Cytomegalovirus-Induced Colitis Presenting as Acute Appendicitis in an Immunocompetent Patient With Ulcerative Colitis
Alessandro Pedicelli, Amine Zoughlami, Olga Aleynikova, Christina Greenaway, Corey Miller

TL;DR
A 71-year-old man with ulcerative colitis showed symptoms of acute appendicitis, but was diagnosed with cytomegalovirus (CMV) colitis through colonoscopy.
Contribution
This case highlights a rare presentation of CMV colitis mimicking acute appendicitis in an immunocompetent patient.
Findings
CMV colitis was diagnosed in a patient with ulcerative colitis despite an initial radiological diagnosis of acute appendicitis.
The patient was immunocompetent, which is unusual for CMV reactivation cases.
Colonoscopy was crucial for accurate diagnosis after antibiotic treatment failed.
Abstract
We report a rare case of cytomegalovirus (CMV) colitis presenting radiologically as acute appendicitis in an immunocompetent 71-year-old man known for ulcerative colitis. Although initial imaging revealed acute appendicitis, a lack of clinical improvement with antibiotic therapy prompted further evaluation with colonoscopy, which led to the diagnosis of CMV colitis on a background of mild ulcerative colitis flare. Most individuals infected by CMV will exhibit lifelong latency; however, the virus can reactivate under impaired immune status (eg, transplant recipients, those receiving immunosuppressive therapy). Patients with underlying inflammatory bowel disease are especially at risk of CMV colitis during an acute flare. This case illustrates a unique presentation of CMV colitis in an immunocompetent host, with initial imaging studies revealing acute appendicitis.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1 Figure 2
Figure 2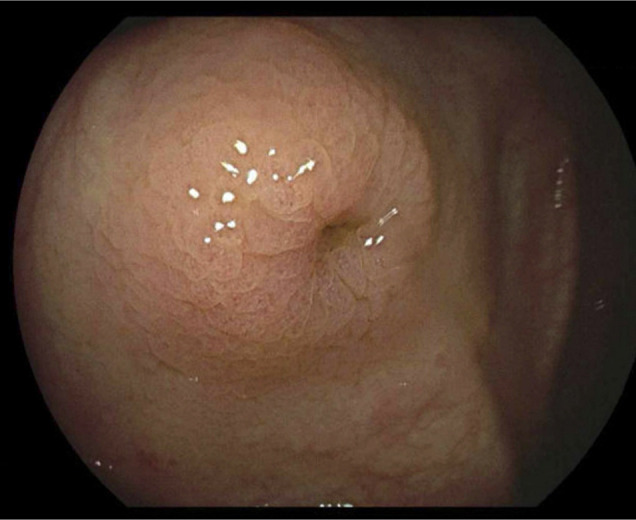 Figure 3
Figure 3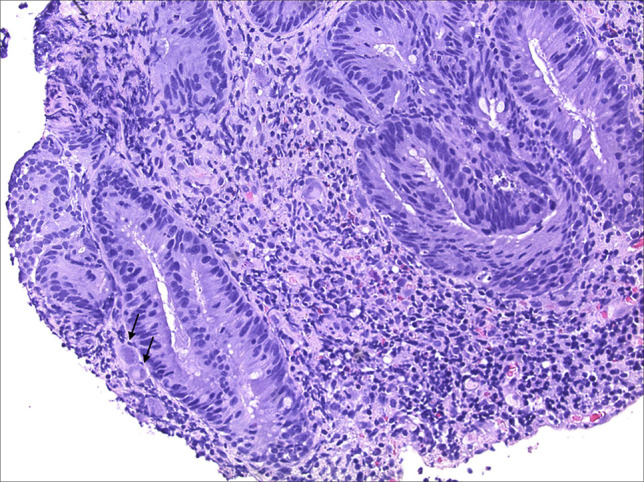 Figure 4
Figure 4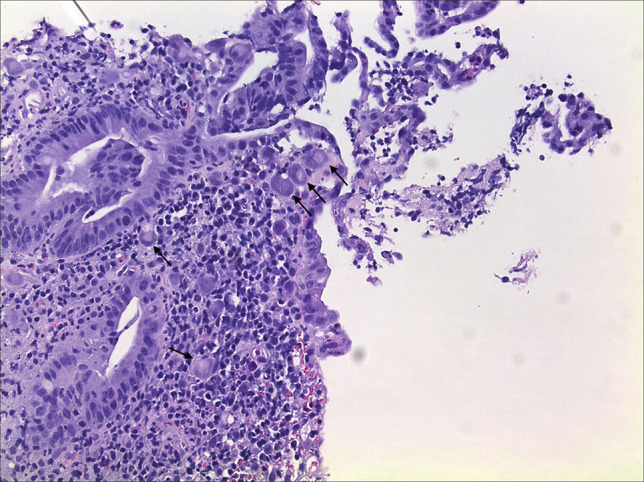 Figure 5
Figure 5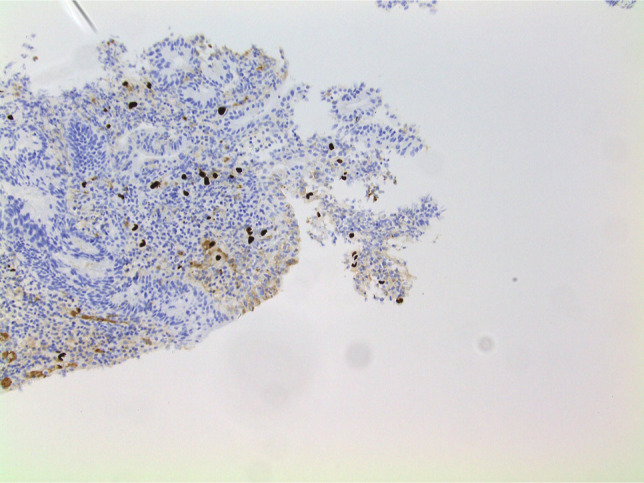 Figure 6
Figure 6| Lab test | At presentation | Follow-up | Reference range |
| Hemoglobin (g/L) | 125 | 131 | 140–175 |
| White blood cells (×109/L) | 6.5 | 7.4 | 4–11 |
