Detection of Sentinel Lymph Node in Endometrial Cancer Using 99m Tc-Nanocolloid SPECT/CT: A Retrospective Cohort Study
Raydel BrianKwee Amalo, Endah Indriani, Hendra Budiawan, Budi Darmawan, Basuki Hidayat

TL;DR
This study shows that using 99m Tc-nanocolloid SPECT/CT helps detect sentinel lymph nodes in early-stage endometrial cancer with high accuracy and matches surgical findings.
Contribution
Demonstrates the effectiveness of 99m Tc-nanocolloid SPECT/CT for sentinel lymph node mapping in endometrial cancer with high detection rates and surgical concordance.
Findings
SLNs were detected in 76.9% of patients using SPECT/CT with 100% agreement with gamma probe results.
Larger tumors (>4 cm) were more frequently associated with positive SLNs.
SPECT/CT count intensity did not correlate with histopathological metastasis.
Abstract
Background Sentinel lymph node mapping (SLNM) using 99m Tc-nanocolloid single photon emission tomography/computed tomography (SPECT/CT) is a minimally invasive technique for detecting lymphatic metastasis in early-stage endometrial cancer. This study aimed to evaluate the detection rate (DR) of sentinel lymph nodes (SLNs) using SPECT/CT and compare the findings with intraoperative gamma probe evaluation and histopathological results. Methods A retrospective cohort study was conducted at Dr. Hasan Sadikin General Hospital, Bandung, Indonesia, between December 2022 and January 2024. Twenty-six patients with FIGO (International Federation of Gynecology and Obstetrics) stage I endometrial cancer were included. 99m Tc-nanocolloid was injected into four cervical quadrants, followed by SPECT/CT imaging and intraoperative gamma probe evaluation. Histopathological analysis was performed to…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
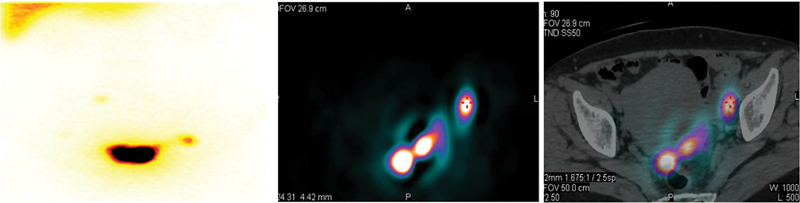 Fig. 1
Fig. 1| Age, mean (range), y | 54.19 (29–71) |
|
Type of tumor,
| |
| Endometrioid endometrial carcinoma | 25 (96.2) |
| Carcinosarcoma | 1 (3.8) |
|
Sentinel lymph node,
| |
| Positive | 20 (76.9) |
| Negative | 6 (23.1) |
|
Histopathology,
| |
| Metastasis | 4 (15.4) |
| Locations SLN | Frequency |
|---|---|
| External iliac | 9 |
| Internal iliac | 8 |
| Common iliac | 3 |
| Obturator bilateral | 2 |
| Para-aorta | 1 |
| SLN detection | SPECT/CT | Intraoperative gamma probe | Histopathology metastasis |
|---|---|---|---|
| Positive | 20 (76.9%) | 20/20 (100%) | 4/20 (20%) |
| Negative | 6 (23.1%) | 0/6 | 0/6 |
| Patients | Tumor size (cm) | Sentinel lymph node | Metastasis | |
|---|---|---|---|---|
| 1 | 4.5 | Positive | No | < 0.001 |
| 2 | 4 | Positive | No | |
| 3 | 2 | Negative | No | |
| 4 | 7 | Positive | Yes | |
| 5 | 1.5 | Negative | No | |
| 6 | 9.5 | Positive | No | |
| 7 | 4 | Negative | No | |
| 8 | 4 | Positive | Yes | |
| 9 | 5 | Positive | No | |
| 10 | 5 | Positive | No | |
| 11 | 4 | Positive | No | |
| 12 | 4 | Positive | No | |
| 13 | 5 | Positive | No | |
| 14 | 3.5 | Negative | No | |
| 15 | 5 | Positive | No | |
| 16 | 2 | Negative | No | |
| 17 | 4 | Positive | No | |
| 18 | 4 | Positive | Yes | |
| 19 | 4 | Positive | No | |
| 20 | 8 | Positive | No | |
| 21 | 5 | Positive | No | |
| 22 | 4 | Positive | Yes | |
| 23 | 5 | Positive | No | |
| 24 | 4 | Positive | No | |
| 25 | 4 | Positive | No | |
| 26 | 1 | Negative | No |
| Patients | Max count | |
|---|---|---|
| 1 | 4,944 | 0.156 |
| 2 | 1,705 | |
| 3 | 4,621 | |
| 4 | 3,424 | |
| 5 | 8,441 | |
| 6 | 7,202 | |
| 7 | 4,140 | |
| 8 | 5,191 | |
| 9 | 1,455 | |
| 10 | 936 | |
| 11 | 833 | |
| 12 | 58 | |
| 13 | 1,434 | |
| 14 | 42 | |
| 15 | 557 | |
| 16 | 667 | |
| 17 | 1,677 | |
| 18 | 1,504 | |
| 19 | 540 | |
| 20 | 670 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsEndometrial and Cervical Cancer Treatments · Ovarian cancer diagnosis and treatment · Angiogenesis and VEGF in Cancer
Background
