Laparoscopic Gastrectomy for Heterotopic Pancreas with Concurrent Gastroduodenal Invagination and Gastric Wall Abscess: A Case Report
Junki Fukuda, Akira Shibata, Ryosuke Ohashi, Yuma Hane, Takahiro Saito, Kohei Nishigami, Naoto Senmaru, Miri Fujita, Satoshi Hirano

TL;DR
This case report describes a rare instance of a stomach condition involving abnormal pancreatic tissue, treated successfully with laparoscopic surgery.
Contribution
The first reported case of laparoscopic distal gastrectomy for GHP with gastroduodenal invagination and gastric wall abscess.
Findings
Laparoscopic distal gastrectomy successfully treated a 46-year-old man with GHP and gastric complications.
Histopathology confirmed the presence of pancreatic tissue and a gastric wall abscess.
The patient had a favorable recovery and was discharged 11 days post-surgery.
Abstract
Heterotopic pancreas refers to pancreatic tissue located outside its normal position and lacking anatomical or vascular continuity with the pancreas. Gastric heterotopic pancreas (GHP) is generally asymptomatic, but in rare cases large GHP lesions can cause gastric outlet syndrome or gastroduodenal invagination. GHP may also occasionally cause acute pancreatitis and abscess formation in the gastric wall. This report describes a rare case of GHP with concurrent gastroduodenal invagination and gastric wall abscess treated via laparoscopic distal gastrectomy. A 46-year-old man was admitted to the hospital with abdominal pain and vomiting. Computed tomography revealed a 40-mm low-density mass in the gastric pylorus, and gastroduodenal invagination. Gastroscopy confirmed a submucosal lesion at the gastric pylorus causing pyloric stenosis. The patient underwent laparoscopic distal…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
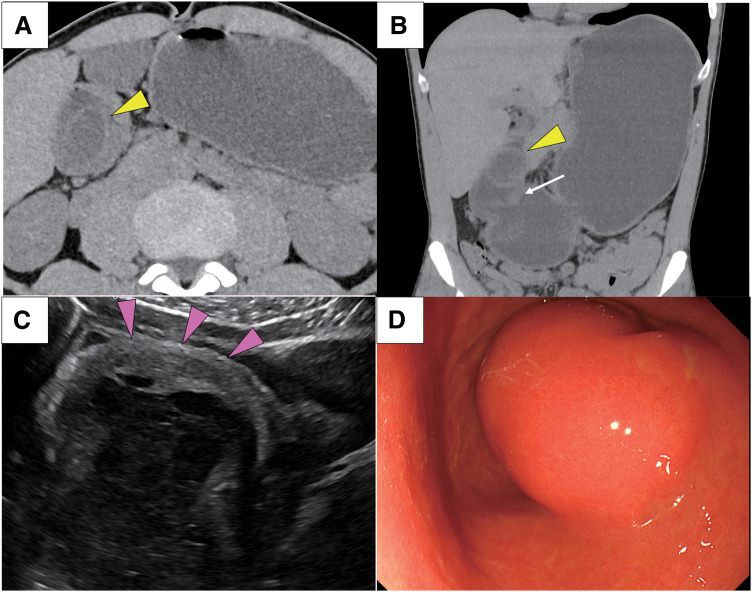 Fig. 1
Fig. 1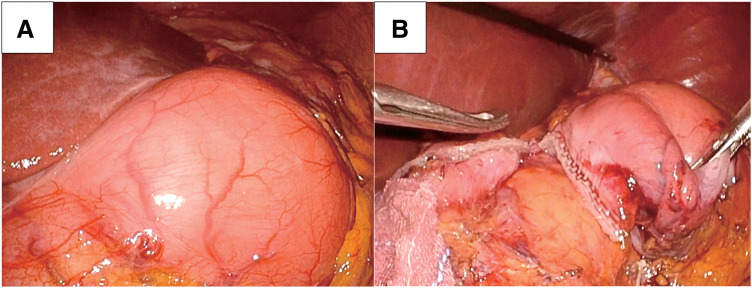 Fig. 2
Fig. 2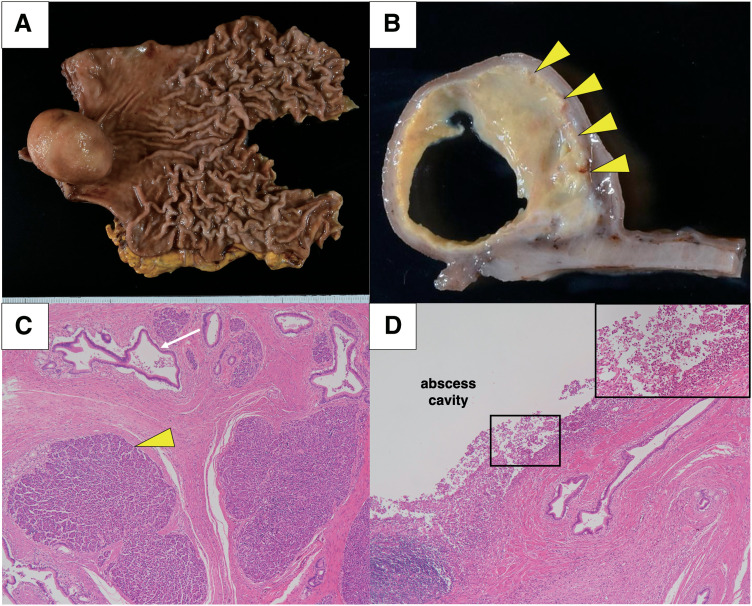 Fig. 3
Fig. 3| First author | Age/sex | Symptoms | Size | Invagination | Surgical | Heinrich’s | Pancreatitis | Gastric wall |
|---|---|---|---|---|---|---|---|---|
| Huang (2002) | 41/M | Abdominal pain | 25 | No | Open subtotal gastrectomy | II | No | No |
