4D flow yields similar clinical results compared to 2D phase contrast for decision making regarding pulmonary valve replacement in repaired tetralogy of Fallot
Alison Almgren-Bell, Andrada Popescu, Aparna Sodhi, Michael Markl, Cynthia Rigsby, Joshua Robinson

TL;DR
This study compares 4D flow MRI to traditional 2D MRI for measuring pulmonary regurgitation in patients with repaired tetralogy of Fallot and finds similar clinical outcomes for valve replacement decisions.
Contribution
The study demonstrates that 4D flow MRI can yield comparable clinical decisions to 2D phase contrast MRI for pulmonary valve replacement in repaired tetralogy of Fallot patients.
Findings
PRF correlated strongly between 2D PC and 4D flow (r=0.83).
The mean absolute difference between 2D and 4D PRF was −3.4% (± 9.3%).
4D flow generates accurate PRF measurements and similar clinical decisions for PVR in rTOF.
Abstract
2D CMR is critical for monitoring PR fraction (PRF) and biventricular size in patients with a history of repaired tetralogy of Fallot and guides decisions about pulmonary valve replacement (PVR). However, its clinical utility is limited, increasing enthusiasm for newer techniques such as 3D time-resolved phase contrast (4D flow) MRI. We investigated whether using 4D flow to calculate PRF would yield similar clinical decisions about PVR in rTOF compared to conventional 2D CMR. All patients with rTOF who underwent standard CMR plus retrospectively gated 4D flow between February 2021 – June 2023 were identified. Clinical information was collected from the EMR. 2D cine SSFP, phase contrast (PC) data, and 4D flow imaging data were analyzed using standard post-processing analysis. Clinical decisions (“intervention vs. no intervention”) were determined using a standardized algorithm, and…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
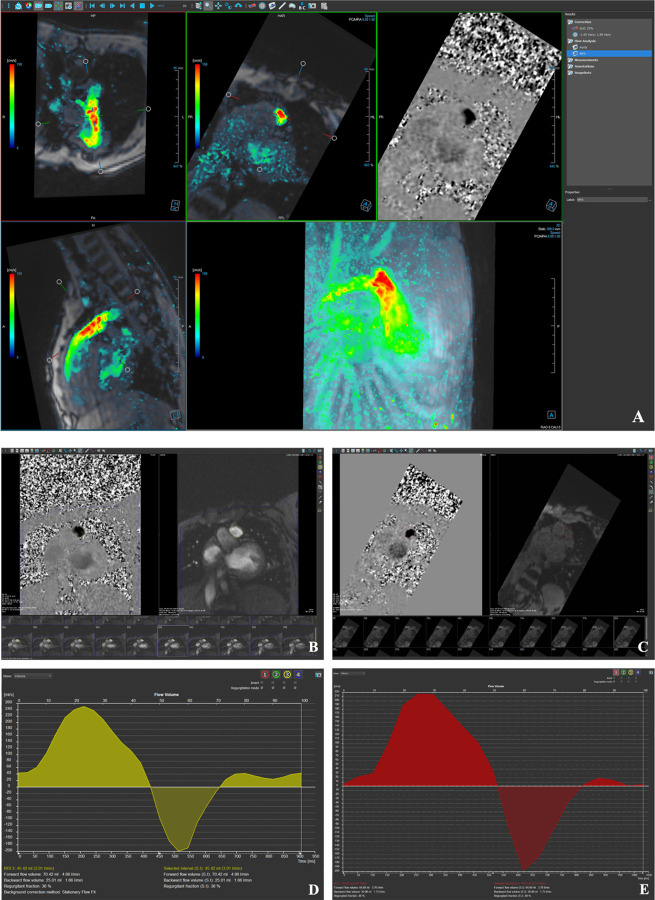 Figure 1
Figure 1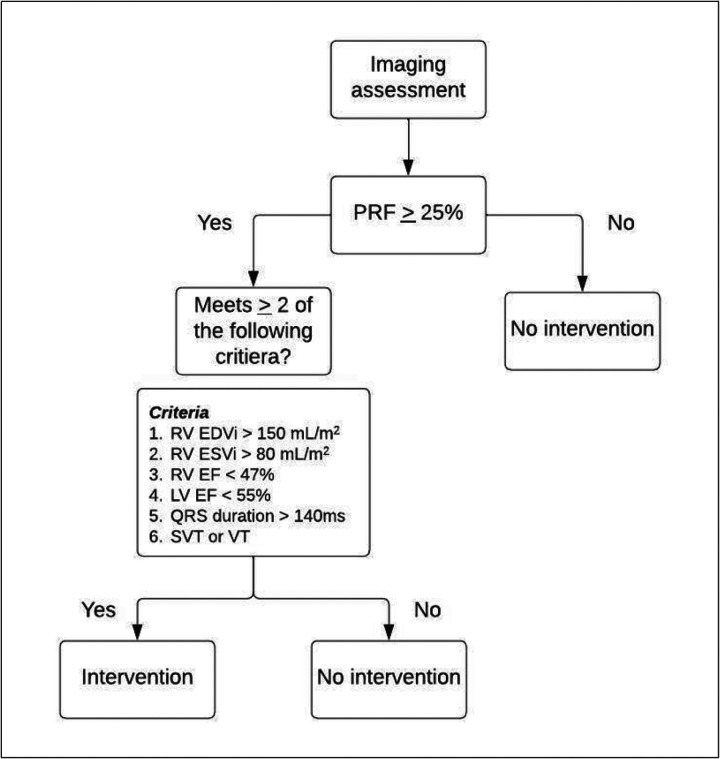 Figure 2
Figure 2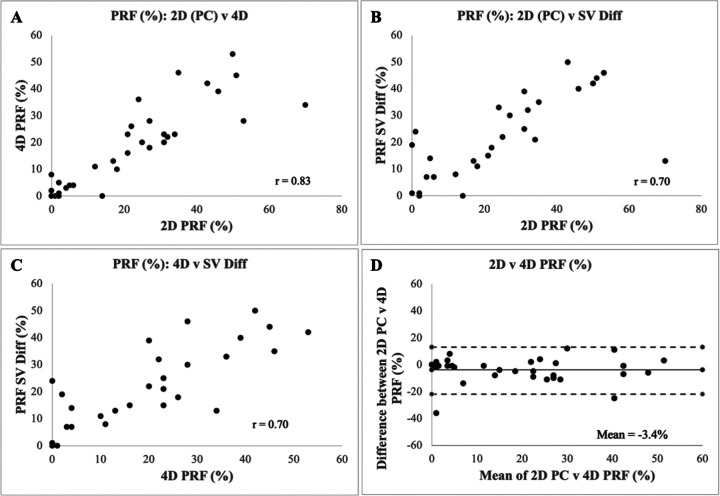 Figure 3
Figure 3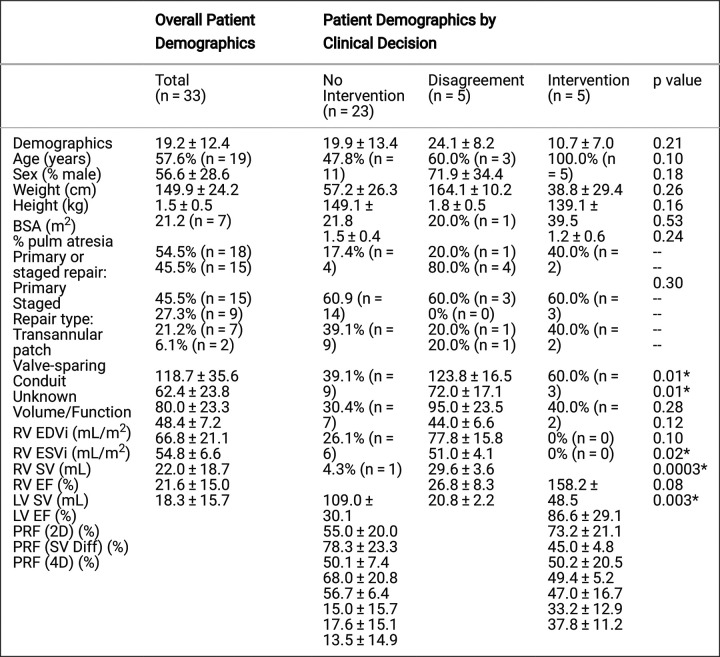 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCongenital Heart Disease Studies · Aortic Disease and Treatment Approaches · Vascular anomalies and interventions
INTRODUCTION
