Development of a modular patient-reported outcome and experience measure on patient needs and benefits in CLL (PBI-CLL)
Beke Hester, Julia Von Tresckow, Minna Voigtländer, Helen Beckmann, Judith Rusch, Christine Blome

TL;DR
Researchers created a new questionnaire called PBI-CLL to capture patient needs and treatment goals in chronic lymphocytic leukaemia, aiming to support personalized treatment decisions.
Contribution
The PBI-CLL is the first modular tool to assess patient-reported outcomes and treatment preferences in CLL.
Findings
Patients with CLL have diverse treatment goals and burdens, emphasizing the need for personalized care.
The PBI-CLL questionnaire includes three modules to measure treatment outcomes, process quality, and patient preferences.
Patients found the questionnaire relevant, comprehensive, and easy to understand.
Abstract
Chronic lymphocytic leukaemia (CLL) is the most common form of leukaemia in adults in western countries. Asymptomatic patients are under clinical observation; when indication for treatment according to guidelines is met, treatment is initiated. When choosing from the numerous new treatment options, individual patient needs should be considered. To date, no instrument exists to capture these needs. The ePROM was developed based on the Patient Benefit Index (PBI) methodology which captures the importance of treatment goals as well as the achievement of these goals. The development considered the COSMIN guidelines and included semi-structured interviews with 28 patients with CLL and free-text questionnaires (n = 15). Data were analysed via qualitative content analysis according to Kuckartz. The PBI-CLL was finalised through an expert consensus and cognitive debriefing interviews with 14…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
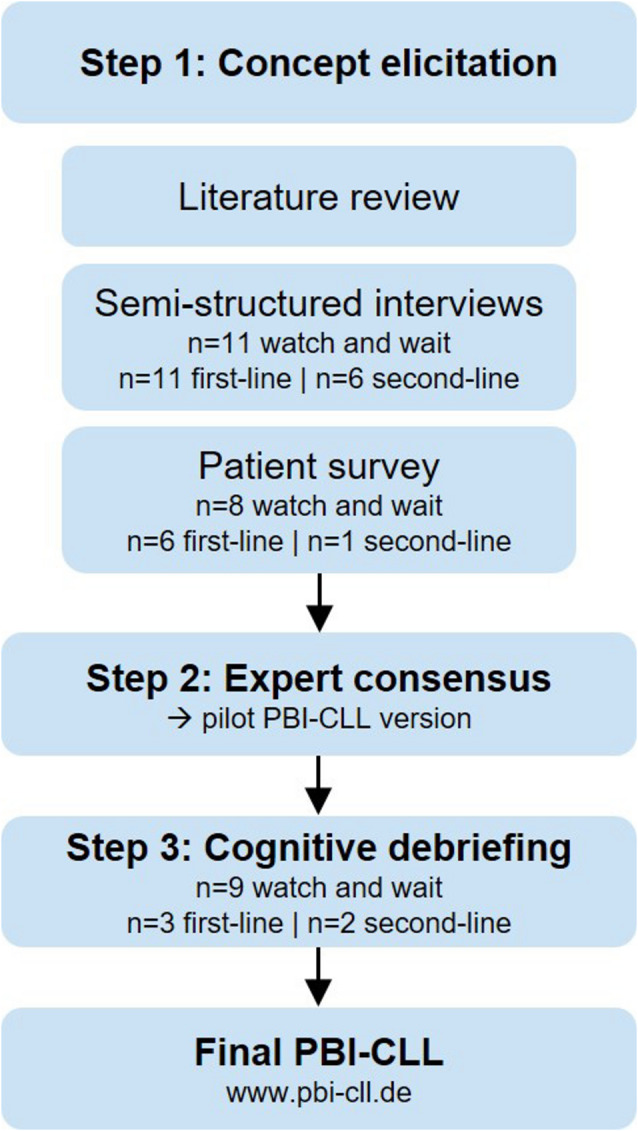 Figure 1
Figure 1- —Universitätsklinikum Hamburg-Eppendorf (UKE) (5411)
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsChronic Lymphocytic Leukemia Research
Introduction
Chronic lymphocytic leukaemia (CLL) is the most common type of leukaemia in adults in western countries with an incidence of 6 per 100,000 people in Germany; men are affected more often than women [1, 2]. Studies show that health-related quality of life (HRQoL) is severely affected [3]. Mean age at diagnosis is 72–73 years, however, due to increasing routine blood testing, the disease is now often found in younger years [1, 2, 4]. CLL develops through a clonal expansion of mature CD5 positive B-cells within blood, bone marrow, and lymphoid tissues [2]. Patients diagnosed at an asymptomatic, early stage are kept under clinical observation (watch and wait); once patients develop symptoms and/or show signs of bone marrow suppression, therapy is recommended [5, 6]. CLL affects people differently; some remain asymptomatic for a long time while others show quick progression and severe symptoms. For the decision on a specific therapy, different factors such as the cytogenetic and molecular genetic profile, comorbidities, comedication and treatment adherence need to be considered [2, 5]. Within the last decade, therapy options for CLL have developed rapidly [7]. With the emerging therapies such as small molecule inhibitors and monoclonal antibodies, chemoimmunotherapy is now rarely used; treatment duration varies between a fixed time period and continuous therapy [4, 5, 8].
