Left S3 + S8 Segmentectomy with Rare Interlobar A3 Vascular Anomaly: A Case Report
Hiroki Imabayashi, Takahide Toyoda, Kazuhisa Tanaka, Yuki Sata, Terunaga Inage, Hajime Tamura, Masako Chiyo, Yukiko Matsui, Hidemi Suzuki

TL;DR
This case report describes a rare vascular anomaly during lung cancer surgery and the successful surgical approach used to manage it.
Contribution
The paper presents a rare case of a complete interlobar branch of the left A3 artery during segmentectomy for lung cancer.
Findings
The left A3 artery branched from the interlobar pulmonary artery in a rare anatomical variation.
The surgical approach included securing the apico-posterior and lingular segments to prevent torsion.
Both nodules were confirmed as early-stage squamous cell carcinomas with no recurrence after one year.
Abstract
Segmentectomy is being accepted as a valid operative procedure for small peripheral non-small cell lung cancer. Understanding pulmonary artery (PA) variations is essential to ensure safe and reliable surgeries. Herein, we report a case of left S3 and S8 segmentectomy involving a complete interlobar branch of the left A3, a relatively rare anomaly reported in less than 0.56% of cases in previous studies. A woman in her sixties was referred to our hospital with two nodules in the left upper lobe anterior segment (S3, 1.1 × 0.8 cm) and the lower lobe anterior basal segment (S8, 1.8 × 1.7 cm), suggestive of double primary lung cancer. Preoperative thin-slice computed tomography (CT) and three-dimensional CT revealed a vascular anomaly in which the entire left A3 branched from the interlobar PA. Left S3 and S8 segmentectomies were performed via thoracotomy. The interlobar A3 branched at…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
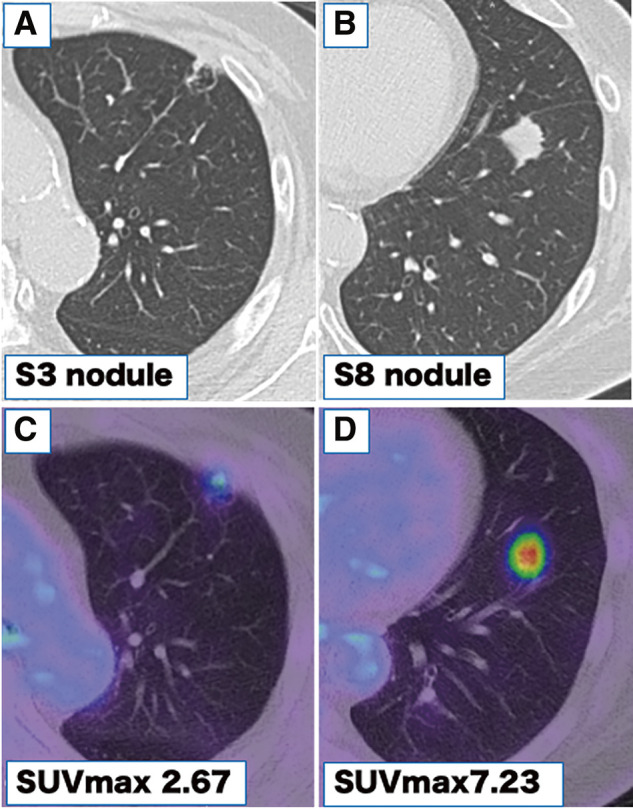 Fig. 1
Fig. 1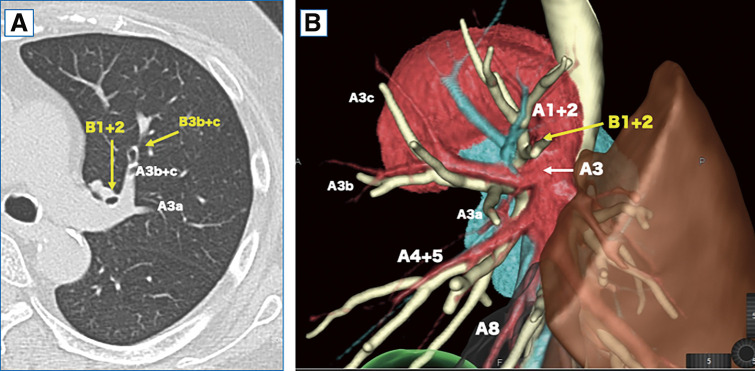 Fig. 2
Fig. 2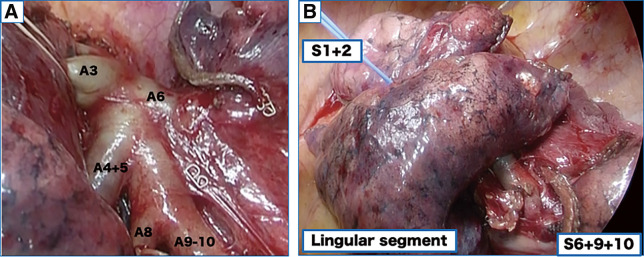 Fig. 3
Fig. 3| First author | Publication | Study | Number of | ILA3a (%) | ILA3 (%) |
|---|---|---|---|---|---|
| Yamashita H. | 1978 | Cadaver | 165 | 16 (9.7) | 0 (0.0) |
| Murota M. | 2020 | 3D-CT | 320 | 27 (8.4) | 0 (0.0) |
| Maki R. | 2022 | 3D-CT | 539 | 54 (10.0) | 3 (0.56) |
| Xu H. | 2023 | 3D-CT | 100 | 2 (2.0) | 0 (0.0) |
| Total | 1124 | 99 (8.8) | 3 (0.27) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsVascular anomalies and interventions · Renal and Vascular Pathologies · Vascular Anomalies and Treatments
Abbreviations
3D-CT three-dimensional computed tomography CT computed tomography NSCLC non-small cell lung cancer PA pulmonary artery
INTRODUCTION
Recent randomized non-inferiority trials comparing segmentectomy with lobectomy for small peripheral non-small cell lung cancer (NSCLC) have demonstrated the non-inferiority of segmentectomy.^1)^ As segmentectomy becomes increasingly established as a valid oncological option for the treatment of small peripheral NSCLC, thoracic surgeons must be well-versed in patient selection, segmentation techniques, and lymph node assessment for segmentectomy in early-stage NSCLC.^2)^ Compared with lobectomy, segmentectomy requires more precise handling of the pulmonary arteries (PAs) and veins, necessitating a thorough understanding of their anatomy.