Tetralogy of Fallot (TOF) is the most common cyanotic congenital heart defect (CHD) with an estimated prevalence of 4.6/10,000 new cases per year [1–3]. While surgical outcomes and long-term prognosis have improved significantly, residual anatomic and hemodynamic abnormalities are common [3–6]. Chronic pulmonary regurgitation (PR) is a common hemodynamic complication following initial repair of TOF and frequently leads to right ventricular (RV) dilation and dysfunction with increased risk for exercise intolerance, right heart failure, arrhythmias, and sudden death [3, 7–10] Pulmonary valve replacement (PVR) reduces PR, decreases RV overload, and normalizes RV volumes [4, 11]. However, the hemodynamic benefits of PVR must be balanced with the risks of premature invention and surgical complications including valve failure and death [4]. These considerations are in uenced by growing transcatheter PVR options such that optimal timing of PVR remains highly debated. The decision to pursue intervention involves careful consideration of natural history and pathophysiology as well as procedural risks and benefits [4, 7, 11, 12].
2D cardiac magnetic resonance (CMR) is currently the gold standard for monitoring PR, ventricular function, and ventricular volumes in patients with repaired TOF (rTOF) [4, 13, 14]. However, long scan times (often >60 minutes) and breath-holding requirements present challenges to clinical work flow and widespread usage, especially in younger patients and those with developmental delay [10, 13, 15]. 3D time-resolved phase contrast (4D flow) CMR is a novel technique that allows magnitude and phase contrast (PC) data to be obtained from a single, free-breathing sequence [13, 16]. 4D flow scan time is an average of 5–15 minutes and thus may decrease the need for anesthesia in younger patients as well as patients with decompensated heart failure or developmental delay, making it a promising new technique for long-term monitoring of rTOF patients [5, 13, 16].
