Prevalence of Delayed Initiation of Breastfeeding and Its Associated Factors Among Mothers Who Gave Birth by Cesarean Section in Gamo and Gofa Zones, Southern Ethiopia: A Multicenter Cross-Sectional Study
Arega Abebe Lonsako, Tsehaynew Kasse, Aster Dure, Abera Cheru, Kinde Kibe, Addisalem Haile

TL;DR
This study finds that over half of mothers who had cesarean births in Ethiopia started breastfeeding late, with lack of support and counseling being key factors.
Contribution
The study identifies specific factors linked to delayed breastfeeding initiation after cesarean births in a region with limited prior research.
Findings
53.4% of mothers who had cesarean births initiated breastfeeding late.
Lack of professional assistance and skin-to-skin contact were strongly associated with delayed breastfeeding.
Postcesarean counseling significantly influenced early breastfeeding initiation.
Abstract
Background: Delayed initiation of breastfeeding after birth can negatively impact maternal and newborn health, significantly increasing neonatal mortality. Due to the rising number of cesarean deliveries, the risk of delayed breastfeeding initiation is imminent. However, there is limited evidence on delayed initiation of breastfeeding among mothers who gave birth by cesarean section in Ethiopia. Thus, this study aims to assess factors associated with delayed initiation of breastfeeding among mothers who gave birth by cesarean section in public health facilities of Gamo and Gofa zones, south Ethiopia. Methods: This multicenter, facility-based, cross-sectional study was conducted across five hospitals in the Gamo and Gofa zones that offer cesarean delivery services. A consecutive sampling technique, which involves selecting every eligible subject until the desired sample size is reached,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
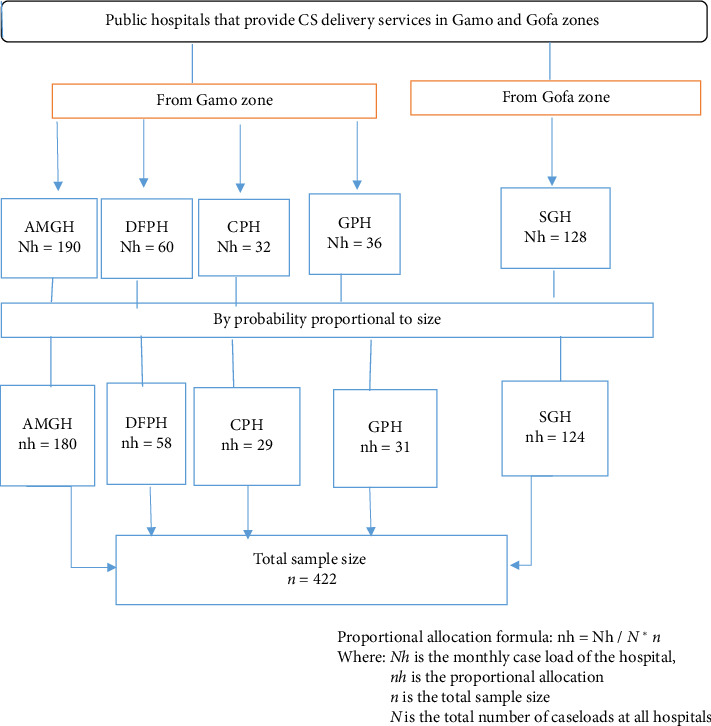 Figure 1
Figure 1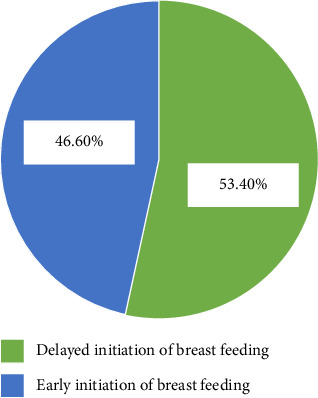 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBreastfeeding Practices and Influences · Global Maternal and Child Health · Child Nutrition and Water Access
1. Introduction
Delayed initiation of breastfeeding is defined as starting breastfeeding more than 1 hour after birth and can have significant health consequences [1]. The World Health Organization (WHO) and United Nations International Children's Emergency Fund [2] strongly advocate for breastfeeding within the first hour of birth, emphasizing its profound benefits for both the mother and the baby [3]. For the mother, it aids uterine contractions, reduces postpartum bleeding, promotes quicker weight loss, and lowers the risk of breast cancer later in life. Similarly, for the newborn, it is crucial for strengthening the mother-child bond and supporting cognitive and immune system development [4, 5].
