Association of overactive bladder with all‐cause and cardiovascular mortality in women: A propensity‐matched NHANES study
Weipu Mao, Sagar Barge, Zhaobo Luo, Weiqun Yu

TL;DR
This study finds that overactive bladder in women is linked to higher all-cause and cardiovascular mortality, and metabolic markers like TyG-WHtR are strongly associated with the condition.
Contribution
The study identifies TyG-WHtR as the most effective metabolic index for predicting overactive bladder in women.
Findings
OAB is an independent risk factor for all-cause and cardiovascular mortality in women.
TyG-related indices show a positive association with OAB, with TyG-WHtR being the strongest predictor.
Higher TyG-WHtR values are linked to an increased risk of OAB.
Abstract
To examine the impact of overactive bladder (OAB) on all‐cause and cardiovascular mortality in women in a real‐world setting, and to examine the association of TyG‐related indices with OAB. Data on 6580 women aged ≥20 years were collected from the National Health and Nutrition Examination Survey (NHANES) database. Kaplan–Meier curves and Cox survival analysis were used to evaluate the association between OAB and all‐cause and cardiovascular mortality. Biomarkers for metabolic syndrome were assessed for their association with OAB, including triglyceride‐glucose (TyG) and TyG‐related indices. The association between TyG‐related indices and OAB was evaluated using restricted cubic splines (RCS), receiver operating characteristic (ROC) curves and multivariate logistic regression, with propensity score matching (PSM) employed to balance confounders between OAB and non‐OAB groups.…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
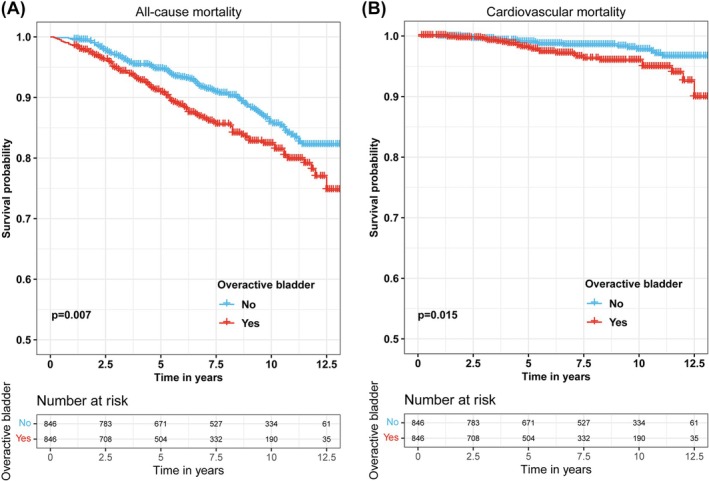 FIGURE 1
FIGURE 1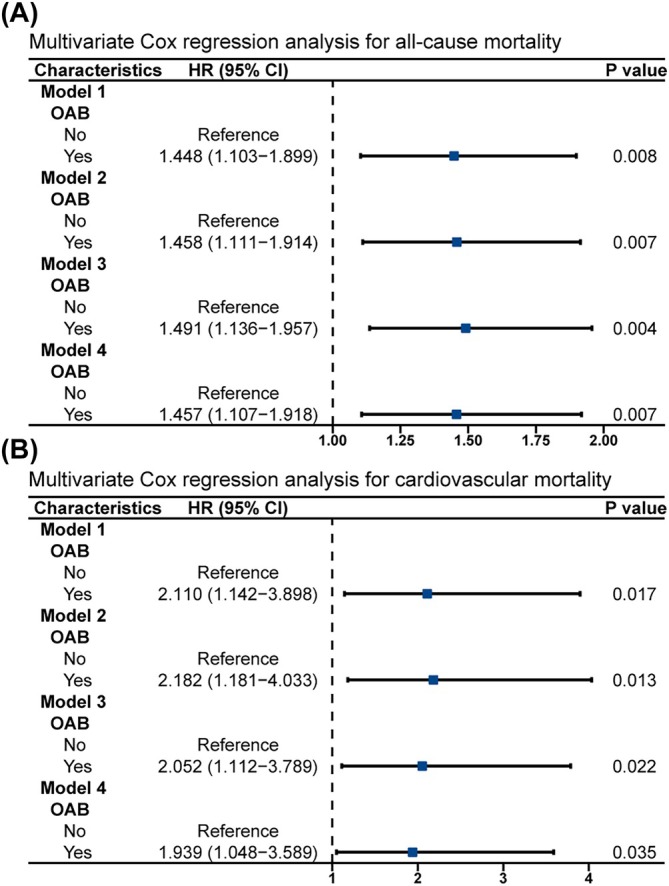 FIGURE 2
FIGURE 2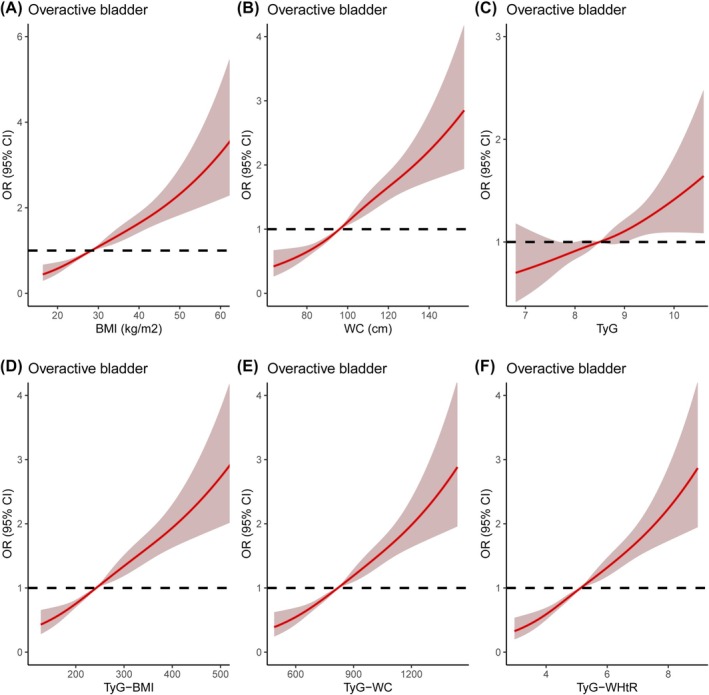 FIGURE 3
FIGURE 3| Characteristics | Total | Non‐overactive bladder | Overactive bladder |
|
|---|---|---|---|---|
| No. (%) | No. (%) | No. (%) | ||
| Total patients | 1692 | 846 (50.0) | 846 (50.0) | |
| Age, years | 0.992 | |||
