Massive Ovarian Oedema in Pregnancy: A Diagnostic Dilemma
Jaice M Devasia, Bharathi D Rao

TL;DR
A pregnant woman presented with a rare condition called massive ovarian oedema, which was difficult to diagnose and required multiple tests to confirm.
Contribution
This case report highlights the diagnostic challenges of massive ovarian oedema during pregnancy and its potential misdiagnosis as ectopic pregnancy.
Findings
Massive ovarian oedema was confirmed histologically after imaging and blood tests failed to provide a definitive diagnosis.
The condition presented as a pelvic mass with imaging features resembling an ectopic pregnancy.
Medical termination and exploratory surgery were necessary to reach a conclusive diagnosis.
Abstract
Massive oedema of the ovary is a rare clinical entity and poses a clinical challenge due to the potential for misdiagnosis. This is a case of a 27-year-old pregnant woman with incidentally detected ovarian oedema on routine dating scan. She was asymptomatic. Clinical examination revealed a midline pelvic mass, which was firm to hard in consistency, corresponding to a 14-week size of a gravid uterus. After medical termination as requested by the patient, further imaging was done. Contrast-enhanced CT showed a well-defined cystic lesion in the left adnexa with a thick, irregular enhancing wall and multiple intensely enhancing tortuous tufts of vessels seen from the ovarian artery and draining into the left ovarian vein, likely of old ovarian ectopic pregnancy. Hence, a beta-human chorionic gonadotropin test was done to rule out ectopic pregnancy. The patient underwent exploratory…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
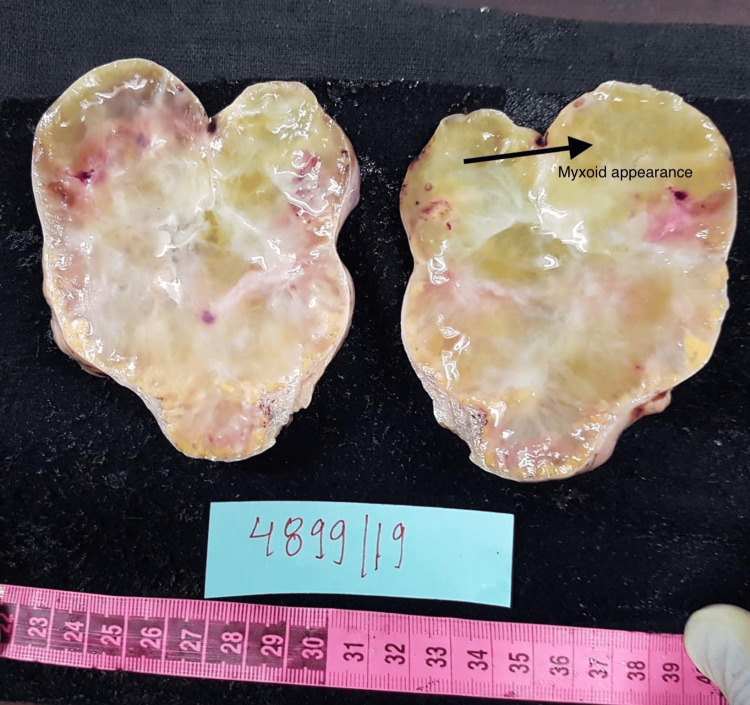 Figure 1
Figure 1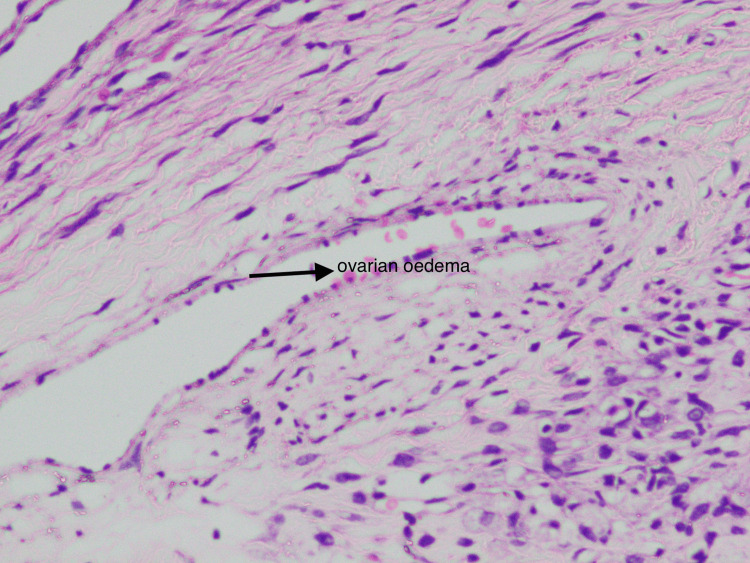 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOvarian function and disorders · Reproductive Biology and Fertility · Ovarian cancer diagnosis and treatment
Introduction
Massive oedema of the ovary is a rare clinical entity. Most commonly, young women are affected [1]. Massive oedema can involve one or both ovaries. It was first described by Kalstone et al. in 1969 [2]. Though the aetiology is unclear, it is suggested that the massive oedema of the ovary results from interference of venous and lymphatic flow due to partial or complete torsion of the mesovarium [1]. It is important to diagnose this condition as it is usually misdiagnosed as malignancy, and young women undergo aggressive treatment, which results in loss of hormonal function and infertility [1]. Only very few cases of massive ovarian oedema have been published from the Indian population.
