Does frailty modulate the predictive value of performance status in older adults living with cancer?
Daniela Patino-Hernández, Mario Ulises Pérez-Zepeda, Natalia Sánchez-Garrido, Alejandro Eliú Cedillo, Eduardo Cárdenas-Cárdenas

TL;DR
This study explores whether frailty affects how well performance status predicts mortality in older cancer patients.
Contribution
The study introduces frailty as a potential modifier of performance status in predicting outcomes for older cancer patients.
Findings
Frailty significantly influences mortality risk in older cancer patients.
Age is a significant risk factor for mortality in frail patients but not in those with low frailty.
Frailty evaluation can improve prognostic accuracy in older cancer patients.
Abstract
Cancer treatments are not a one-size-fits-all approach, treatment options are rarely studied in aging individuals, leading to worse outcomes related to increased vulnerability in this group of patients. Since frailty has shown the ability to modify outcomes, our study aims to assess if frailty modifies the association between performance status and days in bed with mortality risk in older adults with cancer. Our study is a secondary analysis of the Mexican Health and Aging Study, a cohort with a representative sample of individuals aged 50 years or older, with a baseline assessment in 2001 and follow-up data available for the years 2003, 2012, 2015, 2018 and 2021. We extracted the baseline variables from the main questionnaires, and the next-of-kin questionnaires were employed for information regarding mortality. We used Cox regression and Kaplan–Meier curves for survival analysis.…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
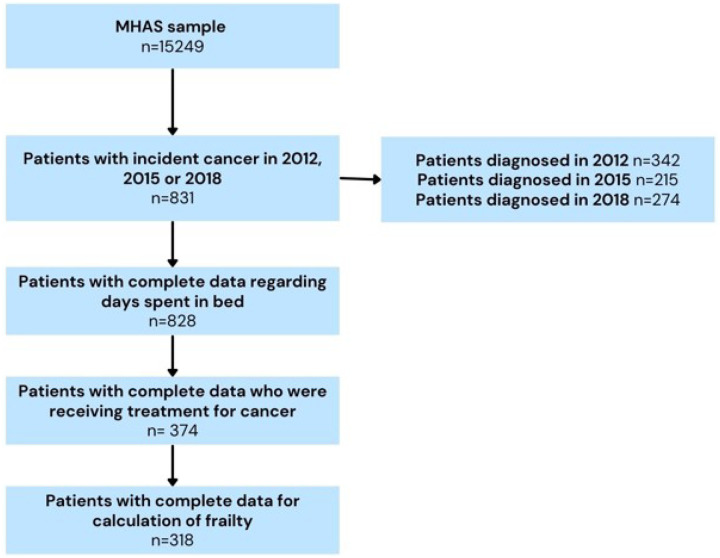 Figure 1
Figure 1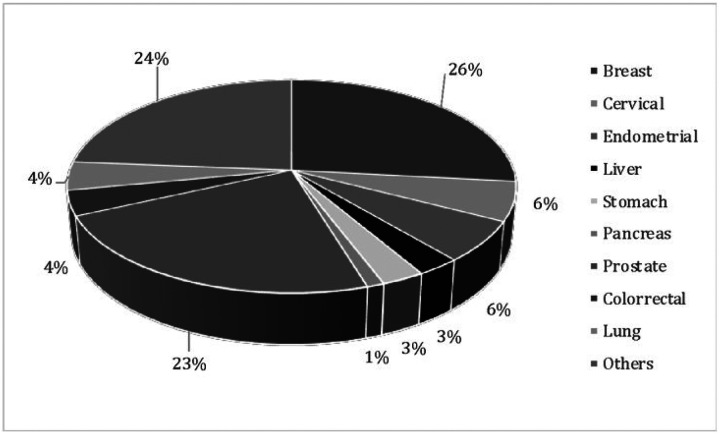 Figure 2
Figure 2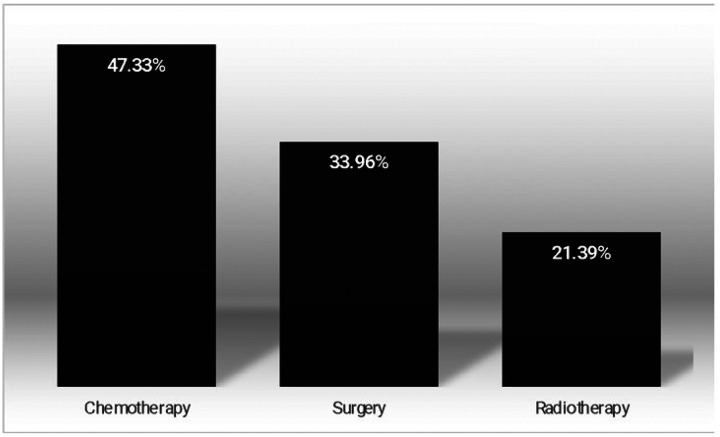 Figure 3
Figure 3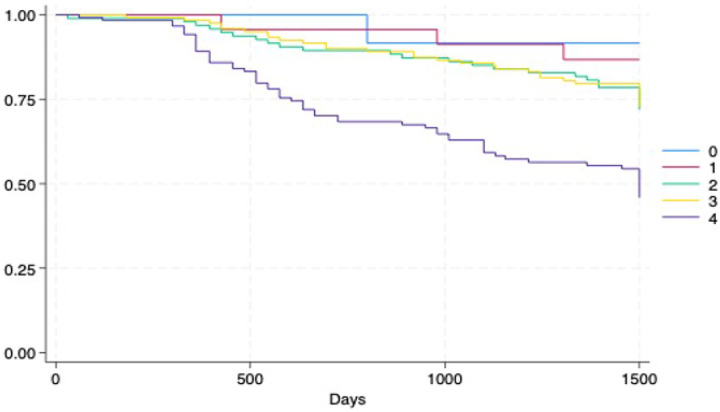 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsFrailty in Older Adults · Health Systems, Economic Evaluations, Quality of Life · Nutrition and Health in Aging
Introduction
Cancer treatments are not a one-size-fits-all approach, and even when age is a well-known risk factor for developing malignant neoplasms, course and treatment options are scarcely studied in aging individuals, leading in many cases to worse outcomes, due to increased vulnerability of these individuals [1]. Frequently impaired functional and cognitive status, increase the risk for treatment-related toxicity, leading to a decline of overall health or even death [2]. For example, social vulnerability; understood as the degree to which susceptibility to health problems may be modulated by the complexity of a particular social situations (e.g., family members, friends, community engagement, financial income, etc.), has shown to be a relevant factor into health outcomes of older adults [3, 4]. Moreover, socioeconomic and cultural factors have important roles in these outcomes of older adults suffering from cancer [5].