| <40 | 344 (20.3) | 171 (20.2) | 173 (20.4) | |
| 40–60 | 560 (33.1) | 280 (33.1) | 280 (33.1) | |
| >60 | 788 (46.6) | 395 (46.7) | 393 (46.5) | |
| Race | 0.981 | |||
| Mexican American | 256 (15.1) | 127 (15.0) | 129 (15.2) | |
| Other Hispanic | 165 (9.8) | 81 (9.6) | 84 (9.9) | |
| Non‐Hispanic white | 773 (45.7) | 393 (46.5) | 380 (44.9) | |
| Non‐Hispanic black | 393 (23.2) | 193 (22.8) | 200 (23.6) | |
| Other | 105 (6.2) | 52 (6.1) | 53 (6.3) | |
| Education level | 0.952 | |||
| Less than high school | 477 (28.2) | 236 (27.9) | 241 (28.5) | |
| High school or equivalent | 350 (20.7) | 177 (20.9) | 173 (20.4) | |
| College or above | 865 (51.1) | 433 (51.2) | 432 (51.1) | |
| Marital status | 0.883 | |||
| Married | 713 (42.1) | 355 (42.0) | 358 (42.3) | |
| Unmarried | 979 (57.9) | 491 (58.0) | 488 (57.7) | |
| Hypertension | 0.846 | |||
| Yes | 802 (47.4) | 403 (47.6) | 399 (47.2) | |
| No | 890 (52.6) | 443 (52.4) | 447 (52.8) | |
| Diabetes | 0.846 | |||
| Yes | 211 (12.5) | 102 (12.1) | 109 (12.9) | |
| No | 1464 (86.5) | 736 (87.0) | 728 (86.1) | |
| Borderline | 17 (1.0) | 8 (0.9) | 9 (1.1) | |
| Alcohol consumption | 0.764 | |||
| Yes | 1040 (61.5) | 523 (61.8) | 517 (61.1) | |
| No | 652 (38.5) | 323 (38.2) | 329 (38.9) | |
| Smoking status | 0.979 | |||
| Never | 1130 (66.8) | 564 (66.7) | 566 (66.9) | |
| Former | 305 (18.0) | 152 (18.0) | 153 (18.1) | |
| Current | 257 (15.2) | 130 (15.4) | 127 (15.0) | |
| Vigorous work activity | 0.518 | |||
| Yes | 127 (7.5) | 67 (7.9) | 60 (7.1) | |
| No | 1565 (92.5) | 779 (92.1) | 786 (92.9) | |
| Moderate work activity | 0.643 | |||
| Yes | 386 (22.8) | 197 (23.3) | 189 (22.3) | |
| No | 1306 (77.2) | 649 (76.7) | 657 (77.7) | |
| Vigorous recreational activity | 0.766 | |||
| Yes | 109 (6.4) | 56 (6.6) | 53 (6.3) | |
| No | 1583 (93.6) | 790 (93.4) | 793 (93.7) | |
| Moderate recreational activity | 0.957 | |||
| Yes | 487 (28.8) | 244 (28.8) | 243 (28.7) | |
| No | 1205 (71.2) | 602 (71.2) | 603 (71.3) | |
| BMI (kg/m2) | 30.25 ± 7.35 | 29.17 ± 6.88 | 31.34 ± 7.64 | <0.001 |
| WC (cm) | 100.05 ± 16.23 | 97.66 ± 15.75 | 102.44 ± 16.36 | <0.001 |
