Therapeutic Landscape of Rosacea: From Clinical Trials to Future Directions
Sitong Li, Jiacheng Lin, Jiaqi Li, Xiaohui Mo, Qiang Ju

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
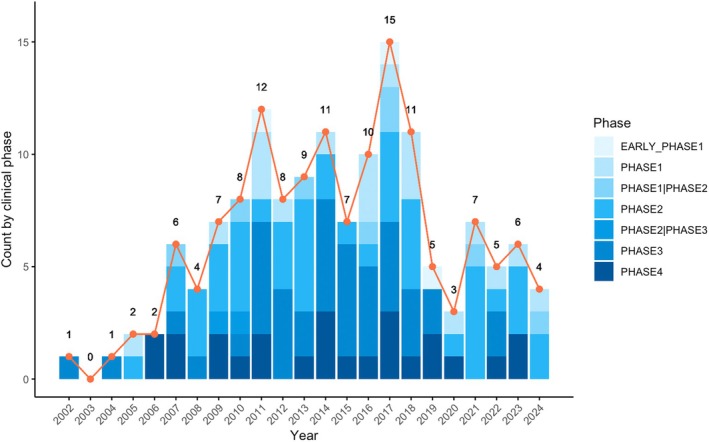 FIGURE 1
FIGURE 1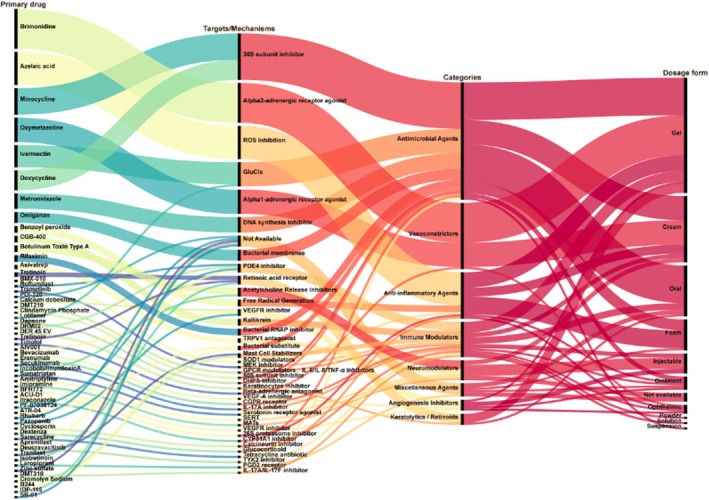 FIGURE 2
FIGURE 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAcne and Rosacea Treatments and Effects · Bee Products Chemical Analysis · Pharmacological Effects of Natural Compounds
To the Editor,
Rosacea is a chronic inflammatory skin condition characterized by facial flushing, persistent erythema, papules, pustules, and telangiectasia that impair patients' quality of life [1]. Despite its prevalence, the pathogenesis remains poorly understood, and current treatments often show limited efficacy [2]. This study analyzes rosacea‐related clinical trials to identify research gaps and therapeutic directions. We searched ClinicalTrials.gov on September 28, 2024, identifying 186 eligible interventional studies. We evaluated trial phases, start years, and primary purposes, focusing on 138 drug‐related and 26 non‐drug trials.
Between 2002 and 2024, 186 rosacea‐related trials were registered across all phases (Figure 1). Of these, 42 trials did not specify a phase, likely reflecting non‐traditional designs or unique interventions. Among 144 trials with defined phases, Phase 2 trials were most frequent (n = 46), followed by Phase 3 (n = 41). From 2002 to 2010, trial numbers remained relatively low during this exploratory stage. The period from 2011 to 2017 marked peak activity, particularly in Phase 2 and 3 trials, indicating the advancement of many therapies into mid‐ and late‐stage clinical validation. Although registrations decreased from 2018 to 2024, research interest remains substantial. Of the 186 trials, 164 focused on treatment, while 22 addressed non‐treatment areas, including basic science(n = 6), diagnostics(n = 2), supportive care(n = 5) and other intervention(n = 9). Among treatment‐focused trials, non‐drug interventions (n = 26) included dietary supplements (n = 2), skincare products (n = 6), and physical therapies (n = 18). Drug‐based trials were dominated by topical treatments (n = 109), followed by oral (n = 23), injectable (n = 9), and ophthalmic (n = 4) routes.
The distribution of clinical trials across different phases and years.
