Diffusion Tensor Imaging 3D Tractography-Guided, Individualized, Transsulcul Approach for Subcortical Hematoma Evacuation Using BrainPath/Myriad
Jose M Soto, Dongxia Feng, Yilu Zhang, Anthony Nguyen, Harold Sonnier, Jason H Huang

TL;DR
This paper explores a new minimally invasive surgery method for brain hemorrhage that uses advanced imaging to guide procedures and avoid damaging important brain pathways.
Contribution
The study introduces a DTI-guided, trans-sulcal MIS approach using BrainPath/Myriad for safer subcortical hematoma evacuation.
Findings
DTI-guided MIS with BrainPath/Myriad is feasible and safe for sICH evacuation.
DTT aids in surgical planning and may predict motor recovery after surgery.
Three patients showed successful outcomes with minimal residual hematoma.
Abstract
sICH (spontaneous intracerebral hemorrhage) is a major cause of death and disability. Traditional surgical evacuation, while beneficial, risks damaging healthy tissue. Minimally invasive surgery (MIS) offers a promising alternative. This study explores the feasibility and safety of diffusion tensor imaging (DTI)-guided, trans-sulcal MIS with BrainPath/Myriad NICO Corporation (Indianapolis, IN, USA) for sICH evacuation. DTI/tractography (DTT) visualizes critical pathways like the corticospinal tract (CST), aiding surgical planning and potentially predicting motor function recovery post-surgery. Our objectives include i) assessing the feasibility and safety of DTT-guided, trans-sulcal MIS with BrainPath/Myriad for sICH evacuation. ii) Evaluating DTT's utility in surgical planning and its potential role in predicting motor function recovery. Three sICH patients underwent pre-operative…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
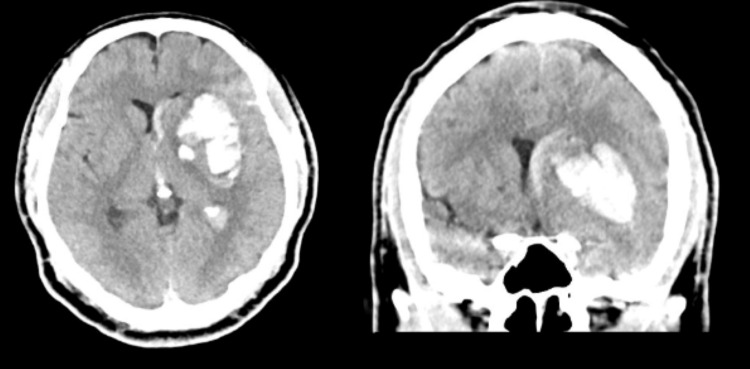 Figure 1
Figure 1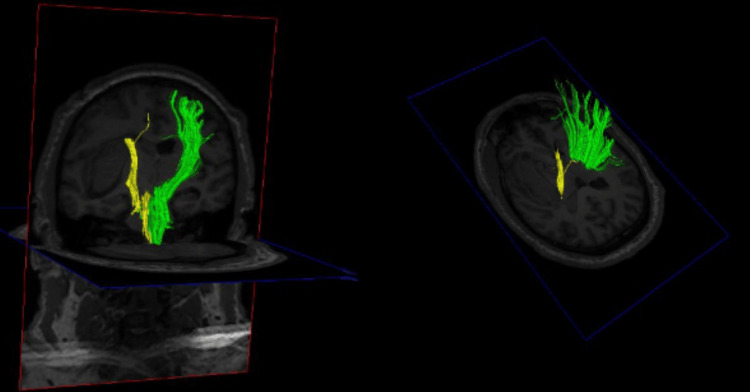 Figure 2
Figure 2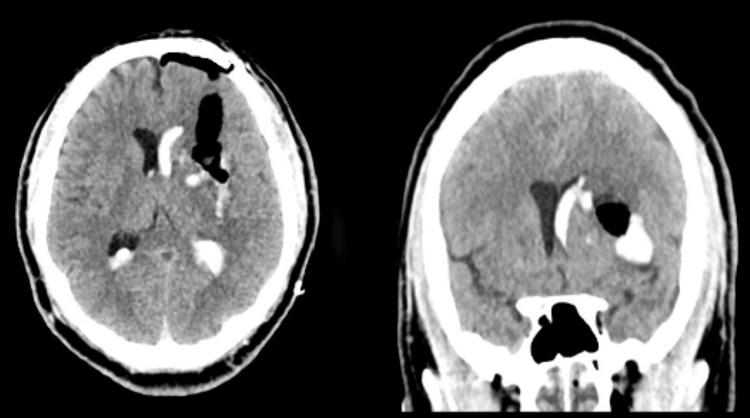 Figure 3
Figure 3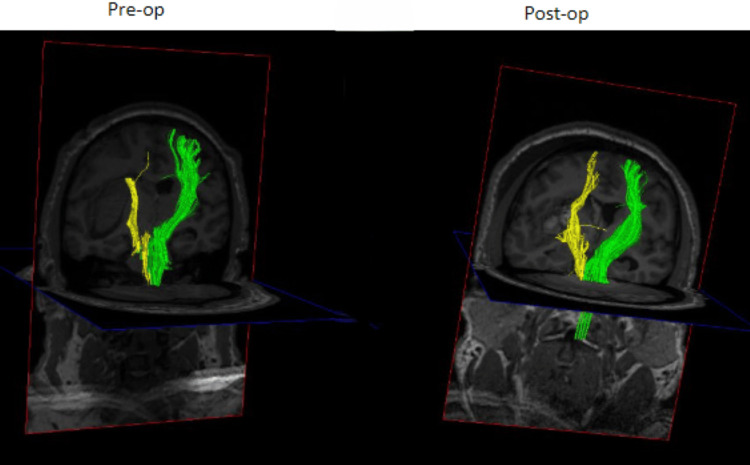 Figure 4
Figure 4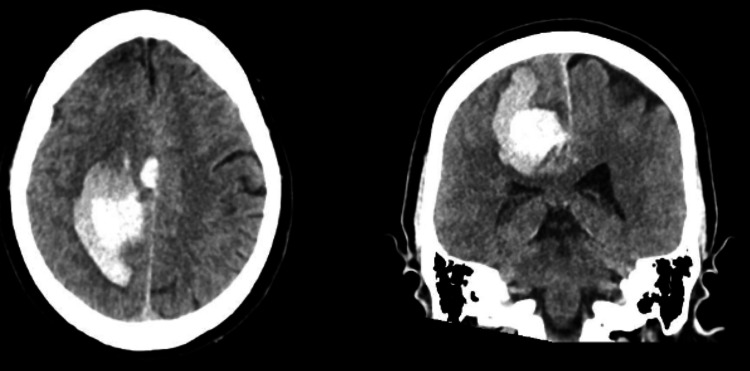 Figure 5
Figure 5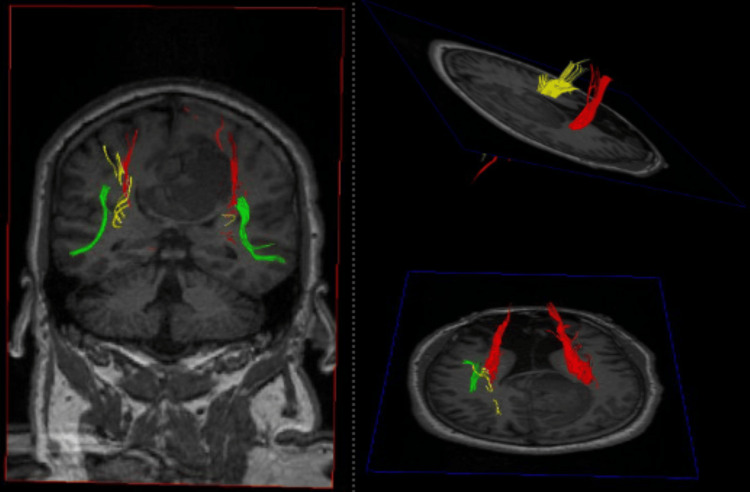 Figure 6
Figure 6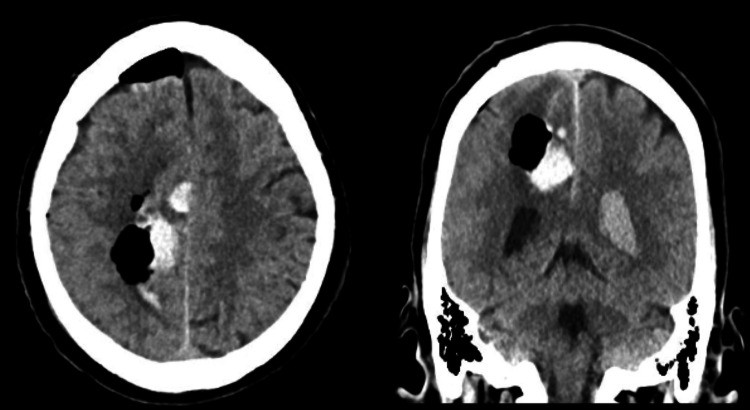 Figure 7