Endometrial cancer (EC) is the most common gynecologic malignancy in high- and middle-income countries. 1 In Indonesia, this cancer is frequently diagnosed at an advanced stage, although a significant proportion of cases are detected at early stages. Patients diagnosed at an early stage have a favorable prognosis, with a 5-year survival rate exceeding 95%. 2
The lymphatic system of the uterine corpus comprises three primary lymphatic pathways: the utero-ovarian, parametrial, and presacral pathways. 3 Sentinel lymph node mapping (SLNM) is a minimally invasive surgical approach used in early-stage EC to identify the sentinel lymph node (SLN), which represents the first site of potential lymphatic metastasis. SLNM serves as an alternative to conventional radical lymphadenectomy, thereby reducing the need for extensive surgical intervention in early-stage patients. 4 This procedure typically uses a planar gamma camera 1 day before surgery and a gamma probe during surgery; however, it is often associated with a low detection rate (DR). 5 A negative SLN histopathology result indicates the absence of metastasis in other lymph nodes, thus eliminating the need for radical lymphadenectomy. 6
^99m^ Tc-nanocolloid, with a particle size ranging from 5 to 100 nm and a diameter of ≤ 80 nm, facilitates easy migration into the lymphatic system. 4 The injection sites may vary, including subserosal/fundal, myometrial, and cervical locations. 7 This study is the first of its kind conducted in Indonesia, specifically at Dr. Hasan Sadikin General Hospital, Bandung, Indonesia. It aimed to evaluate the DR of positive SLNs in EC patients using SLNM with ^99m^ Tc-nanocolloid single photon emission tomography/computed tomography (SPECT/CT), compared to intraoperative gamma probe evaluation.
Materials and Methods
Study Design and Participants
A retrospective cohort study was conducted at the Department of Nuclear Medicine, Dr. Hasan Sadikin General Hospital, between December 2022 and January 2024. During this period, a total of 28 patients with EC were referred to the Department of Nuclear Medicine. All included patients were diagnosed with FIGO (International Federation of Gynecology and Obstetrics) stage I EC. Two patients were excluded based on histopathological results, which confirmed a diagnosis of cervical cancer.
Imaging Protocol
^99m^ Tc-nanocolloid (37 MBq per injection, total dose 148 MBq) was administered into the four cervical quadrants under sterile conditions 1 day prior to surgery. Each injection had a volume of 0.5 mL, resulting in a total injected volume of 2.0 mL. SPECT/CT imaging was performed 1 to 3 hours postinjection using a dual-head gamma camera (model) equipped with low-energy, high-resolution collimators. The acquired imaging data were analyzed to identify SLNs. On the following day, intraoperative gamma probe evaluation was performed to confirm SLN localization. The maximum counts obtained from SPECT/CT imaging were subsequently compared with histopathological findings.
Statistical Analysis
SPSS version 29.0 (IBM SPSS Statistics, Armonk, New York, United States) was used for statistical analysis. The Shapiro–Wilk test was applied to assess normality. Numerical and categorical data were analyzed using the Mann–Whitney U test. A p -value of < 0.05 was considered statistically significant.
Results
This study included 26 patients aged 29 to 71 years (mean age: 54.19 years). The majority of patients (96.2%) had endometrioid endometrial carcinoma ( Table 1 ). SLNs were detected in 20 patients (76.9%) using SPECT/CT and these findings were confirmed in all cases by intraoperative gamma probe evaluation. No SLNs were detected in six patients (23.1%). Histopathological analysis revealed metastases in 4 out of 26 patients (15.4%). Among the identified SLNs, the most common locations were along the external iliac vessels ( Table 2 ).