Like the choice of therapy, treatment benefit is highly individual and does not only depend on effectiveness and treatment modalities but also on patient preferences and individual life situations [9]. The perceived benefit does not only consist of an improvement in QoL after the intervention but also on individual preferences and perceived causal attribution to the therapy [10]. Particularly regarding the increasing number of treatment options, assessment of individual patient preferences has become even more relevant [4, 11]. The patient-relevant benefit should be measured by a tool that reflects whether individual patient’s needs and expectations are fulfilled. As oncologists have been found to often misjudge patient goals, these can only be defined by the patients themselves [12]. A potential reason might be that patients and physicians have different priorities in the treatment of CLL [9, 13]. According to previous studies, patients base their treatment decision on its effectiveness and also on compatibility with their lifestyle; the demonstrated superiority is here less important than the patient’s perceived effectiveness [14]. Additionally, priorities in the treatment do not only depend on the impact the disease has, but also on personal preferences which differ between patients [15].
To include the patient’s perspective, patient-reported outcome measures (PROMs) are increasingly used in evaluating therapies [16]. To our knowledge, no instrument that measures treatment goals and benefit in CLL exists. Existing PROMs measuring HRQoL in CLL such as the QLQ-CLL17 [17] and cancer generic instruments such as the EORTC QLQ-C30 [18] or FACT-G [19], measure impairment at one point in time but neither assess the personal benefit of the chosen therapy nor include patients’ individual preferences [20, 21].
To close this gap, this study aimed to develop a new PROM measuring patient needs and benefits in CLL. Its structure will be based on the established Patient Benefit Index (PBI) methodology which assesses the subjectively perceived treatment benefit through reaching therapy goals. The first part of the PBI, the Patient Needs Questionnaire, assesses the importance of different treatment benefits for the patient. The second part, the Patient Benefit Questionnaire, assesses the achievement of these goals. A weighted global score quantifies the overall patient-relevant benefit [22]. PBI versions have been developed and validated for various indications such as multiple sclerosis [23], psoriasis [24], allergic rhinitis [25], and peripheral artery occlusive disease [26] and the tool has been used successfully in health care and clinical research [27–30].
The PBI for CLL (PBI-CLL) shall measure the importance and achievement of therapy goals regarding treatment outcome and treatment process. It will therefore include both a PROM and a patient-reported experience measure (PREM). It shall be applicable to all patient groups, including patients under clinical observation and patients who already receive treatment.
Methods
This non-interventional methods development study followed the COnsensus-based Standards for the selection of health Measurement INstruments (COSMIN) [31].
Step 1: Concept elicitation
To develop CLL-specific treatment goal items, we conducted a literature review, followed by qualitative interviews and a free-text survey (Fig. 1).
Fig. 1. Flowchart concept elicitation
Literature review
A non-systematic literature review provided an overview on existing instruments, related constructs, and tools. It also explored topics relevant regarding CLL patient’s therapy goals. It was conducted in November 2022 on PubMed/Medline. Search terms included but were not limited to “chronic lymphocytic leukaemia”, “patient needs”, “patient preferences”, “treatment goals”, “instruments”, “evaluation”, “questionnaire”, “index”, “scale”, “tool”, “survey”. Two researchers (BH, student assistant) scanned titles and abstracts to find relevant publications and screened the reference lists of the relevant papers.
Data collection
Based on the literature research and previous PBI development studies [20–23; 33], an interview guideline for qualitative semi-structured interviews with patients (Supplement 1) was developed in consultation with oncologists; it was pilot-tested with a CLL patient. All interviews were conducted by a public health professional (BH) experienced in qualitative interviewing. Throughout the study, minor changes were made to the interview guideline after discussions with an experienced PRO researcher (CB). Patients and recruiting practices were compensated with 30 Euros per interview. The interviews took place from February until August 2023 via phone or Zoom, according to patient preference.
Additionally, a free-text survey questionnaire was completed by patients. It included questions regarding treatment goals and burden, similar to the interview guideline (Supplement 2).
Data analysis
All interviews were audio recorded, transcribed verbatim, and pseudonymised. All hand-written questionnaires were typed into Microsoft Word. Through qualitative content analysis according to Kuckartz [32], data was categorised in the software MAXQDA [33]. The analysis process included identifying all text passages relevant to the research question and then applying thematic codes on potential treatment goals, thereby iteratively developing a hierarchical coding system. Using the interview guideline as a basis for categories, we categorised data into “goals/wishes” of different aspects: general (e.g. physical and mental/emotional), provider-related (e.g. provision of information, involvement in therapy decisions and positive attitude), related to the treatment process (e.g. administrative aspects, circumstances of application), and related to the therapy (e.g. acceptance of side effects and improved performance/fitness). These categories were then, if relevant, broken up into the third hierarchy level, e.g. with “waiting time” and “same doctor throughout” grouped under “administrative aspects”. Eight interviews and all 15 questionnaires were coded independently by two researchers (BH and JR), then comparing and consenting the results with feedback given by CB. Throughout this process, all codes were reviewed and refined by all three researchers, e.g. by adding a third sub-category “fears about the future” to the category mental/emotional burden. The number of new codes per interview and per survey was documented with a saturation table; the recruitment of new study participants was ended when the saturation table showed no or only minor new codes reflecting patient needs or burden.
Step 2: Expert consensus
Based on the coding system, an item pool was generated. An expert panel consisting of haematologists, PROM experts and patient representatives developed a first draft of the PBI-CLL. Clinicians received a reimbursement of 100 Euros for their participation, patients 30 Euros.
Step 3: Cognitive debriefing
The PBI-CLL draft version was transferred into digital format (www.pbi-cll.de).
