A Case of Secondary Extramammary Paget's Disease Surrounding a Cutaneous Ureterostoma After Recurrence of Bladder Urothelial Carcinoma
Masahiro Mizoguchi, Ichiro Chihara, Keisuke Sano, Tomokazu Kimura, Shuya Kandori, Hiromitsu Negoro, Bryan J. Mathis, Hitomi Kawai, Daisuke Matsubara, Hiroyuki Nishiyama

TL;DR
A man developed a rare skin condition called secondary extramammary Paget's disease near a surgical opening after his bladder cancer recurred.
Contribution
This case report highlights the occurrence of secondary extramammary Paget's disease following recurrence of urothelial carcinoma after urinary diversion.
Findings
A 68-year-old man developed secondary extramammary Paget's disease around a ureterostoma after bladder cancer recurrence.
Pathology confirmed urothelial carcinoma and pagetoid cells in the epidermis, indicating secondary Paget's disease.
The case suggests a link between recurrent upper urothelial carcinoma and secondary extramammary Paget's disease.
Abstract
Secondary extramammary Paget's disease features intraepidermal carcinoma caused by tumor invasion and migration into adjacent skin. A 68‐year‐old man underwent radical cystectomy and bilateral cutaneous ureterostomy for bladder cancer and right ureteral cancer. Postoperative follow‐up computed tomography and urine cytology at 3 years suggested right ureteral cancer recurrence. Contemporaneous erythema and bulging of the skin around the right ureterocutaneous fistula were observed, necessitating retroperitoneoscopic nephroureterectomy and peristomal skin resection. Pathology revealed urothelial carcinoma with T2 disease at the lower ureter, plus spreading cytokeratin 7+ and cytokeratin 20+ pagetoid cells clustered within the epidermis indicative of secondary Paget's disease. In cases of recurrent upper urothelial carcinoma after urinary diversion, patients may develop secondary…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
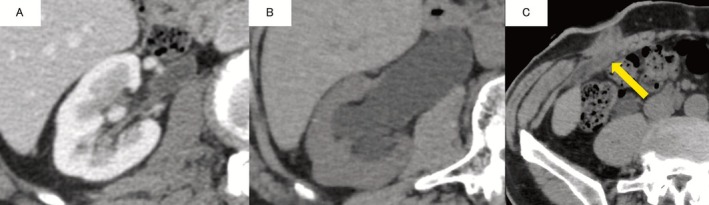 FIGURE 1
FIGURE 1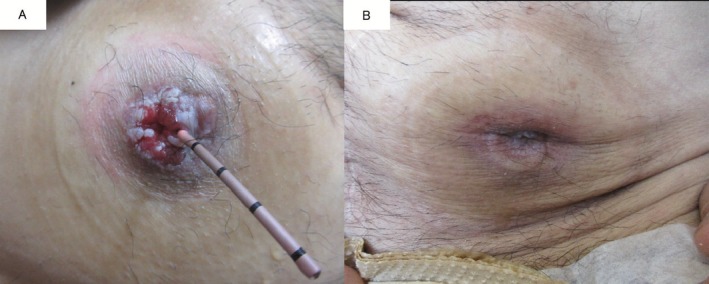 FIGURE 2
FIGURE 2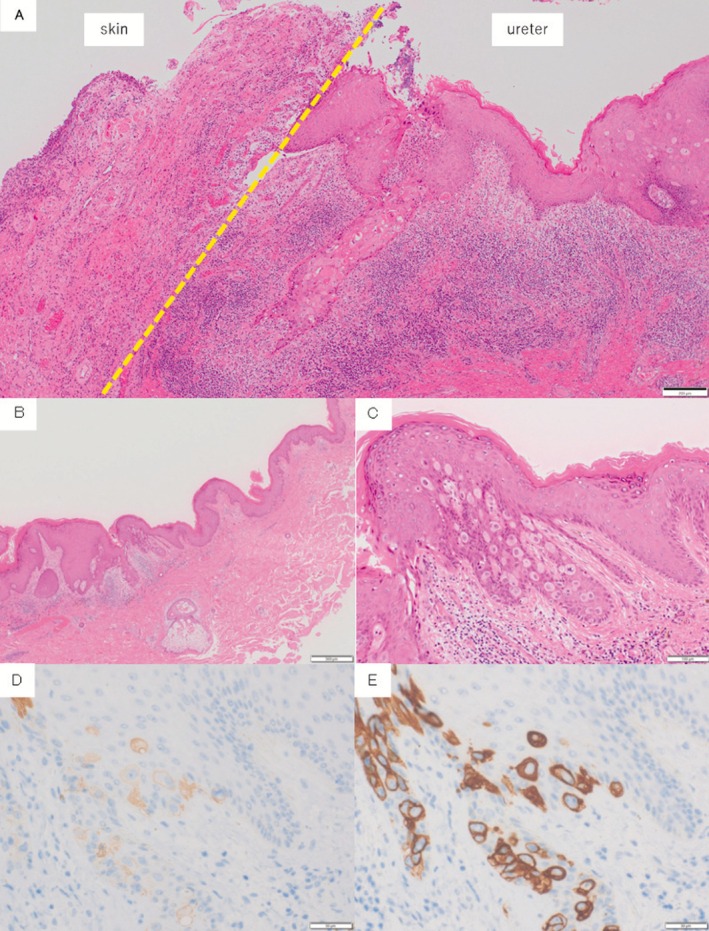 FIGURE 3
FIGURE 3| Report | Age, Sex | Primary tumor | Urinary diversion | Recurrence period | Presence of metastases at diagnosis | Gross findings of the stoma | Treatment of pagetoid spread | Outcome | Biopsy | Stage | Subtype | CK7 | CK20 | GCDFP‐15 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Nakata (2010) | 78, M | Ureteral cancer | Ileal conduit | 13 years | NA | Dermatitis | Skin excision | NA | + | NA | NA | + | + | NA |