| Huang (2002) | 53/M | Abdominal pain | 20 | No | Open subtotal gastrectomy | ND | No | No |
| Ikematsu (2003) | 26/F | Abdominal pain, vomiting | 50 | No | Open distal gastrectomy | I | No | No |
| Ayantunde (2006) | 48/F | Vomiting | 25 | No | Laparoscopic anterior gastrectomy | ND | No | No |
| Christodoulidis (2007) | 40/F | Abdominal pain, vomiting | 50 | No | Open wedge gastrectomy | I | No | No |
| Jiang (2008) | 46/F | Abdominal pain, vomiting | 20 | No | Open distal gastrectomy | II | No | No |
| Trifan (2012) | 31/M | Abdominal pain, vomiting | 35 | No | Open distal gastrectomy | I | Yes | No |
| Iwahashi (2019) | 40/M | Abdominal pain, vomiting | 60 | Yes | Open distal gastrectomy | III | No | No |
| Xiong (2020) | 44/F | Abdominal distension | 40 | No | Open distal gastrectomy | III | No | No |
| Bejiga (2022) | 45/M | Vomiting | ND | No | Open distal gastrectomy | ND | No | No |
| Mirzaie (2023) | 43/M | Abdominal pain, vomiting | 40 | No | Laparoscopic distal gastrectomy | II | No | No |
| Current case (2025) | 46/M | Abdominal pain, vomiting | 40 | Yes | Laparoscopic distal gastrectomy | II | Yes | Yes |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGastrointestinal disorders and treatments · Pancreatitis Pathology and Treatment · Intestinal Malrotation and Obstruction Disorders
Abbreviations
GHP gastric heterotopic pancreas HP heterotopic pancreas
INTRODUCTION
Heterotopic pancreas (HP) is defined as the presence of pancreatic tissue outside its normal location, and without anatomical and vascular continuity with the main body of the pancreas.^1)^ It is usually asymptomatic and detected incidentally via imaging, but it can become symptomatic when complicated by obstruction, inflammation, bleeding, or malignant transformation. When a gastric HP (GHP) lesion is particularly large, in rare cases it may cause gastric outlet syndrome or gastroduodenal invagination, resulting in abdominal pain and vomiting.^1–10)^ Patients with GHP can also occasionally develop acute pancreatitis leading to abscess formation in the stomach wall.^11–13)^ Herein we report a rare case of laparoscopic distal gastrectomy for GHP with concurrent gastroduodenal invagination and gastric wall abscess.