Delayed initiation of breastfeeding significantly increases the risk of neonatal mortality, primarily due to hypothermia and infections. A study shows that initiating breastfeeding more than an hour after birth, but within the first 24 h, increases the risk of neonatal mortality by 40%. If breastfeeding is delayed beyond 24 h, this risk increases by 80% [6, 7]. Additionally, it can also increase the likelihood of common neonatal illnesses such as upper respiratory symptoms and vomiting. These findings highlight the critical role of early breastfeeding in reducing neonatal mortality and promoting infant health [8, 9].
Globally, neonatal mortality remains a pressing issue, with 2.4 million neonates dying within the first month of life in 2020. Alarmingly, approximately 6500 neonatal deaths occurred daily, and nearly 75% of these deaths happened within the first week of life, often from preventable causes including infections and delayed breastfeeding initiation [2, 10]. In sub-Saharan Africa, the neonatal mortality rate remains the highest globally, with 27 deaths per 1000 live births recorded in 2019 with nearly one million newborns dying within 24 h. Ethiopia, one of the top ten Sub-Saharan African countries in terms of neonatal mortality, recorded a neonatal mortality rate of 30 deaths per 1000 live births in 2019 [11].
Further, the increasing rate of cesarean delivery poses a significant challenge, as it is linked to delayed breastfeeding initiation, which can negatively impact neonatal health. Addressing this issue requires improved maternal care practices and policies [12]. Globally, the cesarean delivery rate stands at 21.1% [13]. In sub-Saharan Africa, cesarean delivery rates range from 2% to 51%, with Ethiopia's rate at 29.55%, and a recent study covering public hospitals in the Gamo, Gofa, and South Omo zones of Southern Ethiopia reported a cesarean delivery rate exceeding the World Health Organization's recommended range of 10%–15% [14, 15].
The Federal Ministry of Health (FMOH) of Ethiopia has made significant efforts to promote optimal breastfeeding practices through initiatives such as the National Nutrition Program II (NNP II) and the National Guideline on Adolescent, Maternal, Infant, and Young Child Nutrition (AMIYCN) [16]. Despite these efforts, delayed initiation of breastfeeding remains a pressing public health concern, particularly among mothers who undergo cesarean sections [17]. Nationally, 26.4% of mother's experience delays in starting breastfeeding, with considerable regional disparities. This challenge is exacerbated by weak implementation of newborn care standards and structural, social, and clinical barriers, including inadequate antenatal care, unplanned pregnancies, and the rising rate of cesarean deliveries [15, 18, 19].
Moreover, most previous studies have primarily focused on the general postpartum population, overlooking mothers who gave birth by cesarean section, particularly in the study area. Understanding the context-specific determinants of delayed initiation of breastfeeding among this group is critical for addressing the issue and improving neonatal health outcomes. Therefore, this study aimed to assess the prevalence and associated factors of delayed initiation of breastfeeding among mothers who gave birth by cesarean section in Gamo and Gofa zones of the south Ethiopia region.