| Ito (2013) | 69, F | Left ureteral cancer Tis, bladder cancer Tis | Ureterocutaneostomy | 2 years | None | Tumor formation |
Skin excision +right lower ureterectomy | NA | + | pTis | − | + | + | NA |
| Ishida (2013) | 77, M | Bladder cancer T4 | Ureterocutaneostomy | 4 years 6 months | None | Tumor formation |
Skin excision +right nephroureterectomy | NA | + | pTis | − | + | + | − |
| Sakatani (2013) | 84, M | Prostatic urethra Tis | Ureterocutaneostomy | 4 years 6 months | NA | Dermatitis |
Skin excision +right nephroureterectomy | Survived for 1 year | + | pT1 | − | + | + | − |
| Kanda (2016) | 85, M | Right ureteral cancer T2, bladder cancer T2 | Ureterocutaneostomy | 4 years 6 months | None | Erosion |
Skin excision +left lower ureterectomy | Died after 7 months | + | pT1 | − | + | + | NA |
| Present case | 68, M | Right ureteral cancer T2, bladder cancer T3a + is | Ureterocutaneostomy | 3 years | None | Dermatitis |
Skin excision +right nephroureterectomy | Survived for 1 year and 6 months (cancer death) | − | pT2 | − | + | + | NA |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCancer and Skin Lesions · Nonmelanoma Skin Cancer Studies · Urinary and Genital Oncology Studies
Summary
- Secondary extramammary Paget's disease (SEMPD) around a cutaneous ureterostoma is rare.
- Regular monitoring of skin lesions around the stoma offers an early, noninvasive detection method.
- SEMPD should be considered in the differential diagnosis if tumor formation or refractory dermatitis is present.
AbbreviationsCK20cytokeratin 20CK7cytokeratin 7CTcomputed tomographyEMPDextramammary Paget's diseaseGCDFP15Gross Cystic Disease Fluid Protein‐15HEhematoxylin–eosinPDPaget's diseaseSEMPDsecondary extramammary Paget's diseaseUCurothelial carcinoma
Introduction
1
Secondary extramammary Paget's disease (SEMPD) stems from skin‐adjacent organ cancer that migrates through the epithelium to the epidermis, presenting as intraepidermal carcinoma [1]. SEMPD skin manifestations are characterized by velvety, erythematous eczema (often mistaken for eczema or contact dermatitis) [2], usually warranting surgical resection, although standards of care remain unestablished due to disease rarity [1, 3].
Cases of urothelial carcinoma (UC)‐mediated SEMPD at the stoma site are very rare. Here, we report such a case in the right stoma site at the right ureter recurrence after radical cystectomy via bilateral cutaneous ureterostomy.