On the other hand, frailty —the age-related phenomenon of increased susceptibility to common stressors — is associated with multiple adverse outcomes across common conditions of the older adults [6, 7]. On the other hand, evidence has shown that this condition can shape the prognosis of individuals (e.g., diseases, treatments, emotional crises), particularly those diagnosed with cancer [8, 9]; challenging the results of many tools adopted to predict adverse outcomes in younger individuals.
Regarding cancer prognosis, functional status has been evidenced as having a better prognostic value in oncology than other parameters–such as age–accurately establishing prognosis, tolerance, quality of life and treatment response [10, 11]. Indeed, two of the most used instruments for assessing performance status in oncological practice include the Eastern Cooperative Oncology Group (ECOG) and the Karnofsky scale [12], both of which include functional performance assessment. However, these instruments have been criticized for being highly subjective and not being able to detect real-time changes of potential clinical relevance (e.g., low prognostic value for older adults) [11, 13]. Additionally, these evaluations were not initially intended to assess older adults and might not have the same clinimetric properties as in younger individuals [14], leading to undertreatment if functional status were to be underestimated.
Therefore, we hypothesize that different frailty levels affect the associations of a measurement that includes days in bed and physical functioning with mortality, independent of other variables, such as social vulnerability. Our study aims to assess if frailty modifies the association of performance status and days in bed with mortality risk in older adults with cancer.
Methods
Design and Sample
2.1
This is a secondary analysis of the Mexican Health and Aging Study (MHAS), a cohort with a national-level representative sample from Mexican individuals aged 50-years or older. In brief, this study aims to determine the factors that impact aging in Mexican individuals and consists of several waves, with a baseline assessment in 2001; follow-up data are available for the years 2003, 2012, 2015, 2018 and 2021; information from a wide array of topics was obtained from face–to–face interviews conducted by trained personnel. Further details about MHAS can be found elsewhere [15–17].
For this work, we used data from MHAS assessments from 2012, 2015 and 2018 and follow-up information on survival status through 2021. We extracted the baseline variables from the main questionnaires, and the next-of-kin (NOK) questionnaires were used for information regarding mortality. All individuals ≥ 50 years old who answered directly to the baseline interview and with complete data (both baseline and follow-up) were included (Fig. 1).