| Neutrophils (×109/L) | 4.2 | 5.3 | 1.8–7.5 |
| Lymphocytes (×109/L) | 1.8 | 1.7 | 1.2–3.5 |
| Monocytes (×109/L) | 0.4 | 0.2 | 0.2–0.8 |
| Eosinophils (×109/L) | 0.0 | 0.1 | 0.0–0.5 |
| Basophils (×109/L) | 0.1 | 0.1 | 0.0–0.2 |
| Platelets (×109/L) | 197 | 268 | 150–400 |
| CRP (mg/L) | 45 | 0.6 | 0–10 |
| ALT (IU/L) | 102 | 53 | 5–40 |
| Albumin (g/L) | 31 | 43 | 35–51 |
| ALP (IU/L) | 73 | 60 | 40–125 |
| Total bilirubin (mmol/L) | 7 | 6 | 3–17 |
| CMV quantitative PCR copies/mL | 64,822 | 26 | <20 copies/mL |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCytomegalovirus and herpesvirus research · Mycobacterium research and diagnosis · Herpesvirus Infections and Treatments
INTRODUCTION
Cytomegalovirus (CMV) is a double-stranded DNA virus with a global seroprevalence of 45%–100%.^1^ Most individuals infected by CMV will exhibit lifelong latency; however, the virus can reactivate under an impaired immune state, most commonly in transplant recipients, those receiving immunosuppressive therapy, or patients with immunosuppressive diseases such as human immunodeficiency virus (HIV)/AIDS. Reactivation of the virus can lead to widespread end organ damage including hepatitis, colitis, pneumonitis, myocarditis, and encephalitis.^2^ Despite the high seroprevalence of CMV, clinically significant CMV disease rarely occurs in immunocompetent patients.^2^ However, CMV colitis is more likely to occur in immunocompetent individuals with inflammatory bowel disease (IBD), diabetes mellitus, and chronic kidney disease.^3^ We report a case of CMV colitis presenting as acute appendicitis in an immunocompetent patient known for ulcerative colitis (UC).
CASE REPORT
A 71-year-old man presented to the emergency room with a history of 10 days of intermittent fevers (objectified fever of 40°C at home), lower abdominal discomfort, and constipation of 4 weeks duration. The patient was known for UC, type 2 diabetes mellitus, dyslipidemia, and benign prostatic hyperplasia. Medications included oral and topical mesalamine, metformin, sitagliptin, gliclazide, canagliflozin, aspirin, rosuvastatin, and alfuzosin. He had no allergies and did not smoke or drink alcohol.