Several studies have shown that 4D flow performs similarly to 2D PC in measurements of blood flow and ventricular volume [13, 17, 18]. In one study of rTOF patients, 4D flow demonstrated greater accuracy compared to 2D PC for flow measurements and performed similarly to 2D SSFP for volumetric analysis [13]. While agreement between 2D and 4D flow is established, the implications of 4D flow on real-world PVR decision making have not been fully studied [13]. Moreover, the growing availability of commercial software applications has made 4D flow post-processing easier, less time consuming and more clinically feasible. This study is a retrospective comparison of clinical decision making in the management of rTOF with 2D PC CMR versus 4D flow to test the hypothesis that 4D flow provides accurate clinical information that yields similar clinical decisions.
MATERIALS AND METHODS
Study population
We retrospectively identified all patients with rTOF who underwent standard clinical CMR with cine SSFP and PC imaging between February 2021 and June 2023 at Lurie Children’s Hospital. The medical center IRB approved this study, and informed consent was waived for retrospective clinical data collection. Patients who had undergone prior PVR were included. Patients who did not have diagnostic quality CMR exams, who had important metallic artifact, and who did not have both 2D phase contrast and 4D flow imaging were excluded. Demographic data and clinical history were manually extracted from the electronic medical record and included patient age, sex, BSA, cardiac diagnoses and number of prior cardiac intervention(s), symptoms, and EKG results including QRS duration.
Image acquisition
Imaging was performed on a 1.5T scanner (MAGNETOM Aera; Siemens Healthineers, Erlangen, Germany) using an 18-channel matrix coil. Standard balanced steady-state free precession cine imaging and 2-D PC scans were obtained per routine clinical protocol and as appropriate for the assessment of patients with TOF [19]. If contrast was administered, 2D PC MRI and 4D flow were acquired following administration of either ferumoxytol (Feraheme, AMAG Pharmaceuticals, Waltham, MA) or gadobutrol (Gadavist, Bayer HealthCare, Whippany, NJ). 4D flow scan characteristics for this cohort were: spatial resolution = 1.4–4.5 × 1.1–3.1 × 1.4–3.5 mm^3^, temporal resolution = 36.0–44.8 ms, repetition time/echo time [TR/TE] = 4.7–5.1/2.2–3.0 ms, flip angle = 15°, and velocity sensitivity (VENC) = 100–250 cm/s. General anesthesia was administered by a pediatric anesthesiologist per the institutional clinical protocol for 9/33 patients (27%).
