Impact of Barbed Suture Closure on Vaginal Cuff Dehiscence Following Robot-Assisted Total Hysterectomy: A Retrospective Cohort Study
Shinichi Togami, Furuzono Nozomi, Yusuke Kobayashi, Mika Fukuda, Mika Mizuno, Shintaro Yanazume, Hiroaki Kobayashi

TL;DR
This study found that using barbed sutures during robot-assisted hysterectomy safely prevents vaginal cuff dehiscence in the six months after surgery.
Contribution
Demonstrates the safety and feasibility of barbed suture closure in reducing vaginal cuff dehiscence after robot-assisted hysterectomy.
Findings
No cases of vaginal cuff dehiscence were observed in 313 patients over six months.
Barbed sutures provided consistent outcomes in high-volume robotic surgery settings.
The standardized surgical approach using barbed sutures was feasible and safe.
Abstract
Introduction Vaginal cuff dehiscence (VCD) is a rare but serious complication following hysterectomy, with a higher incidence in minimally invasive surgery (MIS). The choice of suture material and closure technique may influence the risk of VCD. Barbed sutures, such as STRATAFIX™ Spiral PDS Plus, enhance tissue approximation and eliminate the need for knot tying, potentially improving wound healing. This study aimed to evaluate the incidence of VCD following robot-assisted total hysterectomy (RAH) with vaginal cuff closure using barbed sutures. Methods This retrospective cohort study included patients who underwent RAH at Kagoshima University Hospital between July 2017 and July 2024. Patients who had vaginal cuff closure with barbed sutures were analyzed, while those who underwent supracervical hysterectomy or had vaginal cuff closure with non-barbed sutures were excluded. VCD was…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1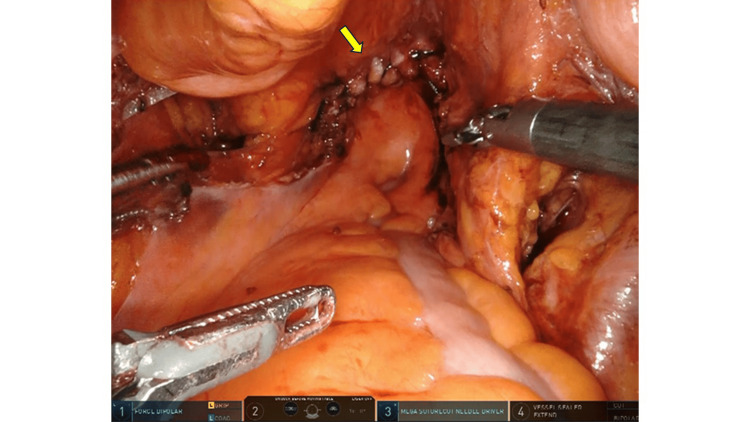 Figure 2
Figure 2| Characteristics | Patients (n = 313) |
| Median age (years) | 55 (28-86) |
| Median BMI (kg/m²) | 28 (17.3-53.1) |
| Surgery indication | |
| Benign disease | 43 (14%) |
| Malignant disease | 270 (86%) |
| Median operation time (min) | 201 (range: 68-638) |
| Median cockpit/console time (min) | 148 (range: 53-520) |
| Median blood loss (mL) | 20 (range: 5-685) |
| Median length of hospital stay (days) | 6 (range: 3-22) |
| Robotic type | |
| da Vinci® Xi | 268 (86%) |
| hinotori™ Surgical Robot System | 45 (14%) |
| Retroperitoneal suture | |
| No | 89 (28%) |
| Yes | 224 (72%) |
| VCD | |
| No | 313 (100%) |
| Yes | 0 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsUterine Myomas and Treatments · Maternal and fetal healthcare · Reconstructive Surgery and Microvascular Techniques
Introduction
Hysterectomy is a commonly performed gynecologic procedure used to treat both benign and malignant conditions. Various surgical approaches are available, including abdominal hysterectomy, laparoscopic hysterectomy (LH), robot-assisted total hysterectomy (RAH), and vaginal hysterectomy. With the increasing adoption of minimally invasive surgery (MIS), LH and RAH have gained prominence due to their advantages, such as reduced postoperative pain, shorter hospital stays, and faster recovery [1,2]. However, the growing prevalence of MIS has been linked to a higher incidence of vaginal cuff dehiscence (VCD), emphasizing the need for effective prevention and management strategies [3-5].