| FBG (mg/dL) | 106.6 ± 29.9 | 105.4 ± 26.8 | 107.7 ± 32.8 | 0.114 |
| TG (mg/dL) | 116.4 ± 61.1 | 114.7 ± 58.9 | 118.2 ± 63.2 | 0.232 |
| HDL (mg/dL) | 59.42 ± 16.86 | 59.60 ± 17.07 | 59.23 ± 16.65 | 0.675 |
| LDL (mg/dL) | 115.3 ± 35.6 | 115.0 ± 35.0 | 115.5 ± 36.2 | 0.783 |
| TC (mg/dL) | 198.0 ± 40.8 | 197.5 ± 40.1 | 198.4 ± 41.6 | 0.676 |
| TyG | 8.58 ± 0.60 | 8.56 ± 0.60 | 8.60 ± 0.59 | 0.166 |
| TyG‐BMI | 260.4 ± 69.2 | 250.6 ± 65.5 | 270.3 ± 71.4 | <0.001 |
| TyG‐WC | 861.1 ± 166.9 | 838.9 ± 164.0 | 883.4 ± 167.0 | <0.001 |
| TyG‐WHtR | 5.39 ± 1.05 | 5.25 ± 1.04 | 5.54 ± 1.04 | <0.001 |
| Blood urea nitrogen (mg/dL) | 13.67 ± 6.62 | 13.37 ± 6.21 | 13.97 ± 7.00 | 0.066 |
| Blood creatinine (mg/dL) | 0.81 ± 0.39 | 0.80 ± 0.36 | 0.81 ± 0.42 | 0.545 |
| Uric acid (mg/dL) | 5.08 ± 1.35 | 5.08 ± 1.36 | 5.08 ± 1.34 | 0.938 |
| Characteristics | Before PSM | After PSM | ||
|---|---|---|---|---|
| HR (95% CI) |
| HRR (95% CI) |
| |
| All‐cause mortality | ||||
| OAB | ||||
| No | Reference | Reference | ||
| Yes | 1.414 (1.167–1.714) | <0.001 | 1.457 (1.107–1.918) | 0.007 |
| Cardiovascular mortality | ||||
| OAB | ||||
| No | Reference | Reference | ||
| Yes | 1.528 (1.026–2.274) | 0.037 | 1.939 (1.048–3.589) | 0.035 |
- —National Institute of Diabetes and Digestive and Kidney Diseases 10.13039/100000062
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsUrinary Bladder and Prostate Research · Pelvic floor disorders treatments · Urinary Tract Infections Management
INTRODUCTION
1
OAB is clinically characterized by urgency, increased frequency, nocturia and urinary incontinence.1 OAB afflicts over 17% of the US population2 and approximately 20.8% of the people in Asia.3 The prevalence of OAB varies by sex, with women being more likely to develop OAB than men. For example, OAB affects 10.8% of men and 12.8% of women in Europe and Canada.4 OAB significantly impacts the quality of life of patients, and severe OAB in female patients can serve as an independent risk factor for bone fractures.5, 6 However, the impact of OAB on overall survival has not yet been reported.
