Swallowed by the Past: Dysphagia as a Decade-Late Manifestation of Renal Cell Carcinoma Recurrence
Hassam Ali, Fnu Poonam, Prashant Mudireddy

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
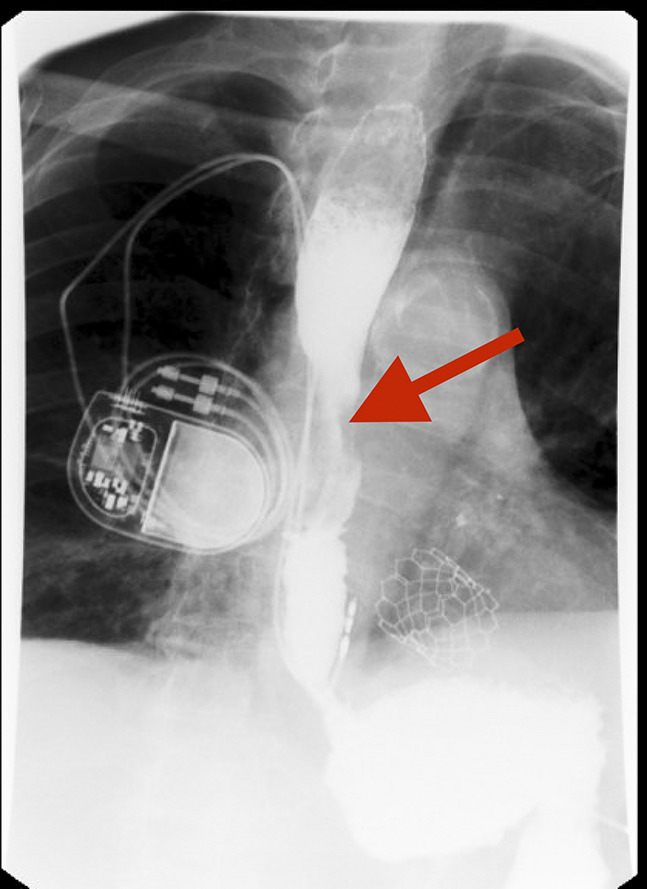 Figure 1
Figure 1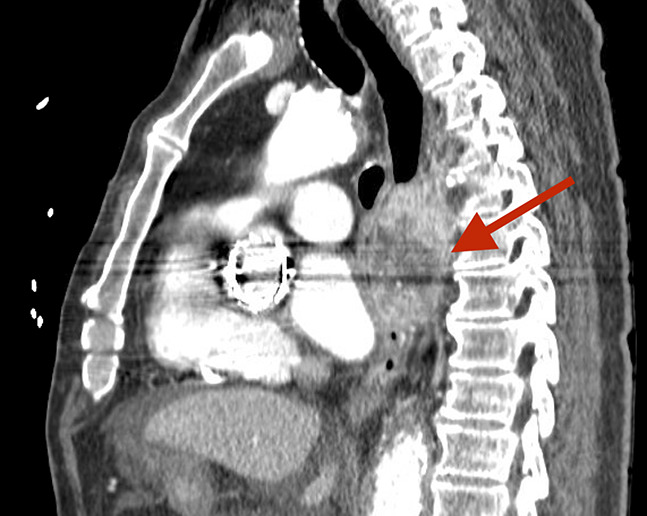 Figure 2
Figure 2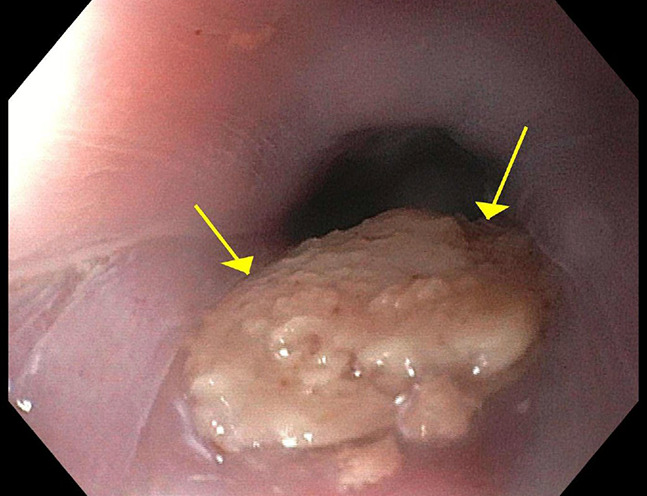 Figure 3
Figure 3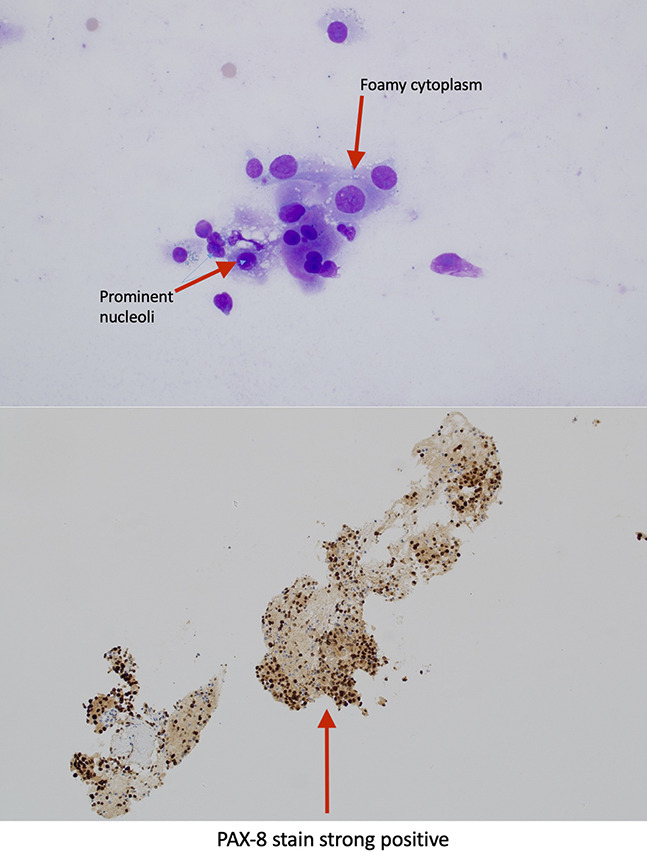 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTuberous Sclerosis Complex Research · Renal cell carcinoma treatment
CASE REPORT
A 74-year-old man with a history of metastatic clear cell renal cell carcinoma (RCC), status postright nephrectomy and radiation therapy to para-aortic lymph nodes 10 years earlier, presented with progressive dysphagia over several months. His medical history included end-stage renal disease on peritoneal dialysis, coronary artery disease, and atrial fibrillation (post-Watchman device). Surveillance imaging had shown no disease recurrence until this presentation. Barium swallow indicated a midesophageal stricture (Figure 1). Chest computed tomography revealed an enlarging subcarinal mass in the posterior mediastinum, measuring 52 × 44 mm, compressing the esophagus (Figure 2). Esophagogastroduodenoscopy identified an ulcerated, malignant-appearing stenosis in the midesophagus (Figure 3). Endoscopic ultrasound-guided biopsy demonstrated an infiltrating mass with strong paired box gene 8 positivity, confirming metastatic RCC (Figure 4). The patient was referred to medical oncology to start systemic chemotherapy. Balloon dilation was performed to alleviate dysphagia with future plans for palliative stenting. This case underscores the potential for delayed gastrointestinal manifestations of RCC recurrence, exemplified by dysphagia due to esophageal compression from mediastinal metastasis, even a decade postnephrectomy. Such late recurrences, including isolated mediastinal lymph node metastases, have been documented in the literature.^1–3^ Clinicians should maintain a high index of suspicion for metastatic disease in patients with RCC presenting with new gastrointestinal symptoms, regardless of the time elapsed since initial treatment. Although isolated mediastinal metastases are uncommon, regular thoracic surveillance may be warranted in long-term follow-up.^4,5^
Esophagram demonstrating significant esophageal narrowing. Figure shows an upper gastrointestinal contrast study revealing a tight narrowing of the midesophagus with extrinsic compression (red arrow), suggestive of a mass effect.