The incidence of VCD varies by surgical approach, with MIS procedures carrying a higher risk compared to open surgery. Studies have reported a VCD incidence of 0.75% following LH, which is greater than the 0.38% observed after abdominal hysterectomy [6]. VCD is believed to result from impaired wound healing at the vaginal cuff and excessive mechanical stress, which can lead to bowel evisceration - a severe complication requiring emergent surgical intervention due to the risk of bowel ischemia and necrosis. Several documented cases of bowel evisceration following VCD highlight its clinical significance.
Multiple risk factors for VCD have been identified, including patient-related factors such as vaginal hematoma, smoking, and chronic constipation, all of which negatively impact wound healing [7,8]. Additionally, postoperative factors, such as early resumption of sexual activity and increased intra-abdominal pressure from coughing or straining during defecation, contribute to VCD occurrence [8]. Surgical factors, including the surgical approach, suture technique, and type of energy device used for colpotomy, further influence VCD risk. However, no consensus exists on the optimal technique to minimize its occurrence.
STRATAFIX^™^ Spiral PDS Plus is a knotless, absorbable barbed suture with a 360° spiral configuration of barbs along its surface and is impregnated with triclosan, an antimicrobial agent. This novel suture design enhances tissue approximation and eliminates the need for knot tying, potentially improving wound healing. This study aimed to evaluate the incidence of VCD following RAH with vaginal cuff closure using STRATAFIX^™^ Spiral PDS Plus, assessing its efficacy and safety in VCD prevention.
Materials and methods
Study overview
This single-center retrospective cohort study was conducted at Kagoshima University Hospital to evaluate the incidence of VCD following RAH with vaginal cuff closure using barbed sutures.
Ethical considerations
The study was approved by the Institutional Review Board of Kagoshima University Hospital (IRB approval no. 20-K04). Due to its retrospective design and the use of anonymized data extracted from electronic medical records, the requirement for informed consent was waived.
Study criteria
Patients who underwent RAH with vaginal cuff closure using barbed sutures (STRATAFIX™ Spiral PDS Plus) between July 2017 and July 2024 were included in the study. Patients who underwent supracervical hysterectomy or those in whom barbed sutures were not used for vaginal cuff closure were excluded.
Surgical procedure
All surgeries were performed by four certified gynecologic oncologists from the Japan Society of Gynecologic Oncology. Among them, two were board-certified laparoscopic surgeons accredited by the Japan Society of Gynecologic and Obstetric Endoscopy. Additionally, all four surgeons held certifications for the da Vinci® Xi and hinotori™ Surgical Robot System.
Colpotomy was performed using monopolar scissors in coagulation mode at 35 watts to create a circumferential incision. Vaginal cuff closure began with the placement of interrupted 0-Polyglactin 910 sutures at both lateral ends, followed by a continuous barbed suture using STRATAFIX™ Spiral PDS Plus. Retroperitoneal closure was performed at the surgeon’s discretion (Figure 1, Figure 2).
Vaginal cuff closure using a barbed suture with retroperitoneal closureThe arrow indicates the area where retroperitoneal suturing was performed following vaginal cuff closure.
Vaginal cuff closure using a barbed suture without retroperitoneal closureThe arrow indicates the site of vaginal cuff closure where retroperitoneal suturing was not performed.
Assessments
The presence or absence of VCD was assessed through routine pelvic examinations performed at one, three, and six months postoperatively, or earlier if clinically indicated. If a patient underwent a pelvic examination for other reasons within six months after surgery, those findings were also reviewed. If no VCD was detected during the six-month postoperative period, the patient was considered VCD-negative for the purpose of this study. All examinations were conducted by attending gynecologists and documented in the electronic medical records.