Many factors could contribute to OAB, such as infection, injuries, outlet obstruction and ageing. Among these, diabetes is the most common significant risk factor for OAB. Diabetes affects approximately 463 million people worldwide, and this number is expected to rise continuously to around 700 million by 2045.7, 8 Diabetes mellitus (DM) results in a range of complications,9 including the prevalent diabetic bladder dysfunction (DBD), which often accounts for 40%–100% of DM patients. DBD is characterized by symptoms of overactive bladder (OAB), particularly in the early stage of DM.
Insulin resistance (IR) is the cornerstone of type 2 diabetes, characterized by reduced insulin secretion or inadequate sensitivity to insulin. The gold standard for assessing IR is the hyperinsulinemic‐euglycemic glucose clamp test.10 However, its complexity, time consumption and high cost prevent its wide implementation. Because IR leads to metabolic syndrome by abnormal energy and lipid metabolism,11 the triglyceride‐glucose (TyG) index has recently been widely used as a surrogate marker for IR. TyG is calculated using triglycerides (TG) and fasting blood glucose (FBG).11 Although the conventional TyG index has been widely adopted, its predominant reliance on lipid and glycemic parameters may inadequately reflect the comprehensive influence of obesity and fat distribution. Additional biomarkers derived from TyG, such as triglyceride‐glucose‐waist circumference (TyG‐WC), triglyceride‐glucose‐body mass index (TyG‐BMI) and triglyceride‐glucose‐waist‐to‐height ratio (TyG‐WHtR) have also been developed to study the occurrence and progression of diseases associated with metabolic syndrome and diabetes.12 TyG‐WC integrates waist circumference to assess visceral fat distribution, offering a more direct association between abdominal obesity and visceral adipose‐related IR.13 TyG‐BMI incorporates BMI to evaluate the metabolic impact of systemic obesity,14 while TyG‐WHtR employs waist‐to‐height ratio to standardize fat distribution assessment across individuals of varying heights.15
Diabetes, obesity and metabolic syndrome are well‐known risk factors for OAB. Recently, we reported that insulin signalling and adiponectin signalling play important roles in regulating bladder function, and disruption of these pathways leads to bladder dysfunctions like overactivity.16, 17 These signalling pathways are critical in energy and lipid metabolisms, including blood glucose and TyG. However, the association of TyG and its derived indices with OAB is unknown. We thus speculate that TyG and related indices might be strongly associated with OAB, and we will further evaluate whether OAB could impact all‐cause and cardiovascular mortality in women.
MATERIALS AND METHODS
2
Study population
2.1
The population included in this study was collected from the 2007 to 2018 National Health and Nutrition Examination Survey (NHANES). NHANES is a cross‐sectional study administered by the National Center for Health Statistics (NCHS) that assesses the health and nutritional status of the U.S. population. The survey collects demographic information, socioeconomic data, dietary details, physical examinations, laboratory tests and health‐related questions. The NHANES protocols were reviewed and approved by the NCHS Ethics Committee, and all participants signed informed consent forms during the survey process.18 The study included 30 213 female participants aged 20 years and older.