CASE PRESENTATION
A 46-year-old man presented to the emergency department with abdominal pain and vomiting. He was a heavy drinker, consuming approximately 100 g of alcohol daily, and a heavy smoker, having smoked 20 cigarettes daily for the past 25 years. On physical examination, he exhibited upper quadrant pain and no rebound pain. Laboratory tests revealed elevated inflammatory markers, including white blood cell count 17900/μL and C-reactive protein 1.38 mg/dL. Abdominopelvic computed tomography revealed a 40-mm low-density mass that extended beyond the pyloric ring and descended into the duodenal bulb (Fig. 1A, 1B). Ultrasonography depicted a 40-mm mass with fluid accumulation arising from the gastric submucosa (Fig. 1C). The stomach was markedly dilated due to gastroduodenal invagination, thus the patient was urgently admitted to the hospital after placement of a gastric tube. The next day, gastric fiber revealed a submucosal lesion on the posterior wall of the gastric pylorus. Gastroduodenal invagination was relieved by gastric tube decompression, but pyloric stenosis due to a large lesion was still present (Fig. 1D). Based on these findings, the preoperative differential diagnosis was submucosal cystic tumor of gastric origin, including malignant lymphoma, carcinoid, gastric cyst, and HP. The patient resumed oral intake once, but due to recurrence of vomiting symptoms we decided on surgical resection. Prior to the operation, the patient was kept on no food or drink, with a daily volume of 2000 mL of supplemental fluids and an intravenous infusion of proton pump inhibitors.
Images of preoperative examinations. (A, B) Abdominal computed tomography depicted a 40-mm low-density mass that extended beyond the pyloric ring (white arrow) and descended into the duodenal bulb, showing a target sign (yellow arrowhead). (C) Ultrasonography depicted a 40-mm mass with fluid accumulation arising from the gastric submucosa (magenta arrowheads). (D) Gastric fiber revealed a submucosal lesion on the posterior wall of the gastric pylorus.
Laparoscopic distal gastrectomy with Roux-en-Y reconstruction was performed. Since our institution routinely employs the Roux-en-Y reconstruction for distal gastrectomy to prevent residual gastritis, we consistently opted this reconstruction method in this case. Intraoperative findings indicated that the lesion was localized to the gastric pylorus and the stomach was dilated, although the gastroduodenal invagination had already been released (Fig. 2A). The oral side was dissected at the gastric angle, and the anal side margin was dissected at the duodenum using a linear stapler after sufficient margins of the tumor were confirmed grossly from outside the gastric wall (Fig. 2B). The operation time was 248 min and blood loss was 20 mL.
Intraoperative images of laparoscopic surgery. (A) Intraoperative findings indicated that the lesion was localized to the gastric pylorus. (B) The duodenum on the anorectal side of the lesion was divided using a linear stapler.
Surgical specimens showed a submucosal cystic tumor at the gastric pylorus, which was filled with an internal abscess (Fig. 3A, 3B). Histopathological examination revealed pancreatic tissue containing acinar cells and pancreatic ducts from the submucosa to the muscularis propria of the stomach without islets of Langerhans, leading to a diagnosis of Heinrich type II GHP^14)^ (Fig. 3C). Additionally, abscesses containing neutrophils and foamy histiocytes were continuously formed from the pancreatic duct tissue within the heterotopic pancreas (Fig. 3D). The patient resumed oral intake and was discharged on postoperative days 2 and 11, respectively, and is progressing well 7 months after surgery.