Sample size calculation
Since this study aimed to determine the incidence of a rare event (VCD), all eligible patients during the seven-year study period were included. A formal sample size calculation was not performed.
Statistical analysis
Descriptive statistics were used to summarize clinical characteristics and outcomes. As no cases of VCD were observed, a one-sided 97.5% CI for a zero-event proportion was calculated, resulting in an upper limit of 1.15%. This estimation provides a statistical boundary for the true incidence of VCD in this population.
All statistical analyses were performed using JMP version 14 (SAS Institute Inc., Cary, NC, USA).
Results
A total of 313 patients who underwent RAH were analyzed to assess the incidence of VCD following barbed suture closure (Table 1).
The median age of the patients was 55 years (range: 28-86 years), and the median BMI was 28 kg/m² (range: 17.3-53.1 kg/m²). Surgical indications included malignant tumors in 270 patients (86%) and benign conditions in 43 patients (14%).
The median operation time was 201 minutes (range: 68-638 minutes), with a median console/cockpit time of 148 minutes (range: 53-520 minutes). The median estimated blood loss was 20 mL (range: 5-685 mL), and the median length of hospital stay was six days (range: 3-22 days).
Two robotic platforms were used in this study: the da Vinci^®^ Xi system in 268 patients (86%) and the hinotori^™^ Surgical Robot System in 45 patients (14%). Retroperitoneal suturing was performed in 224 patients (72%). No cases of VCD were identified within the six-month postoperative period among the 313 patients. The calculated one-sided 97.5% CI for a zero-event proportion was 0-1.15%, indicating that the true incidence of VCD in this cohort is likely below 1.15%.
Discussion
This study investigated the incidence of VCD within six months postoperatively in patients who underwent RAH with vaginal cuff closure using barbed sutures. Among the 313 patients, no cases of VCD were observed during the defined follow-up period, regardless of age, BMI, or retroperitoneal suturing status.
The reported incidence of VCD following MIS varies, with rates ranging from 0.32% to 1.0% in LH and from 0.22% to 1.49% in RAH [9-14]. However, in our study, VCD did not occur in any of the 313 patients. Among the surgical risk factors for VCD in MIS, narrow suture width resulting from magnified visualization has been proposed as a potential contributor. Fuchs Weizman et al. [8] compared interrupted and continuous suturing techniques and concluded that continuous suturing reduced the risk of VCD. Similarly, Uccella et al. [15] reported that barbed sutures were associated with a lower risk of VCD compared with non-barbed closure. In contrast, Cannone et al. [16] found no significant difference in VCD risk between Vicryl and PDS sutures. These findings suggest that barbed suture closure during RAH may contribute to a lower incidence of VCD. The six-month follow-up period was chosen based on previous studies indicating that the majority of VCD events occur within the first three to six months after surgery [12,15]. Therefore, this time frame was deemed appropriate for capturing clinically relevant VCD events while ensuring consistency in outcome assessment.
Few studies have examined the relationship between VCD and retroperitoneal suturing. Hada et al. [9] evaluated 677 patients with LH and identified VCD in four patients (0.6%), but found no statistical correlation between retroperitoneal suturing and VCD. Similarly, our study found no cases of VCD in the 89 patients (28%) without retroperitoneal suturing, supporting the findings of Hada et al. [9].
Another debated factor in MIS-associated VCD is the use of energy devices for colpotomy. Previous studies have investigated whether energy-based colpotomy increases the risk of vaginal cuff separation. Taşkın et al. [11] compared monopolar coagulation and cut mode and found no significant difference in VCD incidence. Similarly, another study found no significant difference in VCD occurrence when colpotomy was performed using a cold scalpel, advanced bipolar devices, monopolar electrosurgery, or a harmonic scalpel [8]. In our study, monopolar colpotomy was performed in all patients, with no VCD observed. This suggests that monopolar energy use may not be a significant risk factor for VCD.