Exclusion criteria were as follows: a) unknown TyG‐related indices (n = 21 409); b) unknown OAB survey data (n = 2100); c) unknown education level and marital status (n = 8); d) unknown hypertension and diabetes status (n = 12); e) unknown physical activity status (n = 5); f) unknown smoking and alcohol consumption status (n = 8); g) unknown kidney function (n = 34); and (h) unknown blood lipid levels (n = 57). After excluding all relevant factors, a total of 6580 individuals were selected.
Study variables and outcome
2.2
The primary study variables include the diagnosis of OAB and the calculation of TyG‐related indices. The diagnosis of OAB was determined based on responses to the questions in the “Kidney Conditions ‐ Urology” section of the survey: KIQ044 (During the past 12 months, have you leaked or lost control of even a small amount of urine with an urge or pressure to urinate and you could not get to the toilet fast enough?), KIQ450 (How frequently does this occur?) and KIQ480 (During the past 30 days, how many times per night did you most typically get up to urinate, from the time you went to bed at night until the time you got up in the morning.). The Overactive Bladder Symptom Score (OABSS) was used to quantify the severity of OAB, with individuals having an OABSS ≥ three diagnosed as OAB.19 Specifically, the KIQ044 question was used to determine the presence or absence of urinary frequency, while KIQ450 and KIQ480 were used to quantify the OAB score. Table S1 presents specific scoring criteria for quantifying OAB, based on symptom frequency conversion criteria recorded in NHANES and OABSS scores.
The calculation of the TyG‐related indices was as follows: TyG index = ln[TG (mg/dL) × FBG (mg/dL)/2], TyG‐BMI index = ln[TG (mg/dL) × FBG (mg/dL)/2] × BMI, TyG‐WC index = ln[TG (mg/dL) × FBG (mg/dL)/2] × WC and TyG‐WHtR index = ln[TG (mg/dL) × FBG (mg/dL)/2] × WC/Height.
Other covariates include age, race, educational level, marital status, hypertension, diabetes, smoking, alcohol consumption, participation in work activities, participation in recreational activities, BMI, WC, FBG, TG, high‐density lipoprotein (HDL), low‐density lipoprotein (LDL), total cholesterol (TC), blood urea nitrogen, creatinine and uric acid. Hypertension and diabetes are based on self‐reported physician‐diagnosis.
Individual mortality data were obtained from the NHANES public‐use linked mortality files through December 31, 2019, which link to the National Death Index (NDI) maintained by the NCHS (https://www.cdc.gov/nchs/data-linkage/mortality-public.htm#). All‐cause mortality refers to deaths from all causes, and cardiovascular mortality refers to deaths due to heart disease (054–068).
Statistical analysis
2.3
Categorical variables were presented as frequencies (n) and percentages (%) and were analysed using the Chi‐square test. A weighted analysis of the data was performed. Kaplan–Meier (KM) curves were used to evaluate the impact of the OAB on all‐cause and cardiovascular mortality. Multivariate Cox regression was employed to assess the association between OAB and all‐cause and cardiovascular mortality, reporting adjusted hazard ratios (aHR) with 95% confidence intervals (CI). To examine the association between TyG‐related indices and OAB, dose–response curves of restricted cubic spline (RCS) and logistic regression analysis were applied to calculate adjusted odds ratios (aOR) with 95% CI. Receiver Operating Characteristic (ROC) curves were used to evaluate the accuracy of TyG‐related indices for OAB, and the area under the curve (AUC) was reported.
We constructed four different models in Cox regression and logistic regression analyses. Model 1 is a univariate regression analysis; Model 2 adjusts for general covariates, including age, race, educational level and marital status; Model 3 further adjusts for disease conditions, including hypertension, diabetes, smoking and alcohol consumption; Model 4 adds additional adjustments for physical activity status, renal function and blood lipid levels. Propensity score matching (PSM) is a statistical method used to mitigate bias caused by non‐randomized group allocation in observational studies.20 To balance the differences between the OAB and non‐OAB groups, we used a 1:1 PSM method, adjusting for the following confounding variables: age, race, education level, marital status, hypertension, diabetes, smoking, alcohol consumption and physical activity status. Data were reanalysed after PSM to test the validity. All data and charts in this study were organized and analysed using R software (version 3.5.3) and SPSS software (version 25.0). A p‐value of less than 0.05 was considered statistically significant.
