An Overlooked Case of Abdominal Pain and Bowel Dysfunction: Chilaiditi Syndrome
William Adili, Corey Mumaw, Harthik Kambhampati, Carter R Olberding, Michael Herman

TL;DR
This paper describes a rare condition called Chilaiditi syndrome, where the colon sits between the liver and diaphragm, causing abdominal pain and bowel issues.
Contribution
The paper presents a case study highlighting the diagnostic challenges and conservative treatment of Chilaiditi syndrome.
Findings
Chilaiditi syndrome can be managed with conservative measures like dietary changes and fiber supplementation.
Imaging studies are crucial for diagnosing Chilaiditi syndrome and avoiding unnecessary procedures.
The condition is often misdiagnosed due to nonspecific gastrointestinal symptoms.
Abstract
Chilaiditi syndrome is an uncommon and often misdiagnosed condition characterized by the interposition of the colon between the liver and diaphragm, leading to symptoms of abdominal pain, bloating, and bowel dysfunction. Risk factors include chronic constipation, anatomical variations, and diaphragmatic dysfunction. This report presents the case of a 67-year-old male with right upper quadrant discomfort exacerbated by stool retention. Imaging studies ruled out acute pathology for critical conditions but demonstrated colonic interposition suggestive of Chilaiditi syndrome. Management provided consisted of conservative measures including dietary modifications and fiber supplementation, alleviating his symptoms without necessitating invasive procedures. This report emphasizes the importance of recognizing radiographic findings and risk factors of Chilaiditi syndrome in patients with…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
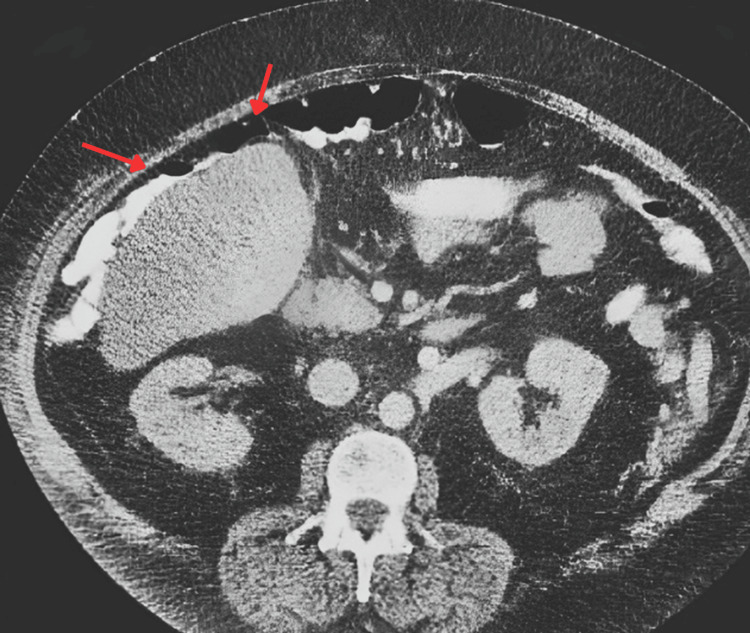 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsIntestinal Malrotation and Obstruction Disorders · Genetic Syndromes and Imprinting · Gastrointestinal disorders and treatments
Introduction
Chilaiditi sign is a rare radiologic finding of segmental interposition of the intestine between the liver and diaphragm [1]. Chilaiditi sign carries a worldwide incidence of 0.025-0.28% on plain radiographs and 1.1-2.4% on computed tomography (CT) scans [1,2]. This finding is observed significantly more in men than women, with a 4:1 male-to-female predominance [3]. When this finding is accompanied by gastrointestinal symptoms such as abdominal discomfort, bloating, nausea, or constipation, it is termed Chilaiditi syndrome [4]. While generally benign, Chilaiditi syndrome can mimic serious conditions, including pneumoperitoneum, hepatic pathology, or diaphragmatic hernia, potentially leading to unwarranted procedures [5]. Most cases of Chilaiditi syndrome can often be managed conservatively, and surgical intervention is rarely required when correctly identified. This report highlights the case of a 67-year-old male with suspected Chilaiditi syndrome, emphasizing the importance of considering this condition in the differential diagnosis of individuals with persistent upper abdominal pain.
Case presentation
A 67-year-old male presented to the clinic complaining of right upper quadrant abdominal pain, fullness, and persistent abdominal discomfort for several weeks. He reported that his symptoms worsened postprandially, but he denied symptoms of nausea, vomiting, weight loss, or bloody stools. Additionally, he reported a bloating sensation and occasional constipation, which he attributed to his overall level of discomfort.
Physical examination revealed mild tenderness in the right upper quadrant without guarding or rebound tenderness. Bowel sounds were normoactive, and no palpable mass was detected. Laboratory results, including liver function tests and inflammatory markers, were within normal limits. A right upper quadrant gallbladder ultrasound was performed, and no abnormalities were observed.
CT imaging of the abdomen revealed colonic interposition between the liver and diaphragm, raising suspicion for Chilaiditi syndrome (Figure 1). Additional findings included colonic distention with stool impaction in the right colon without evidence of hepatic steatosis, free air, or significant pathology.
Computed tomography (CT) displaying the left colon interposition between the liver and the left diaphragm (indicated by the arrows).