Sagittal view of the chest by contrast-enhanced computed tomography scan. The figure highlights an esophageal mass causing significant luminal obstruction and compression of adjacent structures (red arrow).
Endoscopic visualization of the esophageal lumen. The figure reveals the intraluminal impression of a smooth, bulky mass (yellow arrows), corresponding to the extrinsic compression noted on imaging studies.
Histopathologic confirmation of metastatic RCC. The top panel shows a hematoxylin and eosin stain (×40 magnification) with foamy cytoplasm and prominent nucleoli. The bottom panel demonstrates strong PAX-8 immunohistochemical staining, consistent with metastatic RCC. RCC, renal cell carcinoma.
DISCLOSURES
Author contributions: Writing manuscript and literature research: H. Ali; pathology expert: F. Poonam; supervision; supervision of case and manuscript: P. Mudireddy and article guarantor: H. Ali. Dr. Ali accepts full responsibility for the conduct of the study and the integrity of the work as a whole.
Financial disclosure: None to report.
Informed consent was obtained for this case report.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Lin H Zhang H Cheng Y Zhang C. Solitary metastasis in the mediastinal lymph node after radical nephrectomy for clear cell renal cell carcinoma: A case report and literature review. Front Oncol. 2020;10:593142.33392088 10.3389/fonc.2020.593142 PMC 7773822 · doi ↗ · pubmed ↗
- 2Kanzaki R Higashiyama M Okami J Kodama K. Surgical treatment for patients with solitary metastasis in the mediastinal lymph node from renal cell carcinoma. Interact Cardiovasc Thorac Surg. 2009;8(4):485–7.19126555 10.1510/icvts.2008.191114 · doi ↗ · pubmed ↗
- 3Miyazaki K Sato S Kodama T Kurishima K Satoh H Hizawa N. Mediastinal lymph node metastasis of renal cell carcinoma: A case report. Oncol Lett. 2016;11(2):1600–2.26893788 10.3892/ol.2016.4090 PMC 4734274 · doi ↗ · pubmed ↗
- 4Urushibara M Nagata M Okumura T Bladder metastasis with additional metastases in multiple other organs 4 years after radical nephrectomy for clear cell renal cell carcinoma: A case report and review of the literature. J Med Case Rep. 2022;16(1):131.35366927 10.1186/s 13256-022-03368-w PMC 8977018 · doi ↗ · pubmed ↗
- 5Boorjian SA Crispen PL Lohse CM Leibovich BC Blute ML. Surgical resection of isolated retroperitoneal lymph node recurrence of renal cell carcinoma following nephrectomy. J Urol. 2008;180(1):99–103.18485415 10.1016/j.juro.2008.03.025 · doi ↗ · pubmed ↗