The patient's vital signs revealed a fever of 38.2°C with all other parameters within normal limits. He was alert and oriented. His abdomen was soft, with some right lower quadrant fullness but no significant tenderness. The remainder of his physical examination was noncontributory.
Initial biochemical workup revealed anemia (hemoglobin 125 g/L), hypoalbuminemia (31 g/L), elevated alanine transaminase (102 IU/L), and elevated C-reactive protein (45 mg/L) (see Table 1 for further details). Computed tomography scan of the abdomen and pelvis revealed a retrocolic appendix with wall thickening, increased diameter, surrounding fat stranding, and edema of the cecal base, consistent with acute uncomplicated appendicitis. In addition, there was evidence of rectal wall edema, in keeping with possible proctitis. The patient was subsequently admitted by the general surgery service and was started on broad-spectrum antibiotics (piperacillin–tazobactam) and intravenous fluids for an acute appendicitis.
Over the next 24 hours and despite antibiotic therapy, the patient remained intermittently febrile and began experiencing diarrhea with mild hematochezia. His C-reactive protein value continued to rise (maximally 65 mg/L). An initial infectious workup was negative for hepatitis A, B, and C, Epstein–Barr virus, HIV, syphilis, as well as for bacterial bloodstream and urine infections. CMV serum IgG, IgM, and viral load were requested.
Given the new onset of diarrhea and hematochezia, a colonoscopy was performed on day 3 of his admission. It revealed severely ulcerated proctitis in the distal 8 cm of the colon (Mayo UC endoscopic score = 3), scattered erosions throughout the remaining colonic segments, and edema surrounding the appendiceal orifice (see Figures 1–3). A diagnosis of acute IBD flare and incidental acute appendicitis was entertained, but the decision to initiate immunosuppressive therapy was delayed until pathologic examination of the biopsies taken during colonoscopy was completed.
Ulcerated and inflamed distal colon.
Ulcerated and inflamed distal colon.
Appendiceal orifice with surrounding edema.
The next day, serologies resulted positive for CMV IgG and IgM. Given the atypical course with ongoing fever for 21 days despite antibiotics, mild transaminitis and positive CMV IgM and IgG, intravenous ganciclovir therapy was started for suspected CMV colitis on a background of mild-to-moderate UC flare. Piperacillin–tazobactam was discontinued.
Within 48 hours of receiving ganciclovir, the fever resolved, and the diarrhea improved. The examination of colonic biopsies revealed focal active colitis in the ascending, transverse, and descending colon with positive CMV immunostaining (see Figures 4–6). In addition, there was a background of mild-to-moderate chronic active colitis in the sigmoid colon and rectum, indicating UC disease activity. Biopsies of the appendiceal base revealed only congested colonic mucosa. Subsequently, results of the quantitative serum CMV viral load showed 64,822 copies/mL (normal <20 copies/mL).
Colonic mucosa with marked cells showing characteristic features of cytomegalovirus infection, including cytomegaly, enlarged nuclei, and typical “owl-eye” intranuclear inclusions (200× magnification).
Colonic mucosa with marked cells showing characteristic features of cytomegalovirus infection, including cytomegaly, enlarged nuclei, and typical “owl-eye” intranuclear inclusions (200× magnification).
Confirmatory immunohistochemistry staining done with cytomegalovirus antibody (200× magnification).
Over the ensuing days, the patient's diarrhea and hematochezia resolved, and he was discharged home on oral valganciclovir and his home regimen of oral and topical mesalamine. At follow-up 2 weeks after discharge, the patient continued to have no gastrointestinal symptoms, his C-reactive protein and alanine aminotransferase had normalized, and quantitative CMV viral load had decreased to 26 copies/mL.
DISCUSSION
We report a rare case of CMV colitis presenting as acute appendicitis in context of a UC flare in an immunocompetent host. The case is remarkable for a few reasons.
First, the patient was immunocompetent at the baseline, having a normal immune system and no exposure to systemic corticosteroids or immunomodulating medications before presentation. Although clinically dormant in most immunocompetent hosts, CMV reactivation has long been associated with UC, usually occurring in context of severe flares requiring systemic immunosuppression or colectomy.^4^ The prevalence of reactivation seems to mirror flare severity, with more than 30% of steroid-refractory patients exhibiting evidence of concurrent colonic CMV disease.^5^ This case is atypical in that the underlying UC flare was mild-to-moderate in nature, and the patient exhibited clinical CMV colonic disease even in the absence of steroid and/or immunomodulator therapy for IBD.