Figure 7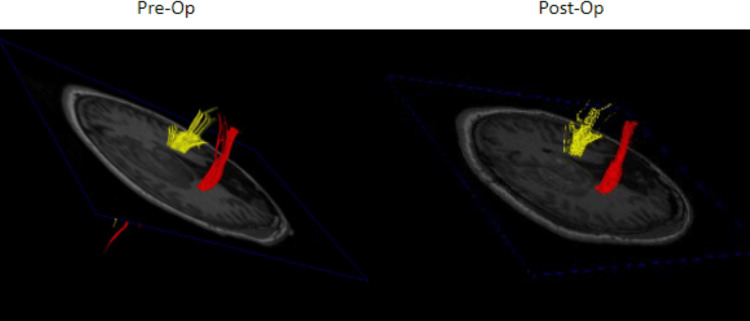 Figure 8
Figure 8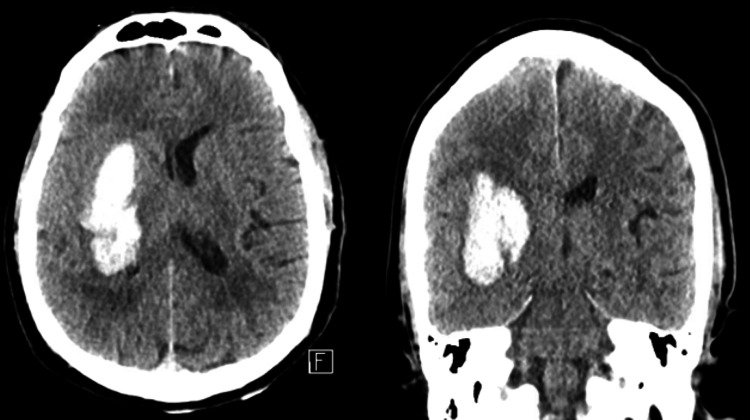 Figure 9
Figure 9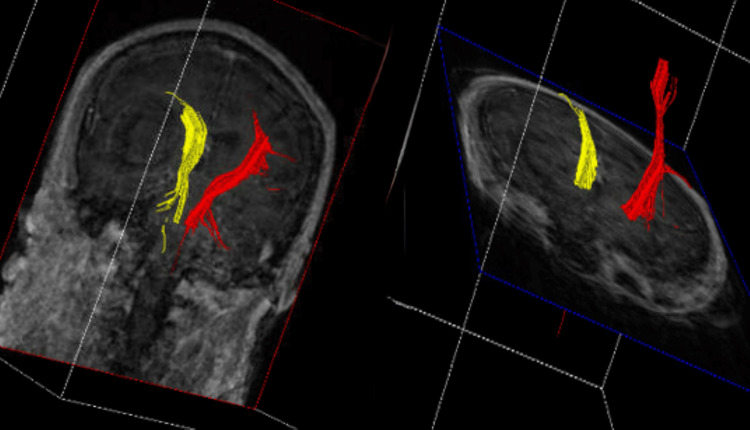 Figure 10
Figure 10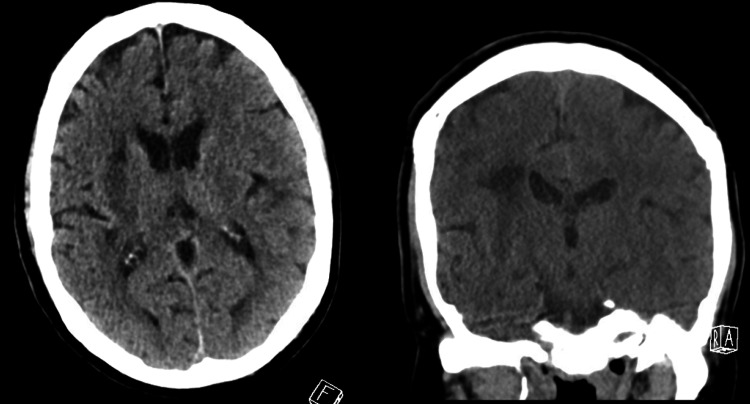 Figure 11
Figure 11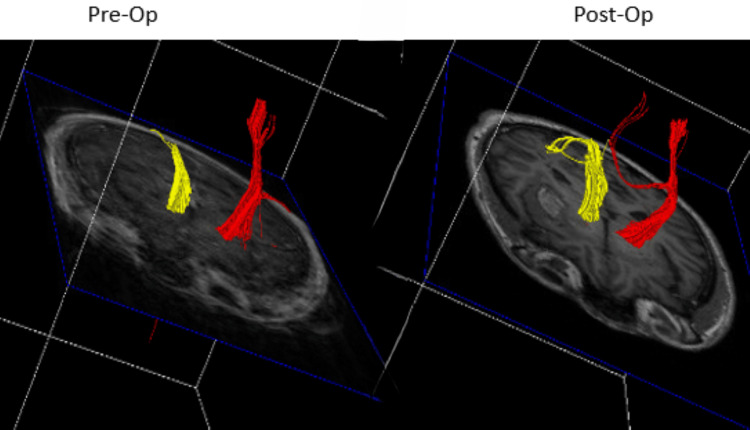 Figure 12
Figure 12| Patient | Age (in years)/Sex | Pre-operative FA ipsilateralCST mean | Pre-operative ADC ipsilateral CST mean | Post-operative FA ipsilateral CST mean | Post-operative ADC ipsilateral CST mean | Pre-operative FA contralateral CST mean | Pre-operative ADC contralateral CST mean | Post-operative FA contralateral CST mean | Post-operative ADC contralateral CST mean |
| 1 | 41/M | 0.5435 | 73.31 | 0.5683 | 71.67 | 0.6109 | 71.95 | 0.5744 | 70 |
| 2 | 52/M | 0.5927 | 64.39 | 0.5731 | 74.08 | 0.5494 | 71.89 | 0.5799 | 70.44 |
| 3 | 61/M | 0.3984 | 85.82 | 0.3421 | 77.84 | 0.5918 | 74.03 | 0.4624 | 74.24 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsIntracerebral and Subarachnoid Hemorrhage Research · Acute Ischemic Stroke Management · Neurosurgical Procedures and Complications
Introduction
Spontaneous intracerebral hemorrhage (sICH) is a source of significant morbidity and mortality. There are almost 80,000 cases of sICH per year in the US with an early mortality rate of 30-40%[1]. Growing evidence shows that motor outcome after stroke is heavily dependent on the integrity of the corticospinal tract (CST) [2]. Although large, superficial lesions (i.e., those within 1 cm of the cortical surface) can be readily evacuated to improve patient outcomes in certain circumstances, for subcortical lesions the current standard of care remains medical management [1]. Traditionally, subcortical lesions are approached via a large corticotomy using brain retractor blades that often cause significant white matter tract disruption. The concurrent cortical and subcortical trauma typically negates the potential benefits of hematoma removal. Multiple studies have shown that subcortical injuries are more severe than cortical injuries of the same volume [3-13]. Additionally, the inability to identify white matter tracts put them at risk of inadvertent injury.