It was tested in cognitive debriefing interviews with CLL patients conducted via Zoom, unless the patient preferred to be interviewed by telephone, in which case they were sent the PBI-CLL on paper. The Think Aloud Method was used: patients were asked to fill in the questionnaire while expressing their thoughts verbally. Patients were asked about comprehensiveness (including completeness of all key concepts), comprehensibility (their ability to read and understand items, instructions, and response options), and relevance of each item (including appropriateness of recall period and response options). The interviews were conducted by a researcher experienced in qualitative interviewing (BH) using an interview guideline (Supplement 3). Minor changes of the interview guideline were made throughout the interview conduction, based on discussion between BH and CB.
All interviews were audio-recorded and transcribed verbatim. The data was analysed based on content analysis by Kuckartz (see described above). After rounds of 4–5 interviews, the PBI-CLL was revised. Interviews were conducted until no further need for changes was found for two consecutive interviews.
In all study phases, inclusion criteria were a diagnosis with CLL, being aged 18 years or older, and being fluent in the German language. Patients were recruited through patient advocacy groups, social media, oncological practices, and a specialised CLL consultation hour; the response rate was not systematically documented.
The study was reviewed and approved by the Ethics Commission of the UKE Psychosocial Center (LPEK-0570). All patients participating in the study provided written informed consent.
Results
Patient characteristics
A total of 57 patients were included. Patients were heterogeneous regarding gender, age, and disease status (Table 1).
Table 1. Patient characteristics of study participantsInterviews(n = 28)Survey(n = 15)Cognitive debriefing(n = 14)n (%) / Mean (Range)Age (years)64.4 (44–86)65.3 (42–82)64.1 (52–83) Gender FemaleMale11 (39%)17 (61%)5 (33%)10 (67%)8 (57%)6 (43%) Highest school education Higher education (12 or 13 years)Middle school (10 years)General education (9 years)Not stated16 (57%)9 (32%)3 (11%)0 (0%)9 (60%)2 (13%)3 (20%)1 (7%)9 (64%)4 (29%)1 (7%)0 (0%) Living situation AloneWith spouse/partner/family6 (21%)22 (79%)3 (20%)12 (80%)2 (14%)12 (86%)Distance to oncologist (km)22.8 (1–220)25.0 (2–90)24.5 (2–120) Disease status Watch and waitFirst-lineSecond-line11 (39%)11 (39%)6 (21%)8 (53%)6 (40%)1 (7%)9 (64%)3 (21%)2 (14%)Time since diagnosis (years)7.4 (0.3–28)3.9 (0.1–15)7.4 (1–15) Treatment setting Practice [niedergelassen]Hospital outpatient clinic [Klinikambulanz]University hospitalNot stated11 (39%)3 (11%)14 (50%)0 (0%)3 (20%)3 (20%)8 (53%)1 (7%)9 (64%)1 (7%)4 (29%)0 (0%) Interview setting ZoomPhone13 (46%)15 (54%)7 (50%)7 (50%)
Step 1: Concept elicitation
The literature review confirmed that no tools to measure treatment goals and benefits in CLL exist. Therefore, the results of the literature review are not described in further detail; however, we used the results as a basis for prompts included in the interview guide, that is, topics to be addressed only if not reported spontaneously by the patient (e.g., application route; duration of recurrence-free period).
Through qualitative content analysis of the interviews and surveys, a category system with four categories and up to three hierarchy levels was developed: the first category covered outcome-related therapy goals and burden; the second covered provider-related goals and wishes (regarding doctors or other health workers); the third covered treatment-process-related goals and wishes. The fourth category covered general wishes regarding the therapy.
Outcomes-related treatment goals and burden
In this category, the physical impact of the disease and/or treatment was the most mentioned aspect. Many patients reported tiredness, exhaustion, and fatigue: “I also notice that I get exhausted quickly,* that I get tired quickly. […] You have to rest more quickly. You’re no longer so productive*” (I05). The B symptoms of CLL (fever, night sweats, weight loss) were also mentioned by many patients: “What I also had,* which is one of the B symptoms*,* is night sweat. […] And in the beginning*,* I even had some fever episodes”* (I22). Other physical impacts were breathlessness, heart problems, sleep disruptions, and polyneuropathies. Many patients could not say with certainty whether symptoms were caused by the CLL itself or by the therapy. Some had been living with the disease for many years and believed that some physical impairments were increasing due to their age. However, there were also patients who reported no or only very light physical impairments due to the CLL.
Another category was the mental impact due to CLL. Some patients reported fears about their future: “I’m always thinking about when it will get worse and how I will be able to cope with it” (S02). Others felt a mental burden due to the CLL; this included both patients in the watch and wait phase and patients who received treatment: “So far it’s only in my head. You think about the fact that you’re carrying around a serious illness. And the watch and wait is of course also something that gives you cause for thought.” (I26) “The psychological burden is very great. Because you’re constantly reminded of it. When I’m sitting at dinner with my wife and then something comes up,* an infusion and then I have [to take] tablets*,* side effects*,* then I’m reminded of the CLL. Or when the fatigue becomes worse*,* I say: That damn illness*” (I19). Some patients said they do not feel any or only a very small impact on their mental health, particularly patients in the watch and wait phase: “It’s been going on for eight years now and I’ve been living very well with it for all eight years. And I hope it goes on like this for a few more years” (I13).
Impacts on social life and relationships was mentioned by several patients. Some talked about reducing their social activities or avoiding crowds of people and the negative impact that the disease had on their social contacts: “I don’t go anywhere where lots of people gather. And if that happens,* then I put a mask on. […] That restricts you. […] Because you’re afraid that it will get bad*.” (I19). Several patients did not feel any impact on their social life: “Overall,* you can say that the social environment or social contacts do not change much*” (I24).