Furthermore, the patient's CMV colitis presented uncharacteristically with clinical and radiologic findings of acute appendicitis, and he only developed the more typical symptoms of diarrhea and hematochezia later in his admission. A recent review of CMV disease of the gastrointestinal tract^1^ reports that immunocompetent patients can present with features not typical of gastrointestinal infections, including ischemic enterocolitis and vasculitis-like symptoms. Most CMV appendicitis cases occur in patients with underlying immune system dysfunction, including HIV/AIDS, solid-organ and hematopoietic stem cell transplant recipients.^6–8^ There are only 4 other published cases of CMV appendicitis occurring in immunocompetent hosts, thus adding to the distinctiveness of this case.^9^ The presentation and disease course of the other cases in the literature resemble our own in that the immunocompetent patients presented with atypical gastrointestinal symptoms, had radiologic evidence of acute appendicitis, did not improve with standard antibiotic therapy, and were subsequently diagnosed with primary CMV infection of the appendix and/or colon, which then improved with adequate antiviral therapy.^9^
Whether CMV reactivation is a consequence of an acute UC flare or plays an active role in propagating the underlying IBD remains to be fully elucidated. Still, there is a growing body of evidence that treatment of underlying CMV colitis, when discovered during an acute UC flare, is indicated and can improve outcomes in the form of lower colectomy rates, especially for patients with high CMV tissue viral loads.^10^ As such, gastroenterologists must maintain a high degree of suspicion for comorbid CMV colitis when assessing their patients with UC presenting with acute IBD symptoms, as early recognition and treatment can importantly impact clinical outcomes.
DISCLOSURES
Author contributions: A. Pedicelli and A. Zoughlami: conceptualization, manuscript writing, editing; O. Aleynikova: editing, pathology slides; C. Miller, C. Greenaway: conceptualization, editing. A. Pedicelli is the article guarantor.
Financial disclosure: None to report.
Informed consent was obtained for this case report.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Yeh PJ Wu RC Chen CL Cytomegalovirus diseases of the gastrointestinal tract in immunocompetent patients: A narrative review. Viruses. 2024;16(3):346.38543712 10.3390/v 16030346 PMC 10975113 · doi ↗ · pubmed ↗
- 2Salehi M Shafiee N Moradi M. Cytomegalovirus colitis in immunocompetent hosts: A case report and literature review. Clin Case Rep. 2024;12(1):e 8435.38197061 10.1002/ccr 3.8435 PMC 10774537 · doi ↗ · pubmed ↗
- 3Fakhreddine AY Frenette CT Konijeti GG. A practical review of cytomegalovirus in gastroenterology and hepatology. Gastroenterol Res Pract. 2019;2019:6156581.30984257 10.1155/2019/6156581 PMC 6431500 · doi ↗ · pubmed ↗
- 4Sager K Alam S Bond A Chinnappan L Probert CS. Review article: Cytomegalovirus and inflammatory bowel disease. Aliment Pharmacol Ther. 2015;41(8):725–33.25684400 10.1111/apt.13124 · doi ↗ · pubmed ↗
- 5Singh G Rentsch C Beattie W Christensen B Macrae F Segal JP. Long-term follow up of patients treated for inflammatory bowel disease and cytomegalovirus colitis. Diagnostics. 2024;14(18):2030.39335709 10.3390/diagnostics 14182030 PMC 11431378 · doi ↗ · pubmed ↗
- 6Valerdiz-Casasola S Pardo-Mindan FJ. Cytomegalovirus infection of the appendix in patient with the acquired immunodeficiency syndrome. Gastroenterology. 1991;101(1):247–9.1646140 10.1016/0016-5085(91)90485-4 · doi ↗ · pubmed ↗
- 7Mc Carty TP Lee RA Herfel BM Pappas PG. Cytomegalovirus appendicitis in solid organ transplant patients, two cases and a review. J Clin Virol. 2015;66:48–50.25866336 10.1016/j.jcv.2015.03.004 · doi ↗ · pubmed ↗
- 8Kothari A Caradine KD Rico Crescencio JC, et al. Cytomegalovirus appendicitis after hematopoietic stem cell transplantation. Transpl Infect Dis. 2017;19(5):e 12747.10.1111/tid.1274728708253 · doi ↗ · pubmed ↗