Discussion
Chilaiditi sign is often an incidental radiologic finding. However, when associated with gastrointestinal symptoms such as abdominal discomfort, bloating, and altered bowel habits, it is classified as Chilaiditi syndrome. This condition is particularly relevant in elderly patients with chronic constipation, as colonic distention and stool retention can exacerbate symptoms [6]. The reported incidence of Chilaiditi sign varies, with a greater incidence detected on CT scans (1.1-2.4%) compared to plain radiographs (0.025-0.28%), highlighting the importance of advanced imaging in its identification [2].
The pathophysiology of Chilaiditi syndrome is often multifactorial, involving anatomic variations and physiological factors. Under normal circumstances, the colon is secured by suspensory ligaments and other anatomical attachments, preventing displacement between the liver and diaphragm; however, anatomical variations, including the absence, laxity, or elongation of suspensory ligaments, can predispose to this condition [2]. Additional risk factors for Chilaiditi syndrome include chronic constipation, paralysis of the right hemidiaphragm, obesity, ascites, and cirrhosis [7]. Notably, the incidence of Chilaiditi syndrome is also higher among psychiatric inpatients, particularly those with schizophrenia, suggesting a wide range of risk factors that are not yet fully understood [8]. In this patient, chronic constipation, stool retention in the right colon, and advanced age were likely key contributors to the development and exacerbation of symptoms.
Management of Chilaiditi syndrome is generally conservative, focusing on symptom relief. This includes dietary modifications, stool softeners, and increased fiber intake to reduce colonic distention and improve bowel motility in those with constipation. Dietary recommendations include eating smaller, more frequent meals to prevent gastrointestinal overdistension, drinking at least eight glasses of water per day to promote bowel hydration and bowel motility, and limiting gas-producing foods such as legumes, carbonated beverages, and cruciferous vegetables to reduce bloating and discomfort. Surgical intervention is rarely necessary and is typically reserved for cases complicated by volvulus, ischemia, or bowel obstruction.
Recognizing Chilaiditi syndrome in patients with nonspecific gastrointestinal complaints is critical for preventing unnecessary interventions. Although a benign radiographic finding, misinterpretation of imaging findings for suspected free air under the diaphragm increases the likelihood of unwarranted exploratory surgeries, exposing patients to potential surgical complications and prolonged hospital stays. Furthermore, distinguishing Chilaiditi syndrome from other pathological conditions such as pneumoperitoneum, volvulus, or diaphragmatic hernia creates a more accurate and efficient diagnostic approach for clinicians. This increased recognition can lead to timely and appropriate management, reducing the likelihood of invasive procedures while ensuring appropriate patient care.
Conclusions
Chilaiditi syndrome remains an underrecognized yet important differential diagnosis for persistent abdominal pain and bowel dysfunction, particularly in elderly patients. As demonstrated in this case, chronic constipation and stool impaction can contribute to symptomatic exacerbation, best managed through dietary modifications, fiber supplementation, and bowel regulation.
Clinicians should maintain a high index of suspicion when evaluating patients with unexplained upper abdominal pain, especially if imaging reveals colonic interposition between the liver and diaphragm. Recognizing the benign nature of this condition is crucial to avoiding unnecessary interventions and ensuring effective, noninvasive management strategies to improve patient outcomes.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Colonic interposition between the liver and left diaphragm - management of Chilaiditi syndrome: A case report and literature review Oncol Lett Weng WH Liu DR Feng CC Que RS 16571660720142476519510.3892/ol.2014.1903 PMC 3997735 · doi ↗ · pubmed ↗
- 2Eventeration of diaphragm with Chilaiditi sign - A rare occurrence Respir Med Case Rep Sharan Kumar V 1014573420213440131310.1016/j.rmcr.2021.101457 PMC 8358153 · doi ↗ · pubmed ↗
- 3Chilaiditi syndrome precipitated by colonoscopy: A case report and review of the literature Hawaii J Med Public Health Yin AX Park GH Garnett GM Balfour JF 158162712012 https://pmc.ncbi.nlm.nih.gov/articles/PMC 3372788/22787564 PMC 3372788 · pubmed ↗
- 4Colonic interposition between the liver and diaphragm: "The Chilaiditi Sign"Can J Gastroenterol Hepatol Nair N Takieddine Z Tariq H 2174704201620162744682910.1155/2016/2174704 PMC 4904707 · doi ↗ · pubmed ↗
- 5Chilaiditi syndrome Stat Pearls [Internet] Kumar A Mehta D Treasure Island, FL Stat Pearls Publishing 2023 https://www.ncbi.nlm.nih.gov/books/NBK 554565/32119452 · pubmed ↗
- 6A case report of Chilaiditi syndrome presenting with a small bowel obstruction in an elderly Ethiopian man: A potential case for a misdiagnosis Int J Surg Case Rep Tola GG Tesso BA Kebede ML Bezabih YD 11053212520243954178410.1016/j.ijscr.2024.110532 PMC 11609392 · doi ↗ · pubmed ↗
- 7Image of the month. Chilaiditi sign or syndrome Arch Surg Alva S Shetty-Alva N Longo WE 939414320081820915910.1001/archsurg.2007.12-a · doi ↗ · pubmed ↗
- 8Chilaiditi syndrome--associated schizophrenia: 3 case reports J Clin Psychiatry Miyaoka T Seno H Itoga M Ohshiro R Inagaki T Horiguchi J Tachibana H 585962200110.4088/jcp.v 62n 0112 d 11235932 · doi ↗ · pubmed ↗