Further categories covered the influence of the disease on everyday life and leisure time: “Holiday travels only possible to a limited extent. Limited sports activity” (S04). Some patients reported having to reduce their work hours or volunteer work or that they “had to stop working because of the illness” (I07). Few patients felt financially impacted due to the CLL. Many hoped that through treatment, they could continue to live their life without any changes or impacts: “My goal is of course to have as much normality as possible” (I02).
Provider-related treatment goals and wishes
Patients mentioned the aspect of receiving information regarding their disease and the treatment. Some were hoping for information already when they first received their diagnosis, others also mentioned hoping to receive information regarding possible therapies early on: “What if… I needed treatment? What if? How does that work? I am a person who needs a bit of a handrail,* a guideline*” (I01). Most patients wanted extensive information regarding their disease in general and regarding the therapy once indication for treatment is given. Few said they did not want to receive a lot of information as they trusted their physician and would feel overwhelmed with information: “But I’m not a doctor and he is known to be a good oncologist; if he thinks that would be good for me now,* then I say: Yes*,* fine*,* then we’ll do it*” (I09). Many patients also described finding information online, through forums or self-help groups.
Patients wished for a collaboration of the physicians involved in their treatment. Empathy and a trusting relationship to the doctor were important to many patients. Patients wanted to be involved in treatment decisions and wished to be taken seriously and have a relationship on an equal footing: “I find that important,* my opinion and my assessment are really accepted and taken seriously [by the new doctor]”* (I22). Lastly, patients wished for their physician to have extended knowledge regarding therapy options and to be well-informed and hoped for a positive attitude if they chose to get a second opinion.
Treatment process-related goals and wishes
Within this category, administrative aspects regarding the treatment were discussed. Some patients wished to always be treated by the same doctor, particularly in university hospitals. Others mentioned that they would appreciate appointments as rarely as possible and with short waiting times. Patients also mentioned they want good availability of the practice / clinic via phone or e-mail.
Furthermore, the circumstances regarding treatment application were important to some patients. Most patients preferred oral therapy over infusion, as it makes the treatment easier for them and they do not need to travel to their physician for treatment: “I’d rather,* because I can do it at home… I’d rather take tablets. […] Because of the [previous] infusions*,* I am completely bruised*,* I mean*,* my veins are*” (I14). While some patients wished for a break in their treatment if the clinical parameters improved, others did not mind their continuous therapy without any breaks: “Of course it would be nice to pause [the treatment],* but the treatment doesn’t restrict me at all*” (25).
General wishes regarding the therapy
This category included different general wishes regarding therapy, forming the basis for module 3 of the PBI-CLL which will provide a quick overview of what is important to the patient before a consultation. The preferences mentioned in this category were very heterogeneous. For example, some patients were willing to accept more severe side effects if this implied higher effectiveness of the treatment: “Rather higher side effects at the beginning and a better cure. You can’t really speak of a cure for CLL” (I10). Others wanted a treatment with as little side effects as possible: “With the chemo it was very important that I had little side effects. […] So I was given a really mild mixture“ (I03).
While some participants hoped to remain in the watch and wait phase for as long as possible, others preferred to receive treatment early on, hoping to increase the chances of remaining symptom-free: “If there is a diagnosis,* why don’t you start relatively early a light […] or well-tolerated therapy? Why? Why do you wait until it has escalated?*” (I01).
Lastly, some patients preferred newer, innovative therapies while others wanted a tried and tested therapy. However, most patients mentioned that they want to avoid chemotherapy, mostly because they were scared about its side-effects: “Without really knowing it,* but you have images in your head or hearsay about what they can do to you or that they are quite stressful and so I have always avoided or still want to avoid that*” (I25).
For the full code system, see Supplement 4.
Based on the above-described categories, an item pool was developed by BH, CB and JR.
Step 2: Expert consensus
The item pool was examined by the expert panel in two rounds: in the first round, the item pool was discussed with a haemato-oncologist (JvT) and a patient with CLL; for organisational reasons, in the second round, the researchers included a further haemato-oncologist (MJV) in the discussion of the item pool.
A consensus was found on the content and structure of the questionnaire. The panel agreed on using the same response scale as in the original PBI version; for module three, the content of the questions as well as a bipolar format were agreed upon.
After the meetings, two researchers (BH, CB) made some additional small alterations (order of the items, phrasing, and grammar of items) and the expert panel confirmed the draft version of the questionnaire before the following study phase.
Step 3: Cognitive debriefing
Fourteen cognitive debriefing interviews, separated in three rounds, were conducted. In the first round, some patients mentioned unclarities regarding individual items. For example, multiple patients missed the symptom fatigue and did not think it was covered by the item on physical impairment; therefore, we added fatigue as a separate item. Additionally, some items were summarised, and the order of items was changed to increase comprehensibility. In the second round, only minor changes regarding the wording of individual items were made. In the third and last round, the final version of the questionnaire was tested with patients with no need for additional revisions found.
We found that most patients answered many items of the Patient Needs Questionnaire at the upper end of the scale; however, this cannot be quantified as interviewees’ responses to the PBI-CLL were not documented.
Overall, patients found the questionnaire to be relevant and easy to understand: “The questions were all understandable. They were very well phrased. And are basically understandable for everyone” (CD13).