Image analysis
2D SSFP and PC data were obtained from the clinical CMR report completed by the cardiologist and radiologist. PRF by SV was calculated using the following equation: PRF = (SV_RV_ – SV_LV_) / SV_RV._ Qflow software (Medis Suite, Leiden) was used for 4D flow post processing (Figure 1). Background phase offset corrections were performed, and the phase unwrap tool was applied if there was velocity aliasing For 4D flow analysis, cross-sectional planes were oriented perpendicular to the direction of flow and vessel anatomy. Pulmonary flow was measured at the main pulmonary artery, and the 3D region of interest was manually drawn around the vessel lumen directly above the pulmonary valve. flow parameters such as net flow, forward flow, backward flow, and PRF were quantified and recorded.
PVR decision-making algorithm
Clinical decisions regarding PVR (“intervention vs. no intervention”) were determined using the conventional indications algorithm outlined in the flow chart Figure 2) [4]. Decisions were first made using the PRF calculated only by 2D PC or 4D flow. The same algorithm was then run again using PRF calculated by 2D PC or 4D flow in conjunction with PRF calculated via SV difference, similar to conventional clinical practice.
Statistical analysis
All continuous variables were reported as mean ± standard deviation, and categorical variables were reported as percentage and frequency. Bland-Altman analyses were used to assess agreement between different methods. Inter-rater agreement for the decision was measured using Cohen’s kappa coefficient.
RESULTS
Fifty patients met initial criteria during the defined study time period. Fifteen patients were excluded due to lack of 2D (n=6) or 4D (n=9) PC data, and two patients were excluded due to metallic artifact precluding PV assessment, resulting in a study population of 33 patients. Contrast was administered in 15/33 exams (45%). Patient demographics are shown in Table 1. Important differences among groups stratified by clinical decision include RV end-diastolic volume (EDV), RV end-systolic volume (ESV), LV ejection fraction (EF), and PRF measured by 2D PC and 4D flow. PRF calculated by 2D PC correlated strongly with 4D flow-derived PRF (r=0.83) (Figure 3). PRF showed moderate-strong correlation between 2D PC and SV difference (r=0.70) and between 4D flow and SV difference (r=0.70) (Figure 3).
Algorithm-based decisions for PVR are shown in Table 2. 28 decisions (85%) were concordant between 2D PC and 4D flow. Intervention was recommended in 23 of these cases, and no intervention was recommended in the other 5. There were five discordant decisions; in all five, 2D recommended intervention whereas 4D recommended no intervention. When using PRF calculated by 2D only and 4D only, the inter-rater agreement was moderate (κ = 0.58). When using PRF calculated by 2D with SV and 4D with SV, there were three discordiant decisions, in which 2D recommended intervention whereas 4D recommended no intervention. The inter-rater agreement improved and was strong (κ = 0.76).
DISCUSSION
In this study, we assessed the utility of 4D flow compared to 2D PC in real-world clinical decision-making regarding indication for PVR in the rTOF population. We also compared PRF measured by 4D flow, 2D PC, and SV difference and found strong correlations between PRF measured via all three methods. These findings are consistent with prior studies that similarly found robust agreement between flow measurements obtained via 2D PC and 4D flow [17, 18]. We also found that 4D flow and 2D PC resulted in similar clinical decisions about recommendation for PVR using a conventional algorithm. Using all available information (both flow and cine SSFP derived) resulted in nearly universal agreement. Based on these findings, 4D flow holds significant promise in the evaluation and management of patients with rTOF.