^3)^ Herein, we report a case of left S3+S8 segmentectomy for double lung cancer involving a complete interlobar branch of the left A3, a relatively rare anomaly reported in less than 0.56% of cases in previous studies.^4,5)^ To our knowledge, this is the first case report of left S3 segmentectomy with complete interlobar A3. This vascular anomaly in S3 segmentectomy raises a unique concern regarding the possibility of postoperative lung torsion. Our case report adheres to the case report (CARE) checklist.^6)^
CASE PRESENTATION
A woman in her sixties was referred to our hospital with two nodules in the left upper lobe anterior segment (S3, 1.1 × 0.8 cm) and the lower lobe anterior basal segment (S8, 1.8 × 1.7 cm), detected by chest radiography and computed tomography (CT) during a medical check-up (Fig. 1A and 1B). 18F-fluorodeoxyglucose positron emission tomography showed abnormal uptake in the S3 and S8 tumors, with maximum standardized uptake values of 2.67 and 7.23, respectively, leading to a surgical plan under suspicion of double primary lung cancer (Fig. 1C and 1D). Thin-slice CT revealed a vascular anomaly, with the left A3 branching from the interlobar fissure (Fig. 2A). Preoperative three-dimensional (3D) CT was performed using Ziostation 2 and REVORAS (Ziosoft Inc., Tokyo, Japan) (Fig. 2B). The A3a branched proximally from A3, while the A3b and A3c branched distally. The A4/5 was of the interlobar type and branched independently of A3. No other apparent anomalies were observed in the pulmonary arteries (PAs) or the bronchi of the lower lobe. Since lung cancer was strongly suspected based on CT findings, surgical resection was performed without intraoperative pathological confirmation. A short edited intraoperative video is available in Supplementary Video 1. The surgery was conducted through a 10-cm axillary fifth intercostal thoracotomy, with a 2-cm incision in the seventh intercostal space for the camera port. Due to a partially incomplete fissure, the PA was exposed from the dorsal side, revealing the interlobar A3 branching the same level as A6 (Fig. 3A). V3b and V3c were separated from the anterior side, while A3 was separated from the interlobar side. The intersegmental plane and A3 were sequentially divided using staplers. With A3 bifurcation on the interlobar side and the V3 bifurcation anteriorly, the apico-posterior (S1+2) and the lingular segments were completely separated as blocks after S3 segmentectomy (Fig. 3B). An S8 segmentectomy was performed simultaneously. ND1a lymph node dissection and #10 lymph node sampling were carried out. To prevent torsion, the staple line ends of the intersegmental plane of S1+2 and the lingular segments were loosely linked using silk sutures (Supplementary Fig. 1 and Video 1). The operation time was 4 h and 8 min, with 20 g blood loss. Pathological examination revealed squamous cell carcinoma in both the left S3 and S8 nodules, which were diagnosed as pT1bN0M0, pStage IA2. A prolonged air leak occurred, and pleurodesis with OK-432 was performed on postoperative day 5. The chest tube was removed on postoperative day 9. The patient remained recurrence-free for over 1 year.