Variables
2.2
Cancer status
2.2.1
Subjects who reported having cancer were identified by asking the following question: ‘Has a doctor or medical personnel ever diagnosed you with cancer?’ If the individual answered ‘yes’ a follow-up question regarding the type of cancer was asked (including breast, cervix, endometrial/uterine, liver, stomach, pancreas, prostate, colorectal, and lung) (see Fig. 2). Our sample was composed only of ‘incident’ cases, meaning that they had not previously been diagnosed with cancer and did not refer having cancer in previous waves. We further restricted our sample to include only subjects who reported being treated currently in any of the subsequent follow-up interviews. These two criteria (new cancer and currently receiving treatment) were introduced to maximize the approximation to ‘real-world’ and actual clinical practice. Finally, the type of cancer and treatment (surgery, radiotherapy or chemotherapy) were included for descriptive purposes.
Performance status, physical activity and days in bed assessment
2.2.2
The Eastern Cooperative Oncology Group (ECOG) scale is based on the time spent in bed, with 0 representing full functionality for asymptomatic patients and 4 being bedridden [13]. Since MHAS does not include measurements to assess cancer prognosis due to its general scope of aging, the performance status was constructed with available variables in the study measuring days in bed, physical function and exercise. Firstly, number of days spent in bed per year was obtained through the following question: ‘Owing to sickness or injury, during the last 12 months, how many days did you stay in bed for at least half the day?’ [18]. Secondly, physical activity was assessed by answering yes or no to the following question: ‘On average, during the previous two years, have you exercised or had done vigorous physical activity three times a week or more? ´ Finally, basic and instrumental activities of daily living were included, as follows: the MHAS includes a set of 19 of these activities (please see supplementary material); whenever an older adult answered that they were not able to perform an activity, a score of 1 was assigned; if no difficulty was present, the score was 0; and if help was required to perform the activity, a score of 0.5 was assigned. The scores were summed, resulting in a score of 0 (no difficulties in activities of daily living) or up to 19, the highest possible score (impossibility of performing all the assessed activities). More detail can be found in supplementary Table 1.
We then categorized the performance status score into 5 categories: 0 (< 50% of days spent in bed during the previous year, no disability and reported physical activity), 1 (< 50% of days spent in bed during the previous year, no disability and no report of physical activity), 2 (< 50% of days spent in bed during the previous year, disability and no report of physical activity), 3 (> 50% of days spent in bed during the previous year, no disability and no report of physical activity), and 4 (> 50% of days spent in bed during the previous year, disability and no report of physical activity).
Mortality
2.2.3
All-cause mortality was our outcome of interest, including time to event, for survival analysis. For those who survived, follow-up days were calculated as the difference between the interview date in 2001 and that from 2021; in a similar fashion, time to event was calculated as the difference in days from the baseline interview to the reported date of death.
Frailty index
2.2.4
The frailty index (FI) was calculated from 33 variables related to self-reported health, comorbidities, depressive symptoms and other symptoms [19]. The FI is a synthetic measurement grounded on the deficit accumulation theory, that has been used and validated in MHAS [20]. A modified version of the original 52-item FI used in MHAS was used, since variables previously used, for purposes of this work had to be excluded since they were incorporated into the previously described tool for cancer prognosis (see above). Characteristics of the index, such as: prevalence of the deficits, coding and definition from MHAS are available in supplementary Table 2.
Sociodemographic characteristics
2.2.5
We included the following variables: age in years and sex, marital status (married/civil union versus without a couple), and the number of completed years of formal education.
Social vulnerability index
2.2.6
This variable was created by combining various items suggestive of living conditions for everyone, including marital status, support provided by friends and family, social activities and hobbies, among others [21, 22]. The social vulnerability index (SVI) was created using the methods described [23] and has been previously used in MHAS [3]. A more detailed description can be found in Supplementary Table 3.
Lifestyle
2.2.7
Smoking status was assessed based on the following questions: ‘Have you smoked more than 100 cigarettes or 5 packs in your lifetime; not including pipes or cigars?’ and ‘Do you smoke cigarettes now?’, resulting in three categories: never smoked, used to smoke and current smoking. Physical activity was defined as exercising ≥ 3 times a week in the previous year. Finally, risky alcohol use was defined as exercising ≥ 2 drinks per day for women and ≥ 3 drinks per day for men [24].
Statistical analysis
2.3
We conducted a descriptive analysis of all the variables and bivariate analyses by survival status for baseline characteristics, using chi-square tests for all the variables (except for FI and SVI, where t tests were used). Descriptive statistics were used to report these findings.