This study has notable strengths. All patients underwent a uniform surgical procedure - RAH with barbed suture closure - performed by experienced surgeons at a single center. This consistency reduces variability and strengthens the internal validity of the findings. The relatively large cohort over a seven-year period also enables a reliable estimation of VCD incidence, a rare postoperative complication. A retrospective design was chosen because VCD is rare, and data were readily available from electronic medical records. A prospective study would have been time-consuming and less practical for this objective.
However, limitations include the potential underreporting of asymptomatic VCD due to reliance on chart documentation. Additionally, the absence of a control group limits direct comparison with other suture methods, and the single-center setting may affect the generalizability of the findings. Despite these limitations, the absence of VCD in this large, homogeneous cohort supports the safety and feasibility of barbed suture closure in RAH.
Conclusions
In this retrospective cohort study, no cases of VCD were observed within the six-month postoperative period among 313 patients who underwent RAH with barbed suture closure. Given that previous studies have shown that most VCD events occur within three to six months after surgery, this time frame was considered clinically appropriate for capturing relevant outcomes. The findings suggest that barbed suture closure may be a safe and effective technique for preventing VCD in robotic hysterectomy, irrespective of patient age, BMI, or retroperitoneal suturing. While the study is limited by its retrospective design and the absence of a comparison group, the use of a standardized surgical approach and consistent follow-up enhances the reliability of the results. Further prospective studies with longer-term follow-up are needed to confirm these findings and assess long-term safety.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Comparative effectiveness of minimally invasive hysterectomy for endometrial cancer J Clin Oncol Wright JD Burke WM Tergas AI 108710963420162683405710.1200/JCO.2015.65.3212 PMC 4872018 · doi ↗ · pubmed ↗
- 2Robot-assisted versus conventional laparoscopic hysterectomy in endometrial cancer: an observational study in a French tertiary teaching hospital at the beginning of the learning curve J Gynecol Obstet Hum Reprod Bajeux E Hamonic S Brunet-Houdard S Nyangoh Timoh K Dion L Guecheff A Lavoue V 1029175420253989251910.1016/j.jogoh.2025.102917 · doi ↗ · pubmed ↗
- 3Two cases of post-coital vaginal cuff dehiscence with small bowel evisceration after robotic-assisted laparoscopic hysterectomy Int J Surg Case Rep Nguyen ML Kapoor M Pradhan TS Pua TL Tedjarati SS 603605420132370830610.1016/j.ijscr.2013.04.001PMC 3679435 · doi ↗ · pubmed ↗
- 4Delayed postcoital vaginal cuff dehiscence with small bowel evisceration after robotic-assisted staging surgery Taiwan J Obstet Gynecol Lan YP Chen HH Liu WM Chen CH 2582605620172842052110.1016/j.tjog.2016.02.022 · doi ↗ · pubmed ↗
- 5Vaginal cuff dehiscence with bowel evisceration after robotic hysterectomy Turk J Obstet Gynecol Akdemir A Taylan E Ergenoğlu AM Yeniel AÖ ŞendağF Öztekin MK 2492511120142891303010.4274/tjod.47640 PMC 5558371 · doi ↗ · pubmed ↗
- 6Vaginal cuff dehiscence after different modes of hysterectomy Obstet Gynecol Hur HC Donnellan N Mansuria S Barber RE Guido R Lee T 79480111820112193444210.1097/AOG.0b 013e 31822 f 1c 92 · doi ↗ · pubmed ↗
- 7Trends and risk factors for vaginal cuff dehiscence after laparoscopic hysterectomy J Minim Invasive Gynecol Das D Sinha A Yao M Michener CM 9919992820213292014510.1016/j.jmig.2020.09.005 · doi ↗ · pubmed ↗
- 8Vaginal cuff dehiscence: risk factors and associated morbidities JSLS Fuchs Weizman N Einarsson JI Wang KC Vitonis AF Cohen SL 19201510.4293/JSLS.2013.00351 PMC 439605425901104 · doi ↗ · pubmed ↗