New surgical techniques are being developed to improve outcomes in patients with subcortical lesions. One of these techniques utilizes the minimally invasive parafascicular approach to subcortical lesions [14,15]. Using stereotactic image guidance, a tubular retractor system is inserted through the cortex and subcortical tissue in a trans-sulcal manner. This approach reduces traction injury by the radial distribution of the retraction force and reduces parenchymal trauma by using a sulcus as a starting point rather than a gyrus. It also spares the projection fibers that originate from the gyri. The NICO Corporation (Indianapolis, IN, USA) has patented a system that facilitates this approach known as BrainPath. A recent study has shown improvement in functional outcomes using this device in patients with 30 to 80 milliliter (mL) hemorrhages [16]. Current national guidelines recommend considering evacuation of hemorrhages greater than 20-30 mL in patients with Glasgow Coma Scores (GCS) between 5 and 12 [1].
A novel adjunct to this technique is the use of diffuse tensor imaging 3D tractography (DTT) to identify subcortical white matter tracts so that they can be avoided during surgery. This tractography is derived from standard magnetic resonance imaging (MRI) sequences and processed using specialized software. Specifically, the major corticospinal tracts can be identified and avoided to reduce postoperative neurological deficits [7,15-20]. In this study, patients with subcortical intracerebral hemorrhages will undergo DTT to map out their corticospinal tracts prior to surgery. This information will guide the surgical approach to the clot. Additionally, DTT can be used postoperatively to evaluate the integrity of the CST to guide prognosis [21-23].
Case presentation
Methods
This study was approved by our institutional review board. We enrolled three patients who fit our inclusion criteria for minimally invasive sICH evacuation. They underwent pre-operative DTT, and the involvement/injury of the CST was graded from A to E, with A signifying direct injury (i.e., a disrupted CST) and the others (B, C, D, and E) signifying displacement in anatomic directions (anterior, posterior, medial, and lateral, respectively). Grading was performed by the senior author (DF) in conjunction with another author (YZ). Surgical trajectories were planned from three trans-sulcal approaches (anterior, posterior, and lateral) to avoid damage to the ipsilateral CST, and the surgery was performed with the BrainPath and Myriad devices (NICO Corporation, Indianapolis, IN, USA). The anterior corridor was defined as the junction of the superior frontal sulcus and precentral sulcus and runs parallel to the association fibers. Its course runs between the superior longitudinal fasciculus and the cingulum. The parieto-occipital sulcus demarcated the posterior corridor, and the superior temporal sulcus was used as the lateral corridor. Additionally, fractional anisotropy (FA) and apparent diffusion coefficient (ADC) values were calculated for both bilateral CSTs before and after surgery. The posterior limb of the internal capsule was the region of interest for these calculations. DTT processing was performed by one of our authors (YZ), a neuroradiologist with specialized training in DTT generation. DTT data were analyzed using Food and Drug Administration-approved software (NordicBrainEx, v.2.3.9, NordicNeuroLab).
All surgeries were performed by the senior author (DF) in a consecutive fashion. Patients were positioned supine in 3-point fixation with a head clamp. Medtronic (Dublin, Ireland) Stealth navigation was used to mark out an appropriate corridor to the hematoma. A 3.5 cm craniotomy was used in all surgeries to place a BrainPath sheath, and the hematomas were evacuated using the Myriad device under microscope visualization. The goal of surgery was a residual hematoma volume of less than 15 mL, which is a common goal for evacuation in other trials [14]. After surgery, three patients underwent a second DTT imaging for assessment of their CSTs after surgery. All patients were followed clinically for improvement in their motor function. Demographic information was collected on all patients, and the patients have been followed clinically for at least three months.