In addition, Kaplan–Meier curves were plotted to assess the differences between performance status groups and other cancer-related variables; log-rank tests were used for statistical significance. Cox regression models were fitted to test the associations with mortality with hazard ratios (HR). Interaction terms between FI and performance status variables were included for the whole sample and were unadjusted and adjusted for baseline characteristics. All the statistical analyses were performed with the statistical software StataNow 18.5 (Stata Corp LLC, 4905 Lakeway Dr; College Station, TX, USA).
Results
Descriptive statistics
3.1
Our sample was composed of 318 individuals (Figure 1), with a mean age of 68.02 years (SD 10.78), and most were women (62.57%). The main types of cancer found in our sample were breast cancer (26%), cervical cancer (24%) and endometrial cancer (23%) (see Figure 2). Chemotherapy was the most common treatment (47.33%), surgery was part of the treatment for 33.96% of the sample, and radiotherapy was the least used reported treatment for 21.39% of the studied individuals (see Figure 3).
Overall, 22.64% of the sample were physically active. With respect to smoking status, approximately one-third of the sample were former smokers (30.48%), and 9.09% were active smokers. Risky alcohol was present in 8.56% of the individuals. No statistically significant differences were found for age, sex, alcohol or cigarette consumption or physical activity among individuals who were alive and those who were deceased at follow-up. However, those who died had higher means for the frailty index, social vulnerability status, days in bed and performance status scores (see Table 1).
Kaplan–Meier survival estimates
3.2
The Kaplan–Meier curves further revealed greater survival in patients with better performance status (lower scores) – (0.81% mortality with performance status category 0) - which decreased with increasing scores (worse performance status). – (49.6% mortality with performance status category 4) (see Figure 4). However, the group with higher mortality was the one categorized as 4, a statistically significant difference (p<0.001).
Cox regression models
Cox regression revealed that for low frailty levels, the social vulnerability index (HR 234.79; 95% CI 4.51–12222.8; p=0.007) and performance status 2 (HR 5.46; 95% CI 1.24–24.04; p=0.025) were significantly associated with increased risk of mortality, whereas age, sex, smoking status, and alcohol intake did not affect mortality risk. In contrast, among individuals with high frailty levels, age (HR 1.04; 95% CI 1.00–1.07; p=0.039) was the only significant predictor of increased risk.
Additionally, when the performance status score was analyzed, a score of 4 clearly increased mortality 8-fold, but this association was lost in those with high frailty levels (see Table 2).
Discussion
According to our results, older adults suffering from cancer and low frailty levels, the composite tool for performance status was associated with higher mortality rates, the higher the composite tool score category was. In fact, previous reports have consistently demonstrated this association across different types of cancer [25–27]. However, our results showed that in individuals with high frailty levels, this composite tool was not associated with mortality. Interestingly, other variables such as the SVI also lost their significant association for mortality.
Older adults with cancer are at greater risk for mortality, treatment-related complications, hospitalizations and admissions to long-term care facilities [1]. Unlike younger patients, whose treatment decisions are typically based on outcomes such as survival and progression-free survival, for older adults, treatment goals should also include minimizing toxicity, maximizing quality of life and maintaining functional independence [28]. This broader focus has recently led to updates in guidelines from the American Society of Clinical Oncology (ASCO) and the Society of Geriatric Oncology (SGO), recommending the inclusion of comprehensive assessments of age-associated vulnerabilities in older patients receiving systemic cancer therapies [29–31].
For example, two randomized clinical trials published recently, the Geriatric Assessment for Patients 70 years and Older (GAP70+) and the Geriatric Assessment-Driven Intervention (GAIN), demonstrated the impact of an integral geriatric assessment (IGA) on reducing the risk of toxicity and improving clinical outcomes in older adults. By identifying vulnerabilities (i.e., frailty) and tailoring treatment plans accordingly, these studies have shown that IGA can help mitigate treatment-related risks and improve overall patient well-being [2, 32].
However, while cost-effective and highly useful, the implementation of this assessment may be limited by resource and geriatricians’ availability across different settings [33]. Furthermore, our findings suggest that older adults suffering from high levels of frailty, physical performance—typically a cornerstone of cancer prognosis—is less predictive of mortality. This may be due to under recognition of frailty in settings where ECOG scores–or other similar tools–can be influenced by subjective assessments of a patient’s functional status. For example, it has been reported that older adults often receive worst ECOG scores despite having similar levels of physical activity as younger individuals [14]. This underestimation of functional status can lead to undertreatment. On the other hand, ECOG scores may be overestimated in older adults who are deemed “normal for their age,” potentially masking manageable conditions.