RESULTS
3
Demographic and clinicopathologic characteristics
3.1
Among the 6580 female participants, 1581 (24.0%) were diagnosed with OAB. Table S2 presents the clinical baseline characteristics of the participants. The chi‐square test revealed significant differences between the OAB and non‐OAB groups in terms of age, race, educational level, marital status, hypertension, diabetes, smoking, alcohol consumption, moderate work activity and recreational activity (All p < 0.05). Patients with OAB were more likely to be older (>60 years, 49.7% vs. 26.2%), black (27.1% vs. 18.3%), less educated (high school: 33.3% vs. 19.7%), unmarried (60.7% vs. 51.0%), have hypertension (56.7% vs. 31.0%) and have diabetes (23.1% vs. 8.7%). Additionally, BMI, WC, FBG, TG, HDL, TC, TyG, TyG‐BMI, TyG‐WC, TyG‐WHtR, blood urea nitrogen, creatinine and uric acid levels were all significantly higher in the OAB group compared to the non‐OAB group.
OAB was strongly associated with all‐cause and cardiovascular death
3.2
We assessed the association of OAB with all‐cause and cardiovascular mortality among all participants using KM survival curves and Cox survival regression analyses. The KM survival curves showed that participants in the OAB group had higher all‐cause mortality (Figure S1 A) and cardiovascular mortality (Figure S1 B) compared to the non‐OAB group. Subsequently, the Cox survival regression analysis showed that OAB significantly increased the mortality risk for participants in all four models (Table 2 and Table S3). After adjusting for all variables (model 4), the OAB group had a 1.414‐fold (95% CI 1.167–1.714, p < 0.001; Figure S2A) increased risk of all‐cause mortality and a 1.528‐fold (95% CI 1.026–2.274, p = 0.037; Figure S2B) increased risk of cardiovascular mortality compared to the non‐OAB group.
To better balance the confounding factors between the OAB and non‐OAB groups, we performed a 1:1 PSM analysis, ultimately including 846 participants in both the OAB and non‐OAB groups. The clinical baseline characteristics of the 1692 participants after PSM analysis were presented in Table 1. After PSM, the OAB group still had higher BMI, WC, TyG‐BMI, TyG‐WC and TyG‐WHtR levels than the non‐OAB group. The KM survival curve results showed that the OAB group had higher all‐cause mortality (Figure 1A) and cardiovascular mortality (Figure 1B) compared to the non‐OAB group. Multivariate Cox regression analysis revealed a 1.457‐fold (95% CI 1.107–1.918, p = 0.007; Figure 2A) increased risk of all‐cause mortality and a 1.939‐fold (95% CI 1.048–3.589, p = 0.035; Figure 2B) increased risk of cardiovascular mortality in the OAB group compared to the non‐OAB group (Table 2 and Table S4).
All‐cause and cardiovascular mortality curves between the overactive bladder and the non‐overactive bladder group after 1:1 propensity score matching (PSM). (A) All‐cause mortality curves; (B) cardiovascular mortality curves.
Forest plots of different models of multivariate cox regression analysis of the relation between OAB and all‐cause and cardiovascular deaths in women after 1:1 propensity score matching (PSM). (A) All‐cause mortality; (B) cardiovascular mortality.
Association between TyG‐related indices and OAB
3.3
RCS curves showed a nonlinear positive association between OAB and TyG‐related indices, including BMI, WC, TyG, TyG‐BMI, TyG‐WC and TyG‐WHtR before and after PSM (Figure 3 and Figure S3). ROC curves were further used to assess the accuracy of BMI, WC, TyG, TyG‐BMI, TyG‐WC and TyG‐WHtR in predicting OAB. The results indicated that TyG‐WHtR exhibited the strongest association with OAB among the TyG‐related indices before and after PSM. (Table S5).