Case 1
A 41-year-old male with a history of methamphetamine abuse presented to the emergency department after he developed confusion and sudden right-sided weakness associated with right-sided facial droop. He had taken methamphetamine that evening when his symptoms started. He was intubated in the emergency department for airway protection. His exam was GCS 1/1T/5 with localization in his left upper/lower extremities and extensor posturing of his right-sided extremities. His initial computed tomography (CT) scan was consistent with a large left-sided subcortical sICH (about 45 mL in volume, Figure 1). Preoperative DTT demonstrated medical displacement of his CST (Grade D injury to the CST, Figure 2). A left frontal approach was selected, and the corridor and the hematoma were evacuated using a 75 mm BrainPath sheath. Postoperative CT was consistent with the satisfactory evacuation of the hematoma (Figure 3, residual hematoma volume of 6 mL). Additionally, repeat DTT after surgery was consistent with improved integrity of the ipsilateral CST (Figure 4). Both FA and ADC values increased after surgery, again consistent with improved integrity of the CST (Table 1). The patient recovered from his sICH well, and his last examination revealed almost full strength in his right lower extremity (strength grade 4/5) and some movement in his right arm (strength grade 1/5).
Preoperative CT scan for patient 1CT scan with a left basal ganglia intracerebral hemorrhage (ICH)
Preoperative DTT for patient 1Preoperative DTT demonstrating injury to the left CST (yellow)DTT: Diffusion tensor imaging tractography, CST: Cortical spinal tract
Post-operative CT scan for patient 1CT scan with a left basal ganglia intracerebral hemorrhage (ICH)
Pre- and post-operative DTT for patient 1 showing increased conspicuity of the ipsilateral CSTPre- and post-operative DTT demonstrating increased connectivity of the CST after evacuation of the ICH.DTT: DTI/tractography, CST: Cortical spinal tract, ICH: Intracerebral hemorrhage
Case 2
A 52-year-old male with a history of cocaine abuse presented to the emergency department with acute onset left arm and leg weakness. On his initial exam, he was GCS 4/4/6 with 1/5 strength in his left upper and lower extremities. His initial CT head demonstrated a large right frontal sICH (about 71 mL in volume, Figure 5). His pre-operative DTT was consistent with a Grade A (direct involvement) injury to the ipsilateral CST (Figure 6). The posterior corridor and a 60 mm BrainPath sheath were used to evacuate his hematoma because the remaining ipsilateral CST was displaced anteriorly and laterally. Post-operative CTH was consistent with a satisfactory evacuation (end of treatment volume of 11 mL), but post-operative DTT did not show improvement in the ipsilateral CST (Figures 7, 8). FA values decreased after surgery on the right side but increased on the left. ADC values increased on the right side but decreased on the left side (Table 1). He did well after surgery, but he did not regain voluntary movement of his left upper and lower extremities (he remained with 1/5 strength in those extremities).
Preoperative CT scan for patient 2Preoperative CT scan with a significant right frontal sICHsICH: Spontaneous intracerebral hemorrhage
Preoperative DTT for patient 2Preoperative DTT showing significant injury to the ipsilateral CST from the sICHDTT: DTI/tractography, CST: corticospinal tract, sICH: spontaneous intracerebral hemorrhage
Post-operative CT scan for patient 2Post-operative CT scan demonstrating excellent evacuation of the right frontal sICHsICH: Spontaneous intracerebral hemorrhage
Pre- and post-operative DTT for patient 2Comparison of pre- and post-operative DTT showing largely unchanged connectivity of the right-sided CSTDTT: DTI/tractography, CST: Corticospinal tract
Case 3
A 61-year-old male with a history of methamphetamine abuse presented to the emergency department with acute onset left arm and leg weakness. He was GCS 4/5/6 with 2/5 strength in his left arm and left leg. He was initially found to have a 15 mL right basal ganglia hemorrhage that expanded to 35 mL, and he became significantly weaker in his left hemibody (Figure 9). His mental status deteriorated, and his GCS became 2/3/6. His DTT was consistent with a Grade A injury (direct involvement, Figure 10). He was taken to the operating room for evacuation of his hematoma using the anterior corridor. A 75 mm BrainPath sheath was used in this case, and an end-of-treatment volume of 7 mL was achieved (Figure 11). His mental status improved after surgery, but he remained at 2/5 strength in his left-sided extremities. Post-operative DTT did not show significant improvement in the ipsilateral CST (Figure 12). Ipsilateral FA values also did not increase after surgery.