This case report was presented as a poster at the Karnataka State Obstetrics & Gynaecology Association in September 2019.
Case presentation
This is a case of a 27-year-old gravida 2 para 1 living 1 female at six weeks and one day of gestation, with a history of previous lower segment caesarean section. She was referred to the department in view of an ultrasonography report, showing an ovarian mass for evaluation, which was incidentally detected. The patient was asymptomatic. Clinical examination revealed an abdominal mass of 14 weeks' size of a gravid uterus, which was firm to hard in consistency. Cancer antigen 125 (CA-125) was 24.5 IU/ml. Ultrasonography done in our hospital showed features suggestive of a left ovarian mass of 8.5 x 5.2 cm with moderate ascites. Medical termination of pregnancy was done as requested by the patient. After the termination of pregnancy, a contrast-enhanced CT of the abdomen and pelvis was done, which showed a well-defined cystic lesion in the left adnexa with a thick, irregular enhancing wall and multiple intensely enhancing tortuous tufts of vessels seen from the ovarian artery and draining into the left ovarian vein, likely of old ovarian ectopic pregnancy. Hence, a beta-human chorionic gonadotropin test was done. It was 2540 IU/mL, and the repeated value after 48 hours was 999 IU/mL. A conclusive diagnosis could not be reached by clinical examination and imaging. The patient was informed about the dilemma in diagnosis. She was informed about the possibility of ovarian malignancy and the need for surgery. She was also informed about the possible impact on fertility after removing the affected ovary. She underwent exploratory laparotomy with left salpingo-oophorectomy after informed consent. The gross appearance of the specimen suggested it could be an ovarian neoplasm. On the cut surface, a gelatinous, homogenous soft surface with yellowish areas was noted (Figure 1). Histopathological examination showed marked oedema of the stroma, which appeared to be pale with prominent vascular channels in the deeper cortex, and medulla was present with clusters of luteinized cells in the periphery (Figure 2). Histological analysis finally revealed it to be a massive oedema of the left ovary.
Cut surface of the ovary.Almost featureless and myxoid.
Microscopic appearance.Marked oedema and abnormally prominent vascular and lymphatic channels.
