Corrigendum: Headache among combat-exposed veterans and service members and its relation to mild TBI history and other factors: a LIMBIC-CENC study
William C. Walker, Sarah W. Clark, Kaleb Eppich, Elisabeth A. Wilde, Aaron M. Martin, Chelsea M. Allen, Melissa M. Cortez, Mary Jo Pugh, Samuel R. Walton, Kimbra Kenney

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
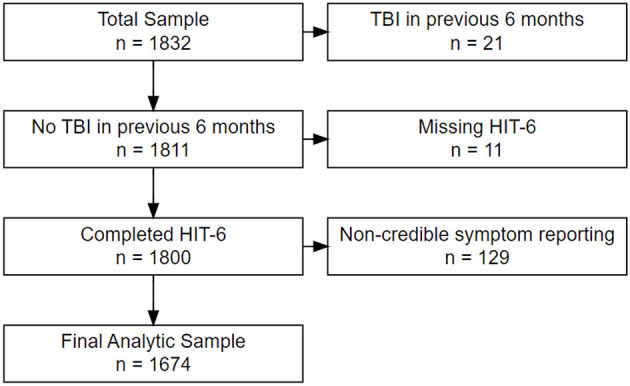 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMigraine and Headache Studies
In the published article, there was an error in “Figure 1. Study Sample Inclusion Flow Diagram”. After publication, the authors were informed that one site's IRB retroactively deemed their data to be invalid, and therefore cannot be published (Site #10; Eisenhower Army Medical Center; located near Augusta, GA). The updated figure reflects changes excluding the removed data and updated the results data in all main Tables and supplementary Tables; Table 1. Headache (HA) prevalence (experienced HA lately) stratified by # lifetime mTBIs; Table 2. Headache (HA) impact stratified by # lifetime mTBIs; Table 3. Post-hoc comparisons of HIT-6 headache severity categories by # lifetime mTBIs; Table 4. Categorical covariates stratified by absence/presence of Headache (HA); Table 5. Continuous covariates stratified by absence/presence of Headache (HA); Table 6. Multivariable logistic regression—experience headaches lately yes/no; Table 7. Multivariable linear regression for HIT-6 total score (multiple R^2^ = 0.350).
In the article, there were errors in the following supplementary tables as published. Supplementary Table 1. Post-hoc comparisons HIT-6 Total Sore by Number of mild TBI groups; Supplementary Table 2. Post-hoc comparisons of HIT-6 Impact categories by Number of mild TBI groups; Supplementary Table 3. Prevalence of Headache Lately; Logistic regression sensitivity analysis including only mTBI positive participants (N = 1,234); Supplementary Table 4. Headache Impact (HIT6 Total Score); Linear Regression sensitivity analysis including only mTBI positive participants who endorsed HA Lately (N = 853).
In the published article, there were errors in the Abstract, Methods and Results sections as published. They should have been written as:
Methods: Participants with non-credible symptom reporting were excluded, leaving N = 1,674 of whom 81% had positive mTBI histories.
Results: In covariate-adjusted analysis, HA prevalence was higher with greater number of blast-related mTBIs (OR 1.81; 95% CI 1.48, 2.23) non-blast mTBIs while deployed (OR 1.42; 95% CI 1.14, 1.79), or non-blast mTBIs when not deployed (OR 1.23; 95% CI 1.02, 1.49).
In the published article, there were errors in the Methods, Participants section as published. This should have been written as:
For this secondary analysis, all LIMBIC-CENC PLS participants whose enrollment (baseline) assessment data were available at time of dataset extraction were included (n = 1,832). …. We also excluded participants with evidence of noncredible symptom reporting based on failing (126) the Mild Brain Injury Atypical Symptom (mBIAS) scale, a validated self-reported measure of symptom reporting credibility in the mTBI population using the developer's recommended cut-point of 8 or higher (Cooper et al., 2011). This left a final analytic sample of 1,674 participants (see Figure 1).
In the published article, there were errors in the Results section as published. This should have been written as:
In our final sample of 1,674 combat-exposed current and former SMs, 19% had an entirely negative lifetime mTBI history, 47% had sustained 1-2 mTBIs, and 34% had 3 or more. Rates of positive history across the mTBI mechanism/setting categories were 63% for Combat mTBI(s), 67% for Non-combat mTBI(s), and 37% for Blast-related mTBI(s).
In the published article, there were errors in the Results, HA prevalence and impact across mTBI history groups (0, 1–2, 3+) section as published. This should have been written as:
For example, the rate of severe HA pain sometimes, often or always was 70% for the no TBI group compared to 78% for those with 1-2 or 3+ lifetime mTBIs. (See Table 3 for HIT-6 item #1 post-hoc testing; the other post-hoc testing data are available in Supplementary Tables S1, S2).
In the published article, there were errors in the Results, Main multivariable regression analyses section as published. This should have been written as:
For TBI history, the number of lifetime mTBIs of every type was significant, including blast-related (OR = 1.80), Blunt during combat-deployment (OR = 1.41), and Blunt outside of deployment (OR = 1.23). Other significant factors included identifying as female (OR = 3.57), age (0.76), total months combat-deployed (OR = 1.23), and symptoms of depression on PHQ-9 (OR = 1.56), PTSD on PCL-5 (OR = 1.54), and disturbed sleep quality on PSQI (OR = 1.78).
For TBI history, only blast-related mTBIs were significant (Beta 0.57). Blunt-only mTBIs did not reach significance, regardless of contextual type (combat or non-combat). Other factors found significant in the HIT-6 linear regression that were also significant in the HA prevalence logistic regression were female identity (Beta 3.4), younger age (Beta −0.98), PTSD symptoms (Beta 4.9), and reduced sleep quality (Beta 1.4). Demographic characteristics that were significant in the HIT-6 score linear regression model but not the preceding HA prevalence model were Black racial identity (Beta 2.3) and Hispanic/Latino ethnic identity (Beta 2.0) as compared with White/non-Hispanic racial/ethnic identity.
In the published article, there were errors in the Discussion section as published. This should have been written as:
Discussion
The overall sample (n = 1,674), which included 19% with negative TBI histories, had a HA point prevalence (i.e., HA lately) of 65%.
The covariate-adjusted logistic regression model for HA prevalence (see Table 6) showed higher prevalence with a greater number of any subtype of mTBI (see Table 6), with the nominally highest OR for blast-related mechanism (OR 1.80; 95% CI 1.47, 2.22).
Our large sample, which included 215 females (13%), enabled us to examine their relative risk for HA, a previously understudied research question in the military population due to insufficient numbers of females in most prior HA studies. Our results show that female sex had the nominally highest OR (3.57; 2.37, 5.48) for experiencing HA lately (see Table 6), and had a strong association with higher HA impact (Beta 3.4; 2.1, 4.8; see Table 7).
In the published article, there were errors in the Discussion, Study strengths section as published. This should have been written as:
Study strengths included our large sample (n = 1,674) of individuals with military combat exposure drawn from the LIMBIC-CENC multicenter cohort with rigorously determined lifetime mTBI histories and a large breadth of data available from their comprehensive assessments.
The authors apologize for this error and state that this does not change the scientific conclusions of the article in any way. The original article has been updated.