Pre-operative CT scan for patient 3CT scan showing a large right basal ganglia ICHICH: Intracerebral hemorrhage
Pre-operative DTT for patient 3Pre-operative DTT demonstrating injury to the ipsilateral CSTDTT: DTI/tractography, CST: Corticospinal tract
Post-operative CT scan for patient 3Post-operative CT scan with complete evacuation of sICHsICH: Spontaneous intracerebral hemorrhage
Pre- and post-operative DTT for patient 3Comparison of pre- and post-operative DTT showing similar CST connectivity after evacuation of sICHDTT: DTI/tractography, CST: Corticospinal tract, sICH: spontaneous intracerebral hemorrhage
Discussion
Our study demonstrates the feasibility and safety of DTI-guided, trans-sulcal minimally invasive surgery (MIS) using the BrainPath/Myriad system for spontaneous intracerebral hemorrhage (sICH) evacuation in a small cohort of patients. The integration of diffusion tensor imaging tractography (DTT) proved invaluable in surgical planning, allowing for the identification and avoidance of critical corticospinal tract (CST) pathways. This approach aligns with the growing recognition of the importance of preserving white matter integrity during sICH surgery, as evidenced by studies highlighting the detrimental impact of traditional open surgical techniques that often disrupt these pathways [11-13].
The ability of DTT to visualize the CST and classify the extent of injury (Grade A to E) facilitated the selection of optimal surgical corridors. In our case series, the anterior, posterior, and lateral trans-sulcal approaches were successfully employed, demonstrating the versatility of this technique. Notably, in Case 2, the posterior approach was crucial in avoiding further damage to the anteriorly and laterally displaced CST. This highlights the potential of DTT to tailor surgical strategies based on individual patient anatomy and pathology.
When considering surgical intervention for sICH, it's essential to contextualize our findings within the broader landscape of clinical trials. The STICH (surgical trial in intracerebral hemorrhage) and STICH II trials have significantly influenced the management of sICH [12,13]. These trials, while showing limited overall benefit from early surgery compared to conservative management, highlighted the complexity of sICH management and the importance of patient selection. Specifically, STICH II suggested potential benefits in patients with superficial lobar hemorrhages without intraventricular hemorrhage. However, both STICH trials relied on conventional surgical techniques, which often involve larger craniotomies and greater disruption of surrounding brain tissue.
Our study differs significantly in its utilization of minimally invasive techniques guided by DTT. We hypothesized that this approach, by minimizing tissue disruption and preserving critical white matter tracts, would improve outcomes compared to conventional surgery. The ENRICH trial, a more recent study evaluating MIS for sICH, demonstrated the benefits of lobar hemorrhages but met futility criteria for basal ganglia hemorrhages [16]. Crucially, the ENRICH trial, like the STICH trials, did not incorporate DTT for surgical planning. Our study, however, proactively utilized DTT to avoid the CST, which we hypothesized would improve outcomes. However, the limited data in our study, with patients who had direct CST involvement (Grade A) showing limited motor recovery, suggest that direct CST disruption may be a poor prognostic factor, regardless of surgical technique.
The changes observed in fractional anisotropy (FA) and apparent diffusion coefficient (ADC) values postoperatively provide insights into CST integrity. Increases in FA and decreases in ADC are typically associated with improved white matter organization and reduced edema, respectively. In case 1, the observed improvements in these metrics correlated with some degree of motor recovery. However, in cases 2 and 3, where direct CST injury was noted, the postoperative DTT and FA/ADC values did not show significant improvement, mirroring the lack of clinical motor recovery. This suggests that DTT may serve as a valuable tool for predicting motor outcomes postoperatively, allowing for more realistic patient and family counseling.