2. Methods
2.1. Study Setting
A multicenter, cross-sectional study was conducted from March 20 to May 21, 2023, in five selected hospitals in the Gamo and Gofa zones of Southern Ethiopia, which are part of the Southern Ethiopia region. The administrative centers, Arba Minch (Gamo Zone) and Sawla (Gofa Zone), are located 434 km and 455 km south of Addis Ababa, the capital of Ethiopia, respectively. According to population projections based on the 2007 Ethiopian census, the study area had an estimated population of 2,658,345 in 2017/18. The study was conducted in two general hospitals (Arba Minch and Sawla) and three primary hospitals (Dilfana, Chencha, and Gerese), which provide curative, preventive, and rehabilitative services to the population [20].
2.2. Population
All mothers who gave birth by cesarean section in public hospitals of Gamo and Gofa zones were considered as the source population, whereas all mothers who gave birth by cesarean section in selected public hospitals during the data collection period were the study population.
2.3. Eligibility Criteria
All mothers who gave birth by cesarean section under spinal anesthesia were included in the study. Mothers who gave birth under general anesthesia, whose newborns were admitted to the neonatal intensive care unit, and who were unable to respond due to critical illness were excluded.
2.4. Sample Size Determination
The required sample size was calculated using a single population proportion formula with the following assumptions: a proportion (p) of 50%, as no prior studies were available in this subject matter, a 95% confidence interval, a 5% margin of error, and an additional 10% to account for the potential nonresponse. The final sample size was 422.
2.5. Sampling Techniques and Procedures
This study included five hospitals in the Gamo and Gofa zones that provide cesarean delivery services. The sample size was proportionally distributed based on each hospital's average monthly cesarean delivery caseload; totally, it was 446: Arba Minch General Hospital (AMGH 180), Dilfana Primary Hospital (DFPH 58), Chencha Primary Hospital (CPH 29), Gerese Primary Hospital (GPH 31), and Sawela General Hospital (SGH 124) (Figure 1).
A consecutive sampling technique was employed, recruiting women who delivered by cesarean section during the data collection period. Participants were informed about the study objectives, provided voluntary consent, and were interviewed using a structured questionnaire. No monetary or material compensation was offered, but participants were encouraged to contribute to improving maternal and child health services in the region.
2.6. Data Collection Instruments and Procedures
The data collection tools were adapted from WHO indicators to assess early initiation of breastfeeding [21] and modified by reviewing the relevant literature [22–26]. The tools included sections on socio-demographic characteristics, delayed initiation of breastfeeding, obstetric and health service-related factors, and newborn-related factors. The questionnaire was originally prepared in English and then translated into local languages (Gamo and Gofa). A language expert performed a back translation into English to ensure its consistency. The data were collected by six bachelor-level nurses under the supervision of four supervisors who hold master's degrees in maternity nursing. Respondents were given a brief orientation about the study's purpose and were interviewed face-to-face, with their medical record reviewed for additional information.
2.7. Variables of the Study
In this study, the dependent variable was delayed initiation of breastfeeding, while the explanatory variables included maternal age, educational level, employment status, place of residence, number of antenatal care visits, type of pregnancy, counseling about early initiation of breastfeeding during ANC follow-up, postnatal counseling, obstetric complications, assistance from health professionals for early initiation of breastfeeding, early skin-to-skin contact with the newborn, prior knowledge of early initiation of breastfeeding, previous breastfeeding experiences, prelacteal feeding practices, birth weight, Apgar score, and sex of the newborn.
2.8. Operational Definition and Measurement
2.8.1. Delayed Initiation of Breastfeeding
It was defined as failure to initiate breastfeeding within 1 h after birth as WHO recommendation. The outcome variable was dichotomized as “1” for delayed initiation and “0” for early initiation [1].
2.8.2. Breastfeeding
It refers to the practice of feeding an infant with milk directly from a woman's breast. Health organizations, including the WHO, recommend initiating breastfeeding within the first hour of birth and continuing as the baby desires [1].
2.8.3. Prelacteal Feeding
This practice refers to providing any liquid or solid food other than the mother's breast milk to a newborn before initiating breastfeeding. Responses were recorded as “Yes” if the newborn was given any liquid or solid food other than breast milk before breastfeeding started and “No” if no such liquid or solid food was given before breastfeeding began [27].