This study offers novel insight into the role of 4D flow in conventional decision-making for patients with rTOF. Despite several studies investigating ideal indications for intervention, the decision surrounding intervention remains highly nuanced and individualized with significant practice variation across centers and providers [20, 21]. Several studies have found that intervention in patients satisfying volumetric requirements leads to improvement in RV volume and function, yet the specific thresholds predictive of optimal outcome vary across studies [22–26]. Massarella et al examined referral patterns in a multicenter cohort of rTOF patients and found that majority of their cohort met criteria for PVR yet were not referred for intervention [20]. Further analysis of their cohort suggested that thresholds for referral proposed in guidelines are more aggressive than the thresholds used to guide decision-making in everyday clinical practice [20]. The small differences in agreement across clinical decisions found in our study fall well within the range of practice variation.
In addition to 4D flow’s strong clinical performance in determining the severity of PR and indication for PVR, this technique offers additional insights into higher order fluid dynamics and evolving hemodynamic efficiencies [5]. Physiological parameters derived from 4D flow like kinetic energy (KE), helix and vortex formation, energy loss, and wall shear stress have shown promise as early biomarkers in TOF [27–35]. RV KE has been shown to be higher in TOF patients compared to healthy controls and correlate with volumetric and flow markers of disease severity, including RV EDVi and PRF [27, 30–32]. Altered hemodynamic forces and flow patterns, including pathologic vortex formation, are seen in TOF patients and have been shown to correlate with RV dysfunction and exercise intolerance [28, 33–35].
In summary, the ability to capture conventional and novel hemodynamic parameters in under ten minutes with a single, free-breathing, scan combined with the recent advancements in commercially available post-processing software makes 4D flow an increasingly feasible and compelling addition to the current clinical workflow for management of patients with rTOF [36].
Limitations of this study include our small study cohort of patients with rTOF and retrospective study design. Another limitation of this study is the focus on agreement between 2D PC and 4D flow; future study of ventricular volume assessment by 4D flow or in combination with other accelerated techniques could lead to an even shorter, comprehensive exam for TOF patients.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Apitz C, Webb GD, Redington AN (2009) Tetralogy Fallot Lancet 374(9699):1462–147119683809 10.1016/S 0140-6736(09)60657-7 · doi ↗ · pubmed ↗
- 2Mai CT (2019) National population-based estimates for major birth defects, 2010–2014. Birth Defects Res 111(18):1420–143531580536 10.1002/bdr 2.1589 PMC 7203968 · doi ↗ · pubmed ↗
- 3Gatzoulis MA (2000) Risk factors for arrhythmia and sudden cardiac death late after repair of tetralogy of Fallot: a multicentre study. Lancet 356(9234):975–98111041398 10.1016/S 0140-6736(00)02714-8 · doi ↗ · pubmed ↗
- 4Geva T (2011) Repaired tetralogy of Fallot: the roles of cardiovascular magnetic resonance in evaluating pathophysiology and for pulmonary valve replacement decision support. J Cardiovasc Magn Reson 13(1):921251297 10.1186/1532-429X-13-9PMC 3036629 · doi ↗ · pubmed ↗
- 5Elsayed A (2021) Four-dimensional flow cardiovascular magnetic resonance in tetralogy of Fallot: a systematic review. J Cardiovasc Magn Reson 23(1):5934011372 10.1186/s 12968-021-00745-0PMC 8136126 · doi ↗ · pubmed ↗
- 6Nollert G (1997) Long-term survival in patients with repair of tetralogy of Fallot: 36-year follow-up of 490 survivors of the first year after surgical repair. J Am Coll Cardiol 30(5):1374–13839350942 10.1016/s 0735-1097(97)00318-5 · doi ↗ · pubmed ↗
- 7Flors L (2020) Preprocedural Imaging Evaluation of Pulmonary Valve Replacement After Repair of Tetralogy of Fallot: What the Radiologist Needs to Know. J Thorac Imaging 35(3):153–16632073541 10.1097/RTI.0000000000000478 · doi ↗ · pubmed ↗
- 8House AV (2019) Can Abbreviated Cardiac Magnetic Resonance Imaging Adequately Support Clinical Decision Making After Repair of Tetralogy of Fallot? Pediatr Cardiol 40(3):616–62230539240 10.1007/s 00246-018-2035-0 · doi ↗ · pubmed ↗