The final version of the questionnaire was uploaded to the website www.pbi-cll.de and can be found in Supplement 5. Table 2 provides an example quote from the content elicitation interviews or the written survey for each treatment goal item to show how items were formed.
The original questionnaire was developed in German: For the process of translation into UK English, we followed the COSMIN guidelines [34]: Firstly, the questionnaire was translated to English separately by two translators and then back to German by two further translators; all persons involved were professional translators from the translation agency lingoking, were mother tongue speakers in the target or source language, respectively, were naïve on the construct measured by the PROM and worked independently from each other. In an online conference with both forward translators and the questionnaire developers, the differences in the translations were discussed and a consensus was found to ensure comparability between the German and English version. The preliminary version was checked by an additional translator and when finalised, discussed with the study team. The process of translation was documented separately.
Table 2PBI-CLL treatment goal items (Patient Needs Questionnaire) and patient quotesItem No.Treatment goal item(How important is it to you…)Patient quotes from content elicitation interviewPatient ID Module 1: Importance of Treatment Outcomes 1… that the therapy reduces or prevents fatigue (exhaustion and chronic tiredness)?“(…) the worst thing is the tiredness, which really affects you quite a bit. You sleep ten hours at night and can still sleep for two hours during the day. That’s very intense.”I242… that the therapy reduces or prevents the physical effects of CLL?“Regaining my stamina as much as possible. Running/ cycling/ strength (muscle building) sport in a group has always been important to me!”S013… that the therapy helps make your CLL less visible?“The symptom that the bones became thicker and thicker, that of course really bothered me, it no longer looked nice, I’ve occasionally been asked about it, and in that respect, it really bothered me”I254… that the treatment is not time-consuming?“Well, I mean, back then with the chemotherapy, of course. You’re tied down for six months. You have to go every four weeks. That was quite disruptive. Because depending on whether the blood count wasn’t right, you had to extend [the treatment] by another week.”I155… that the therapy disrupts your daily routine as little as possible?“Of course it’s annoying that you always have the clock in your head because the medication has to be taken every day at the same time if possible, but I’d say that measured against what the medication does, I manage very well. Of course, I would prefer to take it once a year and then it would be just as good and, of course, it would be less effort, but that’s a bit unrealistic.”I256… that the therapy you receive impairs your immune system as little as possible?“During therapy, of course, you are simply weaker, more fragile and of course more vulnerable. You have to be even more careful.”I077… that the therapy is individually tailored to your comorbidities?“And people often forget that I have several diagnoses. And that’s perhaps why my overall condition isn’t so good.”I238… that the treatment helps you continue leading your life as before the diagnosis?“I personally don’t define it in such a way that the goal is to reach 90 and then not really be able to live on it for the last 20 years, because for me, living is really a lot, working and sport and family, of course. That’s actually my thing. And I just want to keep that going for as long as possible. That’s actually the goal.”I029… that the treatment enables you to continue your working life with fewer limitations?“Well, it’s a burden insofar as I’ve already mentioned that I’m self-employed. And of course, if something happens now, I wouldn’t be able to take longer sick leave. Although, of course, I can take longer sick leave, but then I won’t earn anything. (…)”I2210… that the treatment enables you to enjoy a normal everyday life and leisure activities?“I would like to, so I really enjoy travelling with my wife. Of course, I would like to do that again. For example, I don’t dare to travel long distances at the moment. At the moment, I wouldn’t travel further away from home than Europe so that I can get back within 24 h or come back in case I get worse.”I2411… that the treatment enables you to enjoy a normal social life?“What I don’t do now, I have to say quite clearly, I try to organise my holidays or free time in such a way that I meet as few people as possible. (…) People who have cancer and those around them know that they have cancer; that is very strange. They behave very differently to how they used to. They’re afraid to talk to you, to talk about this illness at all, because they’re afraid that they might embarrass themselves or that you might take offence or/ I don’t know. But we’ve noticed that it’s actually like a shield around you.“I1912… that the treatment enables you to have a normal family life?“[My] children are more worried than I am. That’s probably the case, you can’t really prevent it either. And yes, cancer is actually very common in our family, I’d say. And of course the children end up worrying about how their father is doing and then it doesn’t help saying that I’m fine, because the family is just very worried.”I2613… that the treatment makes you less anxious about a relapse?“And I still can’t quite believe that it’s really gone. That it won’t come back. In other words, I’m thinking that it might come back somehow. And that’s a bit of a worry, what will happen then? What will follow? Are there any options or are there only bad treatment options that restrict you more than they do now?”I2114… that the treatment makes you less anxious about the future?“But of course it’s not nice to know that you have two types of cancer, yes, which COULD get worse and worse. The theory is just bad. And that’s why there are so many appointments. It’s not always fun when you have to go there regularly every three months, every six months, whatever, and have to go for a check-up, isn’t it? And, of course, you always expect the worst. You always expect the sentence: Oh [own name], now it’s got a lot worse. And that’s not nice, of course. You get phases here where you really… see the dark side of it.”I2315… that the treatment means you think less about your CLL?“Sometimes it gets more difficult, depending on where you come from/you always check the forums, what news are there? And then you read about the progress in the quiet phases or in the dark times that we’ve just had in the case, that’s when it sometimes gets more difficult. Then you think: Oh gosh, that really shouldn’t have happened.”I0116… that the treatment helps you feel less depressed?