Moreover, recent studies suggest that clinicians have a limited ability to predict toxicity based on performance status alone, further emphasizing the need for additional evaluation for older adults suffering from cancer [34]. Our results also highlight the relevance of social vulnerability in predicting outcomes for older cancer patients, even when frailty is not present. On this matter, a study by Stuart et al. revealed that high social vulnerability scores were associated with patients presenting with advanced stages of cancer which lead to lower rates of surgery or chemotherapy, increasing the odds of dying due to these delays and incorrect decisions [35].
We recognize that our study has several limitations. This is a secondary analysis of already available data; the latter implies that we created our variables based on information that had been collected in a standardized fashion but that were not collected specifically for our research question. Furthermore, different ways of assessing frailty exist; if a different approach is used, the results may differ. However, our study also has various strengths to consider. For example, this is a representative cohort of individuals followed for 20 years. This allows our conclusions to represent not only a large population but also a significant period, indicating that despite changes in available therapies, frailty continues to modulate the predictive ability of prognostic scores in older adults with cancer. Furthermore, lifestyle factors such as risky alcohol intake and smoking, as well as social vulnerability risk, which are known to be linked to worse outcomes, were considered covariates, which allows conclusions to be of greater strength.
Conclusion
Our results highlight the importance of frailty as a key element in treatment decision-making and outcomes in older cancer patients. While performance status remains a valuable tool, its predictive value diminishes when frailty is present. The latter reflects the complexity of assessing prognosis in older adults with cancer, where factors such as frailty may overshadow other clinical markers, making a geriatric assessment a cornerstone of rational treatment in this group of patients.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Soo WK, King MT, Pope A, Parente P, Darzins P, Davis ID. Integrated Geriatric Assessment and Treatment Effectiveness (INTEGERATE) in older people with cancer starting systemic anticancer treatment in Australia: a multicentre, open-label, randomised controlled trial. Lancet Healthy Longev. 2022 Sep;3(9):e 617–e 27.36102776 10.1016/S 2666-7568(22)00169-6 · doi ↗ · pubmed ↗
- 2Mohile SG, Mohamed MR, Xu H, Culakova E, Loh KP, Magnuson A, Evaluation of geriatric assessment and management on the toxic effects of cancer treatment (GAP 70+): a clusterrandomised study. Lancet. 2021 Nov 20;398(10314):1894–904.34741815 10.1016/S 0140-6736(21)01789-XPMC 8647163 · doi ↗ · pubmed ↗
- 3Sánchez-Garrido N, Aguilar-Navarro SG, Ávila-Funes JA, Theou O, Andrew M, Pérez-Zepeda MU. The Social Vulnerability Index, Mortality and Disability in Mexican Middle-Aged and Older Adults. Geriatrics (Basel). 2021 Mar;6(1).10.3390/geriatrics 6010024 PMC 800604633800197 · doi ↗ · pubmed ↗
- 4Andrew MK, Mitnitski AB, Rockwood K. Social vulnerability, frailty and mortality in elderly people. P Lo S One. 2008 May 21;3(5):e 2232.18493324 10.1371/journal.pone.0002232 PMC 2375054 · doi ↗ · pubmed ↗
- 5Fowler ME, Harmon C, Tucker A, Sharafeldin N, Oates G, Baker E, The association between social vulnerability and geriatric assessment impairments among older adults with gastrointestinal cancers-The CARE Registry. Cancer. 2024 Sep 15;130(18):3188–97.38824657 10.1002/cncr.35390 PMC 12021024 · doi ↗ · pubmed ↗
- 6Rockwood K. Frailty and aging medicine. Aging Med (Milton). 2019 Mar;2(1):4–6.31942506 10.1002/agm 2.12060 PMC 6880699 · doi ↗ · pubmed ↗
- 7Rockwood K, Howlett SE. Fifteen years of progress in understanding frailty and health in aging. BMC Med. 2018 Nov 27;16(1):220.30477486 10.1186/s 12916-018-1223-3PMC 6258409 · doi ↗ · pubmed ↗
- 8Skelly A, O’Donovan A. Recognizing Frailty in Radiation Oncology Clinical Practice: Current Evidence and Future Directions. Semin Radiat Oncol. 2022 Apr;32(2):115–24.35307113 10.1016/j.semradonc.2021.11.010 · doi ↗ · pubmed ↗