In the comparison of SPECT/CT results, intraoperative gamma probe detection, and histopathology in the 20 patients with positive SLNs, metastases were identified in four cases (20%) ( Table 3 ). A significant correlation was observed between tumor size and SLN detection ( p < 0.001) ( Table 4 ). Specifically, SLNs were detected in 20 patients with tumor sizes ranging from 4 to 9.5 cm, whereas all six patients with negative SLN detection had tumor sizes between 1 and 4 cm ( Table 4 ). Metastatic SLNs were identified in patients with tumor sizes > 4 cm (three cases) and 7 cm (one case). These tumors ranged from 4 to 7 cm, suggesting a potential association between tumor size and metastatic SLNs ( Table 4 ).
However, statistical analysis revealed no significant correlation between maximum SPECT/CT counts and histopathological metastases ( p = 0.156) ( Table 5 ). Among the four patients with metastatic SLNs, the maximum SLN count ranged from 1,434 to 8,441. Notably, some patients with high SLN counts did not exhibit metastases, indicating that high radiotracer uptake alone is not predictive of metastatic involvement.
Discussion
Uterine corpus cancer accounted for nearly 13,000 deaths in the United States in 2023. 8 Endometrioid carcinoma is the most common histological subtype of uterine corpus cancer. 9 In this study, the mean age of the patients was 54.19 years, with 21 patients (80.8%) over 45 years of age. The risk of developing EC has been reported to increase with age. 10 Consistent with the literature, the most common type of carcinoma in this study was endometrioid endometrial carcinoma, accounting for 96.2% of cases. 11 Endometrial carcinosarcoma, a rare and aggressive subtype, had a reported prevalence of 5.6% among all endometrial carcinomas. 12 Endometrioid endometrial carcinoma is more prevalent than other subtypes due to its strong association with hormonal factors, particularly estrogen, which stimulates the uncontrolled growth of endometrial cells. 13 Carcinosarcoma, on the other hand, is a rare and aggressive tumor characterized by the presence of both epithelial (carcinoma) and mesenchymal (sarcoma) components. 14 The external iliac region was the most common location for SLNM, consistent with previous studies. 15 The external iliac region is located on one of the major lymphatic drainage routes and is adjacent to the parametrial and presacral nodes. Lymphatic drainage from the uterine body typically passes through the external iliac nodes before spreading to the internal iliac and para-aortic nodes. In this study, the DR using ^99m^ Tc-nanocolloid SPECT/CT was 76.9%. All SLNs identified as positive on SPECT/CT were confirmed intraoperatively using a gamma probe (100% concordance). This method improved anatomical localization and detection compared to planar imaging, which, in other studies, showed a lower DR. 5 Among the six patients with negative sentinel node findings on SPECT/CT, all underwent lymphadenectomy based on intraoperative observations, and no metastasis was found in these cases. As shown in Table 4 , the six patients with negative SLNs had tumor sizes less than 4 cm. Using the Mann–Whitney U test, the relationship between tumor size and sentinel node detection was analyzed, showing a significant correlation ( p < 0.001). In a study published by Jin et al, it was stated that tumor size ≥ 2 cm in EC is significantly associated with lymphovascular space invasion (LVSI), lymph node metastasis, recurrence, and worse overall survival. Other studies have also reported that smaller tumors are associated with lower rates of lymphovascular invasion (LVI) and reduced involvement of SLNs, suggesting a lower likelihood of sentinel node positivity. 16 17 According to a study by Zhu et al, a tumor size greater than 2 cm is often considered a risk factor for metastasis. However, the histological grade of the tumor and the stage of the cancer also significantly influence the likelihood of lymph node metastasis. In endometrioid EC grades 1 and 2 (a less aggressive form of cancer), although the tumor size is larger, the risk of lymph node metastasis may be lower, especially if there is no deep myometrial invasion or LVSI. 18 In low-grade EC (grade 1 or 2), although the tumor size is larger than 2 cm, the less aggressive biological behavior of the tumor may prevent metastasis, even when the tumor exceeds the size typically associated with metastatic risk. 18 In this study, tumor size > 4 cm was associated with positive SLNs. Furthermore, given that tumor size ≥ 2 cm is significantly associated with lymph node metastasis, it is crucial to evaluate the outcomes of the four patients in the negative SPECT/CT group who had tumors ≥ 2 cm. Upon follow-up, these patients showed no signs of disease progression or lymph node involvement. However, a longer follow-up period is necessary to determine the true negative predictive value of SPECT/CT in these cases.