2.8.4. Health Professionals' Assistance
This refers to the support provided by healthcare professionals to help the mother and the newborn with proper attachment and positioning to start breastfeeding within the first hour after birth. If such assistance is not provided, it means that the mother did not receive professional help to initiate breastfeeding on time [28].
2.9. Data Quality Control
A pretest was conducted on 5% of the total sample size at the Jinka General Hospital to ensure data quality. Based on the pretest results, necessary modifications were made, and the modified tools were used for the actual data collection. The data collectors and supervisors were trained on the objectives, the data collection process, and ethical consideration. Data collectors were closely supervised and instructed to check the completeness of data.
2.10. Data Analysis and Processing
The collected data were cleaned, coded, and entered into the Epi-Data version 3.1 software. Then, the data were exported to SPSS version 26 for analysis. Descriptive analysis was employed to summarize the participants' characteristics, with the results presented in text, tables, and figures. A binary logistic regression model was used to explore the association between each independent variable and the outcome variable. Independent variables with a p value of less than 0.25 in the bivariate analysis were included in the multivariable analysis. Multicollinearity was assessed using the variance inflation factor, none of the variables yielding VIF greater than 10. While the model's fitness was evaluated using the Hosmer–Lemeshow goodness-of-fit test, it was founded to be insignificant (p value: 0.481). Adjusted odds ratios (AOR) with 95% confidence intervals (CI) were reported, and variables with a p value < 0.05 were declared to be significantly associated with delayed initiation of breastfeeding.
2.11. Ethical Considerations
Ethical approval was obtained from the Institutional Review Board [29] of the Arba Minch University College of Medicine and Health Sciences (IRB/1476/2023). In addition, permission was obtained from the Arba Minch General Hospital, the Dilfana Primary Hospital, the Chencha Primary Hospital, the Gerese Primary Hospital, and the Sawela General Hospital. Before data collection, informed consent was obtained from the study participants, and the right to withdraw from the interview was guaranteed. The privacy and confidentiality of the information obtained from the respondents were kept confidential and anonymous.
3. Results
3.1. Sociodemographic Characteristics of Participants
A total of 416 mothers who gave birth by cesarean section were enrolled in this study, with a response rate of 98.5%. The mean age of the participants was 28.8 years, with standard deviation (SD) of ±3.8 years. Of the respondents, 171 (41.1%) were between the ages of 25–29 years, and 229 (55%) resided in urban areas. Regarding the educational status, 244 (58.6%) had completed secondary school and above, and 214 (51.4%) mothers were housewives (Table 1).
3.2. Mother's Obstetric and Health Service–Related Characteristics
Among the respondents, 163 (39.2%) had fewer than four antenatal care visits, and 187 (55.0%) did not receive counseling on early breastfeeding initiation during their follow-up. 206 (49.5%) reported that they did not receive assistance from healthcare professionals to initiate breastfeeding immediately after delivery. Regarding cesarean sections, 359 (86.3%) underwent unplanned procedures. Furthermore, 225 (54.1%) did not receive postnatal counseling on early breastfeeding initiation, and 124 (29.8%) did not initiate early skin-to-skin contact. Additionally, 381 (91.5%) understood the importance of colostrum for newborns, and 286 (68.7%) practiced colostrum feeding (Table 2).
3.3. Newborns' Profile of Study Participants
Out of the total 416 newborns, 240 newborns (57.7%) were male. At the 1st minute after birth, 332 newborns (79.8%) had an Apgar score of seven and above, while all newborns had an Apgar score of seven and above by the 5th minute. Additionally, 385 newborns (92.5%) were born with a normal birth weight (Table 3).