Macro and microscopic findings of the resected specimen. (A, B) Surgical specimens indicated a submucosal cystic tumor filled with an abscess (yellow arrowheads) in the gastric pylorus. (C) Histopathological examination revealed pancreatic tissue with acinar cells (yellow arrowhead) and pancreatic ducts (white arrow). (D) In the heterotopic pancreas, an abscess containing neutrophils and foamy histiocytes (boxed area) was continuously formed from the pancreatic duct tissue. The boxed area is magnified in the inset.
DISCUSSION
HP is defined as pancreatic tissue without substantial anatomical or vascular connection to the pancreas, and was first described by Jean-Schultz in 1729.^15)^ In autopsy studies the incidence of HP generally ranged from 0.5% to 13.0%, and was more common in males aged 30−50 years.^16)^ The most common sites of HP are the duodenum (93.6%), stomach (24%–38%), jejunum (0.5%–27.0%), and Meckel’s diverticulum (2.0%–6.5%).^1)^ The majority of GHP originate from the submucosa and occasionally from the muscularis layer. GHP is usually asymptomatic, but depending on its location and size it can cause abdominal symptoms such as vomiting and pain. HP-related symptoms can be divided into two main categories, those due to the size of the mass and those due to pancreatitis.^17)^
Table 1 summarizes the details of GHP with gastric outlet syndrome.^1–10)^ We searched PubMed using the keywords “gastric ectopic pancreas” or “gastric outlet syndrome” (1946–2024) and included studies with detailed patient information. The median age of 7 male and 5 female patients was 44 years (range 26–53 years). The most common symptoms were abdominal pain and vomiting. In all 12 cases the lesions were localized to the pylorus, with a median size of 40 mm (range 20–60 mm). Most GHPs are reportedly located within 50 mm of the pylorus.^18)^ Armstrong et al.^19)^ reported a significant correlation between abdominal symptoms and large lesions (>15 mm in diameter). Larger lesions may cause pyloric stenosis due to gastric outlet obstruction, and rarely they coexist with gastroduodenal invagination, such as in the present case. In cases where the lesion is distant from the pyloric ring, laparoscopic surgery, including laparoscopic endoscopic cooperative surgery, has been reported to be a favorable procedure.^20)^ However, in cases of GHP with gastric outlet syndrome the lesion is often located close to the pyloric ring.^1–7)^ Therefore, we opted for antrectomy in the current case in order to avoid postoperative outlet obstruction due to gastric deformity after local resection of the stomach, and to ensure a sufficient surgical margin. Laparotomy was often chosen in previous cases,^1–3,5–9)^ but laparoscopic surgery could also be performed if the stomach was decompressed and a safe surgical field was secured. GHP is one of the differential diagnoses of submucosal cystic tumors of gastric origin, although it is rarely confirmed preoperatively.^21)^ Endoscopic ultrasound-guided fine needle aspiration was not performed in this case because we believed that fluid was the main component inside the cyst and that a definitive diagnosis was unlikely to be obtained. Abdominal ultrasonography also revealed that the tumor originated from the submucosal layer, thereby excluding epithelial tumors such as gastric adenocarcinoma and neuroendocrine tumor. Based on these findings, we concluded that epithelial malignancy was improbable and attempted a gastrectomy without lymph node dissection.