Chest computed tomography of the nodules. (A, B) Nodules measured 1.1 × 0.8 cm and 1.8 × 1.7 cm in the left S3 (A) and S8 segments (B), respectively. (C, D) 18F-fluorodeoxyglucose positron emission tomography demonstrated abnormal uptake in the tumors, with maximum standardized uptake values of 2.67 (C) and 7.23 (D), respectively.
Thin-slice computed tomography (CT) and Three-dimensional CT findings. (A) Thin-slice computed tomography (CT) findings: The left A3 exhibited vascular branching, with all branches originating from the interlobar pulmonary artery. (B) Three-dimensional CT findings: The left A3a branched from the A3 stem, while A3b and A3c branched at the periphery. The lingular artery branched independently from the interlobar pulmonary artery.
Intraoperative findings. (A) The interlobar A3 branched at the same level as A6 from the main pulmonary artery. (B) After S3 and S8 segmentectomy, the S1+2, lingular segment, and S6+9+10 were separated into isolated blocks, raising concerns about potential torsion.
DISCUSSION
Anatomical variations are more common in the left PA than in the right PA.^7–9)^ Ma et al. reported that 97.6% of left upper lobe branches typically consist of 3–5 branches, with a minimum of two and a maximum of seven branches observed, indicating highly diverse vascular patterns.^10)^ Yamashita investigated whether the lingular artery branches from the first branch centered on the mediastinal A3 or from the second branch centered on the interlobar A1+2. They found that 72.7% (120/165) were interlobar-type lingular arteries.^11)^ Murota et al. further refined this classification of branching patterns in the interlobar region, focusing on the relationships between A1+2c, the lingular artery, and A6, into seven major categories and 85 subcategories.^4)^ In this classification, interlobar branching of A3a was observed in 8.4% (27/320) of cases, but no cases were found where the first mediastinal branch was absent and all A3 branches, including A3b and A3c, branched from the interlobar fissure.^4)^ Similar results have been reported in other studies.^4,11,12)^ Conversely, cases such as ours, where all A3a, b, and c branches from the interlobar fissure were reported, were identified by Maki et al., with 3 out of 539 cases (0.56%) presenting with interlobar-type lingular arteries.^5)^ A summary of the previously reported cases of interlobar A3 branching is presented in Table 1. Three-dimensional CT (3D-CT) interpretation, as demonstrated in this case, is considered a useful tool for the preoperative detection of pulmonary arteriovenous branching anomalies. Accurate preoperative understanding of the direction and changes in PAs is crucial to reduce the risk of bleeding.^13,14)^ Furthermore, in addition to evaluating PA branching patterns using 3D-CT, thin-slice CT images should be assessed to better evaluate the fine PA branches.^15)^ Even in segmentectomy cases involving rare vascular anomalies, such as the present case, careful preoperative simulation using 3D guides and thin-section CT images allowed us to perform the surgery without unexpected bleeding. After S3 segmentectomy, with the base of A3 on the interlobar side and the base of V3 anteriorly, S1+2 and the lingula were completely separated, necessitating measures to prevent torsion of the remaining lung. By predicting the relationship of the remaining lung after segmentectomy based on vascular positioning, and considering intraoperative precautions such as preserving the mediastinal and interlobar pleura as much as possible, postoperative complications can be reduced.^16)^
CONCLUSIONS
We encountered a case of left S3 segmentectomy involving a highly unusual complete interlobar branch of the left A3 segment. Preoperative identification of PA anomalies through 3D-CT and detailed surgical simulations, including assessment of the remaining lung after resection, is essential for ensuring surgical safety. In cases of left S3 segmentectomy with an interlobar A3, it may be necessary to implement measures to prevent torsion, as the S1+2 and lingular segments are prone to becoming isolated blocks.
