04.011 · doi ↗ · pubmed ↗
- 5Muller MD Lyrer P Brown MM Carotid artery stenting versus endarterectomy for treatment of carotid artery stenosis. Cochrane Database Syst Rev 2020; 2: CD 000515.32096559 10.1002/14651858.CD 000515.pub 5PMC 7041119 · doi ↗ · pubmed ↗
- 6Cho SS Joh JH Ahn HJ National trends in carotid endarterectomy and stenting in Korea from 2004 to 2013. Exp Ther Med 2016; 12: 2639–43.27698767 10.3892/etm.2016.3637 PMC 5038473 · doi ↗ · pubmed ↗
- 7Johal AS Loftus IM Boyle JR Changing patterns of carotid endarterectomy between 2011 and 2017 in England. Stroke 2019; 50: 2461–8.31327312 10.1161/STROKEAHA.119.025231 · doi ↗ · pubmed ↗
- 8Office for National Statistics. Population estimates for the UK, England and Wales, Scotland and Northern Ireland: mid-2013 [Internet]. London: Office for National Statistics; 2014 Oct 23 [cited 2025 Apr 28]. Available from: https://www.ons.gov.uk/peoplepopulationandcommunity/populationandmigration/populationestimates/bulletins/annualsmallareapopulationestimates/2014-10-23.