“Psychological is simply the strongest. Well, that’s what I heard at the beginning: You’ll live another 2 years, another 5 years. Then that was… in the end more of a kind of death administration. Looking back, then. I stopped doing a lot of things because I thought there was no sense in it anyway. Why should I still do it? It was already limiting me mentally. […] But… when I look back on my life, it’s rather disappointing. That I didn’t do a lot of things because of the diagnosis. That’s… well, that’s what burdens you the most. […]”I0317… that the treatment makes you less anxious about side effects?“So with the chemo it was very important that I had few side effects. You read so often about oral mucositis and fatigue, that the body is being killed. I didn’t want any of that. (…) That was my goal. Gentle prolongation of life. And the leucocytes and all the blood values were back to normal after these 30 chemos. So I was out of the terminal stage, but in a super gentle way, I have to say. And I would have liked the same with the new drugs. I think the most important thing with CLL is to be gentle and maintain quality of life. I think that’s incredibly important.”I0318… that there is a minimal financial burden associated with CLL and the treatment?“It’s a collapse / I mean, I’ve never been anyone / I’m not a millionaire. But I’ve always worked normally and had my salary. And I could afford my two-bedroom flat, my car and all that. And now there’s nothing left, right? (…) It’s also a financial collapse, this whole medical history. It’s also a burden/it’s very stressful.”I23 Module 2: Importance of process quality 1… to be given explanations and information about CLL, the course of this condition, and the therapeutic options available?“The important thing is how well you get it explained, what you have, what you can expect.”I072… to be given comprehensive information at the time of initial diagnosis?“I simply believe that the diagnosis in the initial consultation is the decisive key or decisive criterion, let’s say, for how the patient deals with the issue in the first stage. It doesn’t matter what it looks like in the individual case, but simply, let’s say, to see the silver lining or the ray of sunshine on the horizon somewhere: Yes, this is what you have. You’re at this stage. We do this and that. If you’re at a different stage, we’ll start therapy here and there. But you’re in good hands with us.“I013… to be provided with brochures or written information when you receive your initial diagnosis?“So at the beginning I simply had no information at all. It was just bad. When I saw the second doctor at the clinic, for example, there were brochures. There were brochures from the German Cancer Aid, which I think would have been great if I’d gone there from the start or if the first doctor had given them to me.”I064… to be given an additional appointment soon after your initial diagnosis to provide you with further information, e.g., from trained practice staff?“And then I would like to be given a telephone number. That you can call again, say, three or four days later. Because it’s/you’re just sitting there in the doctor’s room. You get that. And if, as I said, you’re then also told: It’s not bad. And thousands of people have it and so on. You don’t want to hear that. And you don’t believe it either. Because if I have cancer, I have cancer and cancer still has a bad aftertaste. (…) I’m always talking and doing and doing, so that you can just ask again afterwards. (…) That can also be a doctor’s assistant.”I155… to receive information about future therapeutic options as early as possible?“Well, to be relatively well informed, right? What are the options, what are the chances, what exactly are the treatment options if the time comes? In any case. I think the doctors always hold back a bit at first, if it doesn’t come to a therapy, which is also normal so as not to fuel the fears.”I056… to receive information about support groups?“[…] I mean well, of course the doctors also do a lot to refer people to self-help groups. (…) I mean, with us, I’m lucky, it’s also relatively easy in [city 1]. But for me, it’s important when someone calls, when he has his diagnosis and before he takes Valium and all sorts of things, it’s much better if you talk from one patient to the other”I157… to receive information about rehabilitation options or residential treatment at a medical spa?“[…] although there is no cure, it’s important to me that I can perhaps do some kind of rehabilitation again, and I’ve already enquired about that. (…) just to leave everything here completely. And maybe go to rehab for two or three weeks. I’d like to do that too, maybe with my son. I still have to think about that, clarify whether that’s possible. And yes, that’s something that rounds off the therapy quite well for me.”I188… to be given information about the psychological support options, including for relatives if necessary?“I then also had psycho-oncological support. And that also helped me a lot. I thought that was very good. I also had to stop working because of the illness. And that psycho-oncologist was of course a great help, because I was very reluctant to stop working. And that was somehow very helpful.”I079… that your doctor is up-to-date with the latest research?“I want to be with a doctor who I know is up to date and can explain the therapy to me and also suggest alternatives and explain all the options with advantages and disadvantages so that I have the feeling that I am in really good hands.”I0610… that the doctors involved in your treatment communicate with each other?“Exactly, so he’s a haematologist and he’s also directly in the clinic. So he has his practice in the clinic, so to speak, and of course the short distances and the short communication with various examinations and so on, that’s relatively quick, yes, and of course that makes/is a big advantage. And the exchange with all his colleagues in oncology and so on. Of course, everything goes hand in hand.”I1611… that the doctor treating you has a positive attitude towards obtaining a second opinion?“I have to say that I also think it’s very, very positive that my haematologist took care of the appointment, that she forwarded all the documents to the university hospital. And, as I said, I got the call today within a week. That / or no, actually, I was there yesterday and the university hospital called me today. So that worked out really well, didn’t it? I also think my doctor/ I also said here, if we were to start anything, that I would definitely like to get a second opinion. And then she says: No, no, definitely. That’s not an issue. We’ll do that too.”I0512… that your doctor presents information clearly and in a way that is easy to understand?“For example, why don’t doctors say, well I don’t know if it’s the same everywhere: if you have CLL, it’s not curable. That word has never been used. But it’s true. CLL IS NOT CURABLE. Why don’t doctors tell you that?”I1913… that your doctor talks to you as an equal?