Case Presentation
2
A 68‐year‐old man with chronic kidney disease (estimated glomerular filtration rate 57.3 mL/min/1.73 m^2^) was diagnosed with bladder cancer (cT2N0M0) and right lower ureteral cancer (cT2N0M0) based on transurethral resection of the bladder tumor and CT. Ureteroscopy showed no tumors beyond the right lower ureter. As lower ureterectomy for lower ureteral cancer is reportedly similar in results to radical nephroureterectomy [4], he hoped to reduce dialysis risk by undergoing cystectomy, right lower ureterectomy, and bilateral ureterostomies. The intraoperative frozen section of the ureter was margin‐negative. The bladder and ureter tumors were histologically diagnosed as UC, pT3a + is N0 and UC, pT1 (3 cm from the right ureteral transection, RM0), respectively. Postoperative adjuvant chemotherapy was skipped since neoadjuvant chemotherapy (cisplatin and gemcitabine) was previously administered and other treatments were unavailable in Japan at that time.
Postoperative 3‐year follow‐up CT showed right hydronephrosis and wall thickening of the right lower ureter with subcutaneous periureteral involvement (Figure 1). Simultaneous mild erythema and bulging around the right stoma were noted (Figure 2) and renal pelvic lavage cytology was class III. Right ureteral carcinoma recurrence was diagnosed based on these findings and a retroperitoneoscopic right nephroureterectomy with peristomal skin resection was performed. The ureteral tumor was located just below the right cutaneous ureterostomy, but without skin continuity, and pathology indicated UC, pT2 (Figure 3A). Although urothelial carcinoma was absent in the concurrently resected skin, hematoxylin–eosin (HE) staining (Figure 3B,C) revealed CK7+ (Figure 3D) and CK20+ (Figure 3E) tumor cells showing pagetoid spreading within the epidermal skin lesions. Finally, a diagnosis of SEMPD was made based on continuous invasion of the ureteral tumor through to the skin along with the pagetoid spreading.
Postoperative CT findings. The patient had mild hydronephrosis after surgery (A) but this had progressed 3 years later (B). In addition, subcutaneous wall thickening and periureteral involvement were observed near the opening of the right ureter (C).
Cutaneous ureterostomy findings, revealing mild erythema and bulging around the right side (A). There were no remarkable findings on the left side (B).
(A) The pathology of the transition area between the skin (left) and ureter (right). On the skin side, Paget cells were observed, while on the ureteral side, findings of urothelial carcinoma were present. However, no continuity is visible between these two areas. (B–E) Skin lesion pathological findings. (B) Hematoxylin–eosin findings (HE staining, magnification: 4×). (C) Large atypical cells with pale spores in the epidermis, putatively identified as Paget cells (HE staining, magnification: 20×). Paget cells in the stoma site were verified positive for both CK7 (D) and CK20 (E).
He was discharged without complications and remains recurrence‐free 3 years after right nephroureterectomy.
Discussion
3
Paget's disease (PD) is characterized by proliferation and development of atypical large cells (Paget cells) in the epidermis and classified into breast or extramammary Paget's disease (EMPD) based on the origin site [5]. EMPD usually erupts at apocrine gland‐enriched sites [3, 6, 7, 8, 9, 10], such as the vulva, axilla, and perianal area [11]. Conversely, as SEMPD manifests from skin‐adjacent organ malignancies that tunnel through the epithelium to the epidermis, it differs from EMPD in primary lesion classification (i.e., cutaneous vs. other malignancies). Although UC may cause Paget's phenomenon at the external urethral meatus [1, 8], similarly to uterine carcinoma at the vaginal vestibule [12] or recto‐anal carcinoma at the anus [13], it only occurs in 2% of vulvar cancers and less than 1% of anal cancers [1, 13]. The frequency remains unrevealed in UC patients.
Since Paget cells may resemble pagetoid spreading tumor cells, HE staining alone is inadequate for accurate diagnosis. Typically, primary PD is CK7+ and CK20−, while SEMPD of UC origin is CK7+ and CK20+ [9]. Nevertheless, since immunostaining results may differ by cancer type, Gross Cystic Disease Fluid Protein‐15 (GCDFP15; an apocrine epithelium‐specific tissue protein) is a preferred marker for SEMPD [13] and can readily differentiate primary and secondary cancers in initially detected skin lesions [14].
Table 1 summarizes the existing SEMPD case literature involving patients with UC [15], all diagnosed as SEMPD by immunostaining for CK7/20 or GCDFP15. One case had an ileal conduit and five had cutaneous ureterostomies. Recurrence ranged from 2 to 13 years (median 4.5 years), with skin biopsies performed in all cases except ours, followed by surgery. Of note, there were obvious skin findings (i.e., tumor formation and refractory dermatitis) in all cases (including ours) (Table 1). Both early and noninvasive, regular skin observation around the stoma after urinary tract changes is an excellent prophylactic measure. However, SEMPD is rare enough to render a definitive diagnosis difficult based on skin findings alone because of differential diagnoses. Here, biopsy was eschewed because of the lower tumor localization requiring a total resection of the right renal ureter along with the concomitant resection of the skin lesion. However, all cases, except ours, were biopsied for diagnosis due to skin‐isolated findings. Thus, indeterminate skin findings should precipitate immediate biopsy instead of waiting for follow‐up.