The dose–response analysis between TyG‐related indices and overactive bladder occurrence before propensity score matching (PSM). (A) BMI; (B) WC; (C) TyG; (D) TyG‐BMI; (E) TyG‐WC; (F) TyG‐WHtR. SD = standard deviation; CI = confidence interval.
Logistic regression analysis was then used to assess the OR between TyG‐related indices and OAB. The results indicated that BMI, WC, TyG‐BMI, TyG‐WC and TyG‐WHtR were all associated with the risk of OAB after adjusting for all confounding variables. Among these, TyG‐WHtR exhibited the strongest positive association with OAB. Compared to the Q1 of the TyG‐WHtR, the OAB risks for Q2, Q3 and Q4 were 1.564 (95% CI 1.261–1.940, p < 0.001), 2.084 (95% CI 1.663–2.613, p < 0.001) and 3.135 (95% CI 2.450–4.011, p < 0.001), respectively, before PSM (Figure S4), and 1.644 (95% CI 1.200–2.251, p = 0.002), 2.036 (95% CI 1.472–2.816, p < 0.001) and 2.883 (95% CI 2.084–3.988, p < 0.001), respectively, after PSM (Figure S5).
DISCUSSION
4
In this nationally representative cross‐sectional study, we found that all‐cause mortality and cardiovascular mortality were significantly higher in women with OAB compared to those without OAB. Multivariable Cox regression analysis further revealed that OAB was an independent risk factor for both all‐cause and cardiovascular mortality in women. Interestingly, TyG‐related indices, including BMI, WC, TyG, TyG‐BMI, TyG‐WC and TyG‐WHtR, exhibited a dose‐dependent, nonlinear positive association with OAB. Moreover, ROC curves demonstrated that TyG‐WHtR shows the strongest association with OAB, and multivariate logistic regression analysis indicated that TyG‐WHtR is an independent risk factor for OAB. The positive association between OAB and mortality, as well as the positive association between OAB and TyG‐related indices, were all confirmed in a 1:1 matched cohort after PSM. These findings highlight the importance of OAB as a risk factor for mortality in women and suggest the value of TyG‐related indices as simple and effective biomarkers for evaluating OAB, thereby promoting individualized surveillance and management.
OAB is a common disease in women, with its prevalence increasing with age. OAB can lead to a range of physical, psychological and social problems, including sleep disruption, increased risk of falls, reduced social activity and depression.21 Studies have shown that nocturia, a common symptom of OAB, serves as a significant contributor to sleep disruption in adults, severely impairing patients' sleep and overall quality of life, and potentially leading to increased mortality.22 Furthermore, Gong et al.23 demonstrated that OAB exhibits positive correlations with both the incidence of suicidal ideation among participants experiencing such thoughts and all‐cause mortality. These studies revealed that depression acts as a mediating factor in the association between OAB and suicidal ideation. OAB and urinary incontinence are also strongly associated with cardiovascular diseases like heart failure, contributing to cardiovascular mortality.24 Due to frequent urination and urgency, patients with OAB are more likely to have reduced social engagement.25
As mentioned earlier, metabolic syndrome is strongly associated with OAB.26 A follow‐up study of women over 40 years old in the UK found that diabetes was an independent risk factor for OAB.27 A survey involving 5204 women aged 18 and older revealed that BMI was an independent risk factor for OAB,2 with women having a BMI greater than 30 being 2.2 times more likely to develop OAB compared to those with a BMI less than 24. In a survey of 518 women with type 2 diabetes in Taiwan,28 OAB was significantly more prevalent in women with metabolic syndrome, experiencing more severe symptoms of urgency and nocturia.
TyG index was an effective novel biomarker for assessing insulin resistance (IR), aiding clinicians in their decision‐making.11 Studies have shown that an elevated TyG index is significantly associated with an increased risk of type 2 diabetes, making it a valuable tool for diabetes risk screening.29, 30 Additionally, a higher TyG index is closely linked to an increased risk of diabetes complications, such as atherosclerosis, coronary artery disease, diabetic nephropathy and diabetic retinopathy.31 Furthermore, an elevated TyG index is associated with a higher risk of major adverse cardiac events in patients with triple‐vessel disease (TVD