ACKNOWLEDGMENTS
The authors thank Editage for their assistance in proofreading the English text.
DECLARATIONS
Funding
None.
Authors’ contributions
TT, HI, and KT performed the surgery, and HI, TT, KT, YS, TI, HT, MC, YM, and HS followed up the patient.
The manuscript was prepared by HI and TT, under the supervision of HS.
The authors read and approved the final manuscript.
Availability of data and materials
Data sharing is not applicable to this article, since datasets were neither generated nor analyzed for the case report.
Ethics approval and consent to participate
Patient privacy was considered and the manuscript did not include any identifying information.
Consent for publication
The patient provided informed consent for the publication of this case report.
Competing interests
All authors completed the ICMJE uniform disclosure form. The authors declare that they have no conflicts of interest.
SUPPLEMENTARY MATERIALS
Supplementary Figure 1. Intraoperative findings. To prevent torsion, the staple line ends of the intersegmental plane of S1+2 and the lingular segments were loosely linked using silk sutures (yellow allow).
Supplementary Video
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Saji H Okada M Tsuboi M Segmentectomy versus lobectomy in small-sized peripheral non-small-cell lung cancer (JCOG 0802/WJOG 4607 L): a multicentre, open-label, phase 3, randomised, controlled, non-inferiority trial. Lancet 2022; 399: 1607–17.35461558 10.1016/S 0140-6736(21)02333-3 · doi ↗ · pubmed ↗
- 2Liu L Aokage K Chen C Asia expert consensus on segmentectomy in non-small cell lung cancer: A modified Delphi study. JTCVS Open 2023; 14: 483–501.37425437 10.1016/j.xjon.2023.03.013PMC 10328970 · doi ↗ · pubmed ↗
- 3Liu X Zhao Y Xuan Y Three-dimensional printing in the preoperative planning of thoracoscopic pulmonary segmentectomy. Transl Lung Cancer Res 2019; 8: 929–37.32010571 10.21037/tlcr.2019.11.27PMC 6976356 · doi ↗ · pubmed ↗
- 4Murota M Yamamoto Y Satoh K An analysis of anatomical variations of the left pulmonary artery of the interlobar portion for lung resection by three-dimensional CT pulmonary angiography and thin-section images. Jpn J Radiol 2020; 38: 1158–68.32729007 10.1007/s 11604-020-01024-1 · doi ↗ · pubmed ↗
- 5Maki R Miyajima M Ogura K Pulmonary vessels and bronchus anatomy of the left upper lobe. Surg Today 2022; 52: 550–8.35179645 10.1007/s 00595-022-02471-1 · doi ↗ · pubmed ↗
- 6Riley DS Barber MS Kienle GS CARE guidelines for case reports: explanation and elaboration document. J Clin Epidemiol 2017; 89: 218–35.28529185 10.1016/j.jclinepi.2017.04.026 · doi ↗ · pubmed ↗
- 7Tsubota N. Vascular and bronchial abnormalities. Illustrated Lung Cancer Surgery: Basic and Advanced Techniques. 2nd ed. Tokyo: Igaku Shoin. 2007. p. 39.
- 8Veeramachaneni NK. Surgical anatomy of the lungs. In: Lo Cicero J Feins RH Colson YL Rocco G, editors. Shields’ general thoracic surgery. 8th ed. Philadelphia: Lippincott Williams & Wilkins. 2018. p.101–111.