“I think a (…) doctor-patient relationship like that has to be somewhere on an equal footing. I would find it difficult (…) if I had the feeling that my doctors were saying: She doesn’t understand what we’re explaining to her anyway. That’s why we only explain it to her in very broad terms. But I think that’s also the case today / because everyone does research on the internet and has read so much. I think it’s now the case that patients are given really comprehensive information. Which was also important to me at some point, but that has a bit to do with my personal history and my environment.”I0714… that your doctor and healthcare staff are empathetic?“Of course empathy is always important. That’s a very important topic.”I0715… that your doctor takes time for you?“Yes, the important thing for me in any case was that the oncologist took his time. And he did. So there is such a / not that he says: You have CLL. Yes (incomprehensible), goodbye. No, he did: Do you have any questions?”I1016… to have a good trust-based relationship with your doctor?“The important thing in treatment is to have a doctor you trust. And I always say that in our (self-help) group, many people write: I have a good oncologist. Then I say to them: How do you know that your oncologist is good? You don’t know anything about your illness, but you say your oncologist is good because he talks to you well, but you don’t know if that’s right. But I know with my doctors that I am/ that I am in good hands/ you have to feel that you are in good hands. You have to feel well looked after at the doctor’s/ and I know exactly which doctors I go to.”I0117… to always be treated by the same doctor?“Then I also went to the university hospital in [city 1], as I live in [city 1]. But I’m a statutory health insurance patient. So I realised that I would only have assistant (doctors) sitting in front of me. (…) They are at the cutting edge of research. Basically, I don’t have a problem with that, but you sit in front of someone different every time and I thought it would be better to have a specific contact person for a disease.”I2218… that waiting times at the practice or clinic are as short as possible?“You have long waiting times until you get an appointment. […] Always again, you wait four, five hours. But that is my time, that I don’t feel I have. Time is precious when you have CLL.”I0319… that the practice or clinic is well organised?“So what I would like to see is the complete laboratory results, the blood count tests, if you could always get them straight away or if they were available in full. Of course, that’s not really possible in terms of the procedure. (…) I would like to have all the data, also the attending physician to have all the data on the table. That you could also talk about it completely at the appointment, that would be something organisationally administrative that comes to mind. Something that could perhaps be improved.”I2620… that the practice or clinic is easy to contact by email or telephone?“That’s great, of course. So if you can just write a quick email and get a quick reply. Or you can also call. That’s great for me in terms of accessibility. Yes, that’s actually the most important thing.”I0221… how your medication is administered (e.g. tablets or drip)?“Of course, if you tolerate it well, it’s always easier to take tablets… than this infusion. Infusions are now a big problem for me because my veins are so bad.”I0722… where the medication is administered (i.e. at home or in the hospital/medical practice)?“So if I/if the therapy was to start now, I would do it first, if I was to get an infusion or something else, as I have been told, I would definitely not want to do it at home. I will do it/ like the first therapy, I will go to hospital. I know that. Because I have a contact person there. And there I am… on site. And I don’t want to sit here at home and say to my husband: I’m not feeling well. (…)”I1123… that if you take tablets, you only need to take them as infrequently as possible?“Otherwise, if I could choose between two therapies, let’s assume that one therapy would mean I would have to take tablets five times a day and the other only once, I would naturally tend towards the one with one tablet if they are equally safe. If, of course, the tablet therapy with the five tablets a day, which is what the research says, is much, responds much better, much longer in terms of experience, I would of course do that too.“I0624… that the doctor will consider the possibility of pausing the therapy if your values have improved?“I wouldn’t take a break. So it’s all right. You never know what will happen if you stop taking it for longer. (…) I’m a bit afraid that it will get worse again. I’m so glad that everything is going so well.”I1425… that you and your doctor reach decisions about the best treatment plan together?“Secondly, that I am included in the treatment. So, of course, many doctors already know that I, I mean it came, it is the case that I have a self-help group in [city 1] and of course they already knew that I argue differently, or rather, how should I describe it? I just want to be totally involved. I want to know everything. I want to know how long the treatment will last and so on. It is extremely important to me that I am properly involved as a partner.”I1526… to receive detailed information about the treatment and its side effects at the start of treatment?“Yes, that I get properly informed about the, about the treatment options. And about the consequences of the various treatments and yes. Apart from that, that you can also talk about side effects. And that there are also solutions offered in that aspect.”I21Patient IDs starting with I: qualitative interviews; patient IDs starting with S: written survey
Discussion
This study aimed to develop an electronic PROM that assesses treatment needs and benefits in adult patients with CLL.
Throughout the data collection, we included patients in the watch and wait phase as well as patients receiving treatment; the patient characteristics of participants also reflect the target population regarding age and gender [1, 2]. This supports the applicability across patient groups.
The data showed that patients have numerous therapy goals and report disease burden in different areas of their lives. While the physical impact of the disease and the treatment has a large effect on patients, also mental or psychological effects were reported by both watch and wait patients and patients undergoing treatment. Regarding the providers, patients mostly wished for empathic physicians, but found the expertise and knowledge of their provider even more important. Overall, most patients wanted normality in their lives: they hoped that the CLL or the therapy will not impact their lives and that a therapy will help to increase their life expectancy.