Several limitations must be acknowledged. First, the small sample size (n=3) restricts the generalizability of our findings and underscores the need for larger, multi-center studies. Second, the patient population, primarily middle-aged males with a history of sympathomimetic abuse, may not be representative of the broader sICH population, potentially introducing selection bias. Third, the absence of a control group limits our ability to definitively attribute the observed outcomes to the DTT-guided MIS technique. Future studies should include a control group (e.g., medical management, traditional surgery) to provide a more rigorous comparison. Fourth, while motor function was assessed, a more standardized and comprehensive assessment of functional outcomes using established scales such as the modified Rankin Scale or Barthel Index would enhance the study's rigor.
Despite these limitations, our study provides valuable preliminary evidence supporting the feasibility and potential benefits of DTT-guided, trans-sulcal MIS for sICH. Further research is warranted to validate these findings in larger, more diverse patient populations and to explore the long-term impact of this technique on functional recovery. Future studies should also explore the relationship between DTT metrics and functional outcomes in greater detail, potentially leading to the development of predictive models for personalized sICH management. Additionally, future trials should compare DTT-guided MIS directly against conservative management, and conventional surgical techniques, as used in the STICH trials, to understand if this new technique provides significant benefit.
Conclusions
Based on our small sample size, using DTT in conjunction with MIS evacuation of sICH using the BrainPath/Myriad devices is feasible and safe. The information derived from DTT is useful both for surgical planning and may offer helpful prognostic information for recovery of motor function after sICH evacuation. We will use the data from this preliminary study to optimize our workflow and plan for larger studies involving more patients to see if using DTT-guided, trans-sulcal therapy will improve patient outcomes and lead to less post-operative motor deficits.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 12022 guideline for the management of patients with spontaneous intracerebral hemorrhage: a guideline from the American Heart Association/American stroke association Stroke Greenberg SM Ziai WC Cordonnier C 036153202210.1161/STR.000000000000040735579034 · doi ↗ · pubmed ↗
- 2Corticospinal tract compression by hematoma in a patient with intracerebral hemorrhage: a diffusion tensor tractography and functional MRI study Yonsei Med J Jang SH Kwon YH Lee MY 1351394720061650249610.3349/ymj.2006.47.1.135PMC 2687571 · doi ↗ · pubmed ↗
- 3Prediction of upper extremity motor recovery after subacute intracerebral hemorrhage through diffusion tensor imaging: a systematic review and meta-analysis Neuroradiology Kumar P Yadav AK Misra S 104310505820162743880210.1007/s 00234-016-1718-6 · doi ↗ · pubmed ↗
- 4Prediction of motor function outcome after intracerebral hemorrhage using fractional anisotropy calculated from diffusion tensor imaging Cerebrovasc Dis Kuzu Y Inoue T Kanbara Y 5665733320122268813710.1159/000338904 · doi ↗ · pubmed ↗
- 5White and gray matter contributions to executive function recovery after traumatic brain injury Neurology Cristofori I Zhong W Chau A 139414018420152574655810.1212/WNL.0000000000001446 PMC 4395886 · doi ↗ · pubmed ↗
- 6Cognitive impairment after focal brain lesions is better predicted by damage to structural than functional network hubs Proc Natl Acad Sci U S A Reber J Hwang K Bowren M 118202110.1073/pnas.2018784118 PMC 812686033941692 · doi ↗ · pubmed ↗
- 7Prediction of functional outcome in acute cerebral hemorrhage using diffusion tensor imaging at 3T: a prospective study AJNR Am J Neuroradiol Kusano Y Seguchi T Horiuchi T 156115653020091955635410.3174/ajnr.A 1639 PMC 7051627 · doi ↗ · pubmed ↗
- 8Recovery of a partially damaged corticospinal tract in a patient with intracerebral hemorrhage: a diffusion tensor image study Restor Neurol Neurosci Jang SH Byun WM Han BS 2529242006 https://pubmed.ncbi.nlm.nih.gov/16518025/16518025 · pubmed ↗