While clinical guidelines to treat SEMPD remain unpublished, several reports recommend surgical resection [3, 6] of the skin lesion plus treatment of the primary lesion. Since lesions rarely extend into the dermis, segmental resection of the fatty layer should maintain 1–2 cm margins [3, 7, 18, 19]. If a 2 cm resection margin appears impossible, skin biopsy should be considered to confirm resection margins [19, 20]. Alternatively, chemotherapy targeting the primary tumor has been reported as effective for SEMPD lesions since platinum‐based chemotherapy achieved temporary lesion control in a UC case [1].
In conclusion, since SEMPD in UC patients is rare, clinicians may never encounter it after urinary tract diversion. But, until chemotherapy efficacy for SEMPD is verified, timely detection and complete resection are considered the most effective treatment. Regular observation of any skin lesions around the stoma are an excellent method of detecting SEMPD, with surgery considered if confirmed, while biopsies should be immediately conducted if skin findings are unclear.
Consent
Patient consent for publication was obtained.
Conflicts of Interest
The authors declare no conflicts of interest. Hiromitsu Negoro and Hiroyuki Nishiyama, Editorial Board members of International Journal of Urology Case Reports and co‐authors of this article, were excluded from editorial decisions on its acceptance to avoid bias.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1S. Yamamoto , T. Shimomura , K. Kasai , et al., “Pagetoid Spread of Urothelial Carcinoma Controlled Without Resection,” IJU Case Reports 6 (2013): 65–69.10.1002/iju 5.12555 PMC 980735036605693 · doi ↗ · pubmed ↗
- 2S. Kajtezovic , A. R. Walker , B. Hjalmarsson , S. G. Bell , E. Everett , and C. Wong , “Management of Secondary Paget's Disease of the Vulva Associated With Transitional Cell Carcinoma,” Journal of Cancer Research and Clinical Oncology 148 (2022): 1697–1702.35430687 10.1007/s 00432-022-04007-z PMC 11800952 · doi ↗ · pubmed ↗
- 3S. Ishizuki and Y. Nakamura , “Extramammary Paget's Disease: Dagnosis, Pathogenesis, and Treatment With Focus on Recent Developments,” Current Oncology 28 (2021): 2969–2986.34436026 10.3390/curroncol 28040260 PMC 8395499 · doi ↗ · pubmed ↗
- 4H. Fukushima , K. Saito , J. Ishioka , et al., “Equivalent Survival and Improved Preservation of Renal Function After Distal Ureterectomy Compared With Nephroureterectomy in Patients With Urothelial Carcinoma of the Distal Ureter: A Propensity Score‐Matched Multicenter Study,” International Journal of Urology 21 (2014): 1098–1104.25041040 10.1111/iju.12554 · doi ↗ · pubmed ↗
- 5B. Malcolm , M. D. Dockerty , and M. D. Joseph Hyde Pratt , “Extramammary Paget's Disease A Report of Four Cases in Which Certain Features of Histogenesis Were Exhibited,” Cancer 5 (1952): 1161–1169.12998022 10.1002/1097-0142(195211)5:6<1161::aid-cncr 2820050612>3.0.co;2-d · doi ↗ · pubmed ↗
- 6K. St. Claire , A. Hoover , K. Ashack , and A. Khachemoune , “Extramammary Paget Disease,” Dermatology Online Journal 25 (2019): 1–12.31046904 · pubmed ↗
- 7B. J. Kim , S. K. Park , and H. Chang , “The Effectiveness of Mapping Biopsy in Patients With Extramammary Paget's Disease,” Archives of Plastic Surgery 41 (2014): 753–758.25396191 10.5999/aps.2014.41.6.753PMC 4228221 · doi ↗ · pubmed ↗
- 8W. Q. S. P. Primo , G. R. P. Primo , D. B. Basilio , K. K. Machado , J. P. Carvalho , and F. M. Carvalho , “Vulvar Paget Disease Secondary to High Grade Urothelial Carcinoma With Underlying Massive Vascular Embolization and Cervical Involvement: Case Report of Unusual Presentation,” Diagnostic Pathology 14 (2019): 125.31699107 10.1186/s 13000-019-0895-0PMC 6836446 · doi ↗ · pubmed ↗