Discussion
Massive ovarian oedema is a rare clinical entity exhibiting gross enlargement of one or both ovaries as a result of the accumulation of oedema fluid in the stroma, causing separation of follicular structures [3]. Venous and lymphatic drainage is compromised, but it does not cause ischemic necrosis as the arterial supply is unaffected [3]. It is most commonly seen in women in their second and third decades. The most common presentation is acute abdomen [3], whereas, in our case, the patient was asymptomatic. Other common presentations could be abdominal distension, menstrual irregularities, and infertility [4]. Contrast-enhanced CT done in our hospital showed features suspicious of an old ectopic, which has not been seen in any of the articles reviewed. That gave us an inconclusive diagnosis. There is stromal luteinization, which can lead to masculinization in adult females and precocious puberty in prepubertal girls [5]. Kalstone et al. suggested that luteinization could be due to stretching of the stroma by the fluid oedema, which acts as a mechanical stimulus [2]. On gross appearance, an enlarged ovary with a soft, pearly external surface can be seen. Cut surface is almost featureless and myxoid, which was similar to our case [5]. The typical histological features are diffuse oedema of the medulla and inner cortex, which were seen in our case as well [5]. Superficial cortex and tunica albuginea are relatively spared. Abnormally prominent vascular and lymphatic channels are present [5], which is similar to our case. Foci of fibromatosis have been seen in massive ovarian oedema in some studies [6]. An intra-operative frozen section is always valuable at the time of surgery, as it can assist in performing fertility sparing surgery [1]. Intraoperative frozen section was not performed in our case. Unilateral salpingo-oophorectomy has been traditionally done in massive ovarian oedema. It could be due to failure to consider the diagnosis preoperatively [5]. This was the same with our case as well. An extensive study done by Praveen et al. identified that the majority of the patients have been over-treated with salpingo-oophorectomy due to a mistaken diagnosis of malignancy [7]. When the condition of ovarian oedema is suspected, wedge resection with the removal of 30% or more tissue is the appropriate treatment [4]. Although wedge resection may negatively affect fertility due to adhesion formation, it is a better management option than the removal of ovaries [7]. A study done by Cheng et al. reported that with detorsion, wedge resection, and plication of the ovary, the patient was successfully relieved of abdominal pain and experienced no recurrence during the follow-up period [4]. Praveen et al. performed intraoperative frozen section. Once the diagnosis of massive ovarian oedema was made, an ovarian decompression by ovarian drilling, followed by wedge resection and reconstruction of the distorted ovary with redundant capsule close to normal, was performed with great success [7].
Conclusions
This case report illustrates the challenges in diagnosing ovarian oedema. Though a rare clinical entity, massive oedema of the ovary should be suspected in young individuals presenting with an ovarian mass. It should be considered as a differential diagnosis to avoid aggressive treatment in young patients. Intraoperative frozen section can play a pivotal role in diagnosis and conservative management. Conservative options like wedge resection with fixation of the ovary would be more appropriate, as it preserves ovarian function and fertility.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Massive ovarian edema: a case report presenting as a diagnostic dilemma J Family Med Prim Care Varma A Chakrabarti PR Gupta G Kiyawat P 172174520162745386810.4103/2249-4863.184658 PMC 4943131 · doi ↗ · pubmed ↗
- 2Massive edema of the ovary simulating fibroma Obstet Gynecol Kalstone CE Jaffe RB Abell MR 564571341969 https://pubmed.ncbi.nlm.nih.gov/5822682/5822682 · pubmed ↗
- 3Massive ovarian oedema: a case report Obstet Gynecol Int J Escayola C Ripoll G Cardesa A Torrent JJ 34434592018 https://medcraveonline.com/OGIJ/massive-ovarian-oedema-a-case-report.html
- 4Laparoscopic plication of partially twisted ovary with massive ovarian edema J Chin Med Assoc Cheng MH Tseng JY Suen JH Yang CC 2362396920061683598810.1016/S 1726-4901(09)70226-6 · doi ↗ · pubmed ↗
- 5Robboy's Pathology of the Female Reproductive Tract Mutter GL Robboy SJ Prat J Bentley RC Russell P Anderson MC Amsterdam, Netherlands Elsevier 2008 https://shop.elsevier.com/books/robboys-pathology-of-the-female-reproductive-tract/mutter/978-0-443-07477-6
- 6Fibromatosis and massive edema of the ovary, possibly related entities: a report of 14 cases of fibromatosis and 11 cases of massive edema Int J Gynecol Pathol Young RH Scully RE 15317831984649031310.1097/00004347-198402000-00005 · doi ↗ · pubmed ↗
- 7A clinical update on massive ovarian oedema - a pseudotumour?Ecancermedicalscience Praveen R Pallavi V Rajashekar K Usha A Umadevi K Bafna U 31872013 https://doi.org/10.3332/ecancer.2013.3182371733910.3332/ecancer.2013.318PMC 3660160 · doi ↗ · pubmed ↗