3.4. The Prevalence of Delayed Initiation of Breastfeeding
The prevalence of delayed initiation of breastfeeding among mothers who gave birth by cesarean section in this study setting was 53.4% with 95% CI: (48.5, 58.2) (Figure 2).
3.5. Factors Associated With Delayed Initiation of Breastfeeding
In the binary logistic regression analysis, rural residency, being a primiparous mother, undergoing an unplanned cesarean section, a lack of assistance from a healthcare professional, not applying early skin-to-skin contact, duration of labor, not receiving postnatal counseling about early initiation of breastfeeding, and timing of delivery were factors associated with delayed initiation of breastfeeding.
However, in the multivariable logistic regression analysis, the odds of delayed initiation of breastfeeding were two times higher among primiparous mothers than multiparous mothers (AOR = 1.9, 95% CI: 1.1, 3.5). Mothers who did not receive professional support during breastfeeding initiation were five times more likely to delay breastfeeding compared to those who received support (AOR = 5.1, 95% CI: 3.0, 8.6). Additionally, the odds of delayed initiation were three times higher for mothers who did not apply early skin-to-skin contact compared to those who did (AOR = 3.3, 95% CI: 1.7, 6.4). The odds of delayed initiation of breastfeeding were two times higher among mother who did not receive postnatal counseling about early initiation of breastfeeding compared to those who did (AOR = 2.5, 95% CI: 1.6, 3.8) (Table 4).
4. Discussion
This study aimed to determine the prevalence of delayed initiation of breastfeeding and its associated factors among mothers who gave birth via cesarean section in public health facilities in the Gamo and Gofa zones of southern Ethiopia. The findings revealed that the prevalence of delayed initiation of breastfeeding was 53.4% (95% CI: 48.5, 58.2). Factors significantly associated with delayed initiation included being a primiparous mother, a lack of healthcare professional assistance, the absence of early skin-to-skin contact, and not receiving postnatal counseling on early breastfeeding initiation.
This finding was consistent with the results of study performed in South Sudan (52%) and Addis Ababa, Ethiopia (48.8%) [30, 31]. However, this finding was higher than the results of studies conducted in Uganda (48.2%), Gondar (48.1%), and Dessie, Ethiopia (43%) [10, 22, 23]. This discrepancy may be due to differences in eligibility criteria, healthcare practices, study settings, and sampling procedures, as well as variations in the timing of the studies.
In this study, the odds of delayed initiation of breastfeeding were two times higher among primiparous mothers than multiparous mothers. This finding was supported by the result of the Ethiopian Demographic and Health Survey in 2016 [15]. This might be because primiparous mothers often lack breastfeeding experience and confidence, requiring additional support and guidance to navigate breastfeeding challenges. Conversely, multiparous women typically possess greater confidence and skills from prior experiences, enabling them to overcome common breastfeeding obstacles more effectively [32].
Mothers who did not receive professional support during breastfeeding initiation were five times more likely to delay breastfeeding compared to those who received support. This finding is consistent with studies conducted in Gondar, Addis Ababa, Ethiopia, and Uganda [31, 33]. This may be due to insufficient professional support, particularly in proper attachment and positioning, which can hinder a mother's ability to establish successful breastfeeding practices. Hands-on assistance is crucial to guide mothers on effective breastfeeding techniques, responsive feeding, and comforting their infants [34].
Additionally, the odds of delayed initiation were three times higher for mothers who did not apply early skin-to-skin contact compared to those who did. This result is consistent with studies from Malaysia and Nepal [35, 36]. A possible justification could be that early skin-to-skin contact is essential for initiating breastfeeding immediately, as it promotes bonding, triggers breastfeeding reflexes in both the mother and the newborn, and boosts the mother's confidence. Without early practice of skin-to-skin contact, mothers may feel anxious, leading to delays in breastfeeding initiation [37, 38].