Rarely, HP can form gastric wall abscesses.^11–13)^ There are two factors that cause HP to form abscesses: (1) the pancreatic duct may be blocked by a protein plug resulting in inflammatory changes, or (2) the pancreatic enzymes themselves are activated resulting in acute pancreatitis. In the present case, pathologically there was no protein plug in the pancreatic duct, suggesting that acute pancreatitis due to HP triggered the formation of gastric wall abscesses. Intriguingly, chronic alcohol consumption has been reported to induce pancreatitis in GHP,^10)^ and it may have caused the development of pancreatitis in the present case. Here, we finally performed a gastrectomy on a GHP with an abscess. Even if a diagnosis of GHP with abscess had been made preoperatively, a gastrectomy would have still been indicated. Regarding the treatment of GHP with abscess, antimicrobial therapy alone has been reported to lead to inflammation recurrence; therefore, surgical treatment is recommended.^22,23)^ As an alternative treatment, several cases where endoscopic ultrasound-guided drainage was performed have been reported, although the abscess recurred, ultimately requiring a gastrectomy.^12,24,25)^ In summary, whether the cause of the abdominal symptoms was gastroduodenal invasion or gastric wall abscess, our decision to perform a laparoscopic distal gastrectomy was reasonable, and it was supported by previous reports of favorable outcomes with surgical procedures.
CONCLUSIONS
We report the first case of laparoscopic distal gastrectomy for GHP with gastroduodenal invasion and gastric wall abscess. The case suggests that surgical resection may be an effective treatment option for GHP with concurrent gastroduodenal invasion and gastric wall abscess.
ACKNOWLEDGMENTS
The authors thank Editage (www.editage.com) for the English language editing. No financial support was received for this study.
DECLARATIONS
Funding
Not applicable.
Authors’ contributions
JF drafted the manuscript. RO, YH, TS, KN, NS, and SH critically revised the manuscript.
All authors read and approved the final manuscript.
Availability of data and materials
The datasets supporting the conclusions of this article are included within the article and its additional files.
Ethics approval and consent to participate
This work does not require ethical considerations or approval. Informed consent to participate in this study was obtained from the patient.
Consent for publication
The patient provided written informed consent to publish this case report.
Competing interests
The authors declare that they have no competing interests.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Christodoulidis G Zacharoulis D Barbanis S Heterotopic pancreas in the stomach: a case report and literature review. World J Gastroenterol 2007; 13: 6098–100.18023108 10.3748/wjg.v 13.45.6098 PMC 4250899 · doi ↗ · pubmed ↗
- 2Huang YC Chen HM Jan YY Ectopic pancreas with gastric outlet obstruction: report of two cases and literature review. Chang Gung Med J 2002; 25: 485–90.12350037 · pubmed ↗
- 3Ikematsu Y Nishiwaki Y Kida H Gastric outlet obstruction caused by a heterotopic pancreas in a pregnant woman: report of a case. Surg Today 2003; 33: 952–5.14669092 10.1007/s 00595-003-2614-3 · doi ↗ · pubmed ↗
- 4Ayantunde AA Pinder E Heath DI. Symptomatic pyloric pancreatic heterotopia: report of three cases and review of the literature. Med Sci Monit 2006; 12: CS 49–52.16733487 · pubmed ↗
- 5Jiang LX Xu J Wang XW Gastric outlet obstruction caused by heterotopic pancreas: A case report and a quick review. World J Gastroenterol 2008; 14: 6757–9.19034986 10.3748/wjg.14.6757 PMC 2773325 · doi ↗ · pubmed ↗
- 6Trifan A Târcoveanu E Danciu M Gastric heterotopic pancreas: an unusual case and review of the literature. J Gastrointestin Liver Dis 2012; 21: 209–12.22720312 · pubmed ↗
- 7Iwahashi S Nishi M Yoshimoto T A case of gastric heterotopic pancreas with gastroduodenal invagination. Surg Case Rep 2019; 5: 110.31292813 10.1186/s 40792-019-0669-7PMC 6620227 · doi ↗ · pubmed ↗
- 8Xiong Y Xie Y Jin D-D Heterotopic pancreas adenocarcinoma in the stomach: A case report and literature review. World J Clin Cases 2020; 8: 1979–87.32518790 10.12998/wjcc.v 8.i 10.1979 PMC 7262711 · doi ↗ · pubmed ↗