Tumor size in EC is an important prognostic factor, although it is not always directly correlated with lymph node metastasis. Larger tumors often indicate more advanced disease, increasing the likelihood of local spread and necessitating more intensive treatment. However, not all large tumors result in metastasis, as other factors such as histologic grade, myometrial invasion, and clinical condition also influence prognosis and treatment decisions. 19 In breast cancer, smaller tumors are similarly associated with a lower risk of SLN metastasis due to their less aggressive nature, lower LVI, and the potential for stronger immune responses that inhibit metastatic spread. 20 21
No significant correlation was observed between the maximum SPECT/CT counts and histopathological metastasis ( p = 0.156). This may be attributed to the biological heterogeneity of EC, which can lead to varying levels of radiotracer uptake and inconsistent SPECT/CT maximum values. 22 Tumor heterogeneity is a well-documented challenge in EC, as differences in tumor grade, histology, and molecular profiles can influence radiotracer uptake and imaging results. Consequently, SPECT/CT maximum counts alone may not reliably predict metastatic involvement, and histopathological confirmation remains essential for accurate staging. 9 22 However, in patients with histopathologically confirmed metastasis, the maximum SPECT/CT counts exceeded 1,000.
In Fig. 1 , an example is provided of a patient with EC who had SLNs identified in the left internal iliac lymph node, with a maximum count of 8,441 on SPECT/CT and a tumor size of 4 cm.
Localization of sentinel lymph nodes on single photon emission tomography/computed tomography (SPECT/CT) images in endometrial cancer patients.
Limitations and Suggestions
Small sample size : The study included only 26 patients, which may limit the generalizability of the results to a broader population.
Tumor biology variation : The heterogeneity of EC biology results in variation in radiotracer uptake, which may affect the relationship between maximum SPECT/CT values and histopathology results.
Conclusion
This study demonstrates that SLNM using ^99m^ Tc-nanocolloid SPECT/CT achieves a DR of 76.9%, with intraoperative confirmation using a gamma probe reaching 100%. This method improves anatomical localization accuracy compared to conventional planar imaging. Although no significant correlation was observed between maximum SPECT/CT counts and histopathological metastasis, SLN detection was significantly associated with tumor size ( p < 0.001). These findings support the use of SPECT/CT as a complementary tool in the management of early-stage EC.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Koskas M Amant F Mirza M R Creutzberg C L Cancer of the corpus uteri: 2021 update Int J Gynaecol Obstet 2021155(Suppl 1, Suppl 1):456034669196 10.1002/ijgo.13866 PMC 9297903 · doi ↗ · pubmed ↗
- 2ESMO Guidelines Committee. Electronic address: [email protected] Oaknin A Bosse T J Creutzberg C L Endometrial cancer: ESMO Clinical Practice Guideline for diagnosis, treatment and follow-up Ann Oncol 2022330986087735690222 10.1016/j.annonc.2022.05.009 · doi ↗ · pubmed ↗
- 3Sumita M Bindiya G Recent Advances in Endometrial Cancer Singapore Springer Singapore 2020
- 4Volterrani D Erba P A CarrióI Strauss H W Mariani G Nuclear Medicine Textbook: Methodology and Clinical Applications Cham Springer 2019
- 5Jankulovska A Stoilovska Rizova B Bozhinovska N Preoperative detection of sentinel lymph node in patients with endometrial cancer - comparison of planar lymphoscintigraphy, spect and SPECT/CT Nucl Med Rev Cent East Eur 2022250210110435929122 10.5603/NMR.a 2022.0022 · doi ↗ · pubmed ↗
- 6Sicignano M Mansi LG. Mariani, S. Vidal-Sicart, R.A. Valdes Olmos (Eds): Atlas of Lymphoscintigraphy and Sentinel Node Mapping, Second Edition Eur J Nucl Med Mol Imaging 2021481133453346
- 7Collarino A Vidal-Sicart S Olmos R AV Nuclear medicine manual on gynaecological cancers and other female malignancies 2022. 10.1007/978-3-031-05497-6
- 8Siegel R L Miller K D Wagle N S Jemal A Cancer statistics, 2023 CA Cancer J Clin 20237301174836633525 10.3322/caac.21763 · doi ↗ · pubmed ↗