The odds of delayed initiation of breastfeeding were two times higher among mother who did not receive postnatal counseling about early initiation of breastfeeding compared to those who did. This finding aligns with a study conducted in Dessie, Ethiopia [23]. This may be because postnatal counseling is essential as it provides mothers with crucial support and information, aiding in the earlier initiation of breastfeeding. It helps to overcome potential knowledge and skill deficits related to breastfeeding that may arise after delivery. Proper counseling from healthcare providers significantly enhances the likelihood of successful breastfeeding [39].
Finally, delayed initiation of breastfeeding among mothers who gave birth by cesarean section remains a significant concern. Healthcare providers must address the unique challenges faced by these mothers, offering targeted assistance in breastfeeding positioning and attachment. A tailored approach, including specific counseling strategies, is essential to meet their needs and ensure successful breastfeeding initiation.
5. Conclusion
This study reveals a high prevalence of delayed initiation of breastfeeding among mothers who underwent cesarean sections, with contributing factors including primiparity, a lack of professional support, the absence of early skin-to-skin contact, and insufficient postnatal counseling. To address these issues, we recommend that health policymakers implement supportive policies ensuring all mothers, particularly first-time ones, receive comprehensive breastfeeding support during antenatal and postnatal care. Integrating immediate skin-to-skin contact into standard postcesarean protocols and enhancing the roles of community health workers through targeted training and resources are also crucial. Healthcare professionals should provide thorough counseling on breastfeeding benefits and techniques, offer continuous professional support, and promote kangaroo care practices to improve breastfeeding outcomes. Educators and researchers are encouraged to develop specialized training programs for healthcare providers and conduct further research to identify and address additional barriers to early breastfeeding initiation postcesarean.
5.1. Limitation of the Study
The cross-sectional design prevents establishing causal relationships between delayed initiation of breastfeeding and associated factors, as data were collected at a single point in time. Future longitudinal studies are recommended to address this. Recall bias may also have affected the accuracy of self-reported data, especially on breastfeeding initiation timing. To reduce this, we used structured questions and collected data shortly after delivery.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1WHO WHO Guidelines Approved by the Guidelines Review Committee. Guideline: Protecting, Promoting and Supporting Breastfeeding in Facilities Providing Maternity and Newborn Services 2017 World Health Organization 29565522 · pubmed ↗
- 2UNICEF Neonatal Mortality 2021 UNICEF
- 3Modak A. Ronghe V. Gomase K. P. The Psychological Benefits of Breastfeeding: Fostering Maternal Well-Being and Child Development Cureus 20231510 p. e 4673010.7759/cureus.46730 PMC 1063130238021634 · doi ↗ · pubmed ↗
- 4WHO Early Initiation of Breastfeeding to Promote Exclusive Breastfeeding 2019 World Health Organization
- 5Binns C. Lee M. Low W. Y. The Long-Term Public Health Benefits of Breastfeeding Asia-Pacific Journal of Public Health 201628171410.1177/10105395156249642-s 2.0-8495529471326792873 · doi ↗ · pubmed ↗
- 6Oddy W. H. Breastfeeding in the First Hour of Life Protects Against Neonatal Mortality Jornal de Pediatria 201389210911110.1016/j.jpedp.2012.12.00123642418 · doi ↗ · pubmed ↗
- 7Phukan D. Ranjan M. Dwivedi L. Impact of Timing of Breastfeeding Initiation on Neonatal Mortality in India International Breastfeeding Journal 2018131 p. 2710.1186/s 13006-018-0162-02-s 2.0-85049428535 PMC 602903329988694 · doi ↗ · pubmed ↗
- 8Boakye-Yiadom A. P. Nguah S. B. Ameyaw E. Enimil A. Wobil P. N. L. Plange-Rhule G. Timing of Initiation of Breastfeeding and its Determinants at a Tertiary Hospital in Ghana: A Cross-Sectional Study BMC Pregnancy and Childbirth 2021211 p. 46810.1186/s 12884-021-03943-x 34193067 PMC 8247238 · doi ↗ · pubmed ↗