Our analysis of drug categories and therapeutic targets reflects the ongoing effort to address rosacea's complex pathophysiology through diversified treatment strategies (Figure 2). Antimicrobial agents were most common (36.55%), followed by vasoconstrictors (20.69%) and anti‐inflammatory drugs (14.48%). While traditional antimicrobial and anti‐inflammatory therapies remain central, the increasing use of vasoconstrictors reflects growing recognition of vascular regulation as a critical therapeutic target. Since 2007, vascular abnormalities have attracted attention for their role in persistent erythema and flushing. VEGF polymorphisms may contribute to pathogenesis by promoting vascular dysfunction and inflammatory responses [3]. Novel targets, such as IL‐17 and TYK2 inhibitors, suggest innovative pathways in immune regulation [4], while TRPV1 antagonists highlight the potential of neural pathway modulation [5]. Since 2011, research has increasingly focused on immune and neural regulation, particularly examining the relationship between Demodex mites and immune dysfunction. The expanding use of ivermectin demonstrates its dual function in controlling mite infestation and modulating immune responses [6]. Physical therapies, including PDL and IPL, have been incorporated to improve vascular symptom control. The limitations of single‐target therapies have driven the exploration of multi‐target combinations. Beyond optimizing existing drugs through novel formulations (foams and powders), several innovative therapies, such as ATR‐04 (bacterial substitute) and deucravacitinib (TYK2 inhibitor), have entered clinical trials.
A Sankey diagram illustrating the relationships between primary drugs, their mechanisms of action, drug categories, and dosage forms. GluCls, Glutamate Chloride Channels; PDE4, Phosphodiesterase 4; VEGFR, Vascular Endothelial Growth Factor Receptor; VEGF‐A, Vascular Endothelial Growth Factor‐A; RNAP, RNA Polymerase; TRPV1, Transient Receptor Potential Vanilloid 1; SOD1, Superoxide Dismutase 1; MEK, Mitogen‐Activated Protein Kinase Kinase; GPCR, G‐Protein‐Coupled Receptor; IL‐6, Interleukin 6; IL‐8, Interleukin 8; TNF‐α, Tumor Necrosis Factor Alpha; DHPS, Dihydropteroate Synthase; CGPR, Calcitonin Gene‐Related Peptide Receptor; IL‐17A, Interleukin 17A; IL‐17F, Interleukin 17F; SERT, Serotonin Transporter; MATs, Monoamine Transporters; TYK2, Tyrosine Kinase 2.
This study has limitations due to restricted information availability in ClinicalTrials.gov. We supplemented our analysis with data from DrugBank and Synapse to better understand drug mechanisms and targets. Our findings reveal key trends: (1) sustained research interest in rosacea, (2) diversified therapeutic strategies encompassing antimicrobial, immune‐modulatory, and neuro‐vascular‐regulatory approaches, (3) continued focus on topical formulations, and (4) emergence of new targets and innovative formulations. Although progress has been made, unmet clinical needs persist, emphasizing the importance of personalized treatment strategies and long‐term efficacy evaluations.
Disclosure
The authors have nothing to report.
Conflicts of Interest
The authors declare no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1D. Thiboutot , R. Anderson , F. Cook‐Bolden , et al., “Standard Management Options for Rosacea: The 2019 Update by the National Rosacea Society Expert Committee,” Journal of the American Academy of Dermatology 82 (2020): 1501–1510.32035944 10.1016/j.jaad.2020.01.077 · doi ↗ · pubmed ↗
- 2L. M. C. Almeida , M. Ianhez , T. Dal'Forno , et al., “Long‐Term Maintenance Treatment of Rosacea: Experts' Opinion,” International Journal of Dermatology 63, no. 1 (2024): 94–101, 10.1111/ijd.16920.38013632 · doi ↗ · pubmed ↗
- 3Y. Hayran , I. Lay , M. C. Mocan , T. Bozduman , and S. Ersoy‐Evans , “Vascular Endothelial Growth Factor Gene Polymorphisms in Patients With Rosacea: A Case‐Control Study,” Journal of the American Academy of Dermatology 81 (2019): 348–354.31182382 10.1016/j.jaad.2019.03.055 · doi ↗ · pubmed ↗
- 4A. Amir Ali , R. Vender , and R. Vender , “The Role of IL‐17 in Papulopustular Rosacea and Future Directions,” Journal of Cutaneous Medicine and Surgery 23 (2019): 635–641.31402691 10.1177/1203475419867611 · doi ↗ · pubmed ↗
- 5T. Xiao , M. Sun , C. Zhao , and J. Kang , “TRPV 1: A Promising Therapeutic Target for Skin Aging and Inflammatory Skin Diseases,” Frontiers in Pharmacology 14 (2023): 1037925.36874007 10.3389/fphar.2023.1037925 PMC 9975512 · doi ↗ · pubmed ↗
- 6E. D. Deeks , “Ivermectin: A Review in Rosacea,” American Journal of Clinical Dermatology 16 (2015): 447–452.26254001 10.1007/s 40257-015-0150-8 · doi ↗ · pubmed ↗