The cognitive debriefing interviews showed that participants found the PBI-CLL easy to use. They did not report difficulties completing the questionnaire in neither the electronic nor the paper-based version of the instrument (provided to patients who preferred to be interviewed over the phone). However, during the cognitive debriefing interviews, most patients answered a lot of needs items on the upper end of the scale, indicating a potential ceiling effect. Terwee and colleagues state that floor or ceiling effects may indicate limited content validity as patients in the lower and upper scores cannot be distinguished from each other [35]. However, most cognitive debriefing participants indicated that they would not prefer the response options to be expanded. For this reason, and because there were some patients who replied in the lower end of the Likert scale, we decided not to change the scale to ensure that replies on the lower end of the scale are also reflected in the questionnaire’s scores. Furthermore, the ceiling effect shows that most patients found the goals to be of high importance and that the included items and therefore the therapy goals are indeed highly relevant for patients. In previous PBI developments, floor and ceiling effects were rather low [36], however, as this effect was found in the cognitive debriefing, our sample included only 14 patients compared to validation studies of other PBI versions. If a ceiling effect will be confirmed in a follow-up validation study, and assuming that it indicates that many outcomes are indeed of maximal importance for many patients, this will imply that determining an unweighted rather than a weighted global score might be sufficient to quantify patient benefit. In clinical practice, many high-importance scores suggest that needs should be discussed broadly; few high-importance scores suggest that discussion can be focused on specific areas. The validation study should also test the psychometric characteristics such as reliability, convergent validity, and responsiveness in a longitudinal design with a larger patient sample.
We expect that the PBI-CLL can be used in clinical practice as a basis for a discussion about therapy options and goals. It could provide the oncologist with a quick overview of what is important to patients; specific goals and wishes might be addressed more targeted. Therefore, the tool may save time during patient consultations. Additionally, it may increase satisfaction of patients who are included into treatment decisions and could indicate what is important to them. By using the PBI-CLL, oncologists will be able to assess better which information patients need and improve the quality of care as well as the patient satisfaction. These assumptions need to be tested in subsequent studies. The PBI-CLL can also be used to compare different therapies by comparing the mean scores for the therapies; this way, differences in the patient-reported benefit from interventions can be pointed out.
The PBI-CLL data collection could be a challenge in clinical routine, as it will need to be integrated into existing data structures, with patients completing the questionnaire online before their visit or on a tablet while waiting. In some cases, it may be more feasible to use the paper version. Consideration should also be given to timing (e.g. first visit after diagnosis; before deciding on (new) treatment) and access to the data if there are multiple providers per patient. It is also important to avoid not discussing patients’ responses in PBI-CLL, which can leave patients feeling unheard. In addition, incorporating the PBI-CLL assessment into clinic routines, deciding which modules to assess and when, and becoming familiar with its structure may require some initial effort, but this should be offset by the subsequent efficiency gains from structured assessment of patient needs and benefits. Once implemented, the PBI-CLL’s unified Likert response scale should make it easy to quickly understand the data.
Strengths and limitations
A major strength is the involvement of patients in the study: already during the development of the study protocol, we involved self-help groups. During the progress of the study, we received a lot of positive feedback from patients and patient representatives in that they felt heard by being able to participate in the development.
Due to the nature of the study which only included qualitative data, the results cannot be generalised; a quantitative validation study will be necessary to confirm psychometric characteristics. Conducting qualitative patient interviews also involves the risk of recall bias; however, including patients at different stages of their disease and/or therapy reduced and balanced this risk. Furthermore, in both the content elicitation and cognitive debriefing interviews, a small number of participants in the watch and wait phase reported having neither physical symptoms nor mental burden. These patients reported no therapy goals in the content elicitation and had difficulties filling in the PBI-CLL during the cognitive debriefing, as they found the therapy goals not to be relevant for them. This shows that, as expected, the goal achievement for module 1 (therapy outcomes) is not suited to patients in early watch and wait phase; they should only be asked to complete module 2 on process quality, and module 1 as soon as treatment is indicated. On the other hand, individual items that are not relevant to a patient do not pose a problem due to the “does not apply” response option.
Conclusion
This study provides an innovative electronic PROM that assesses treatment needs and benefits in patients with CLL, an indication for which only few PROMs exist. The instrument was developed according to the COSMIN standards and was seen as very positive by both patients and clinicians. It may help include patients into therapy decisions and provide a basis for a discussion of patient needs in patient-physician-consultations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Supplementary Material 1: Supplement 1. Interview guideline content elicitation
Supplementary Material 2: Supplement 2. Written survey content elicitation
Supplementary Material 3: Supplement 3. Interview guideline cognitive debriefing
Supplementary Material 4: Supplement 4. Overview of the code system
Supplementary Material 5: Supplement 5. Questionnaire PBI-CLL, UK English version
Supplementary Material 6
Supplementary Material 7
Supplementary Material 8
Supplementary Material 9
Supplementary Material 10
Supplementary Material 11
Supplementary Material 12
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Parikh SA, Gale RP, Kay NE (2020) Chronic lymphocytic leukemia in 2020: a surfeit of riches? Leukemia 34:1979–1983. 10.1038/s 41375-020-0852-710.1038/s 41375-020-0852-7PMC 813083932393844 · doi ↗ · pubmed ↗
- 2Schräder NHB, Korte EWH, Duipmans JC et al (2021) Identifying epidermolysis Bullosa patient needs and perceived treatment benefits: an explorative study using the patient benefit index. J Clin Med 10. 10.3390/jcm 1024583610.3390/jcm 10245836 PMC 870949334945131 · doi ↗ · pubmed ↗
- 3Mokkink LB, Prinsen C, Patrick DL, Alonso J, Bouter LM, De Vet H, Terwee CB (2019) (2019, 1–32) COSMIN Study Design checklist for Patient-reported outcome measurement instruments. https://www.cosmin.nl/wp-content/uploads/COSMIN-study-designing-checklist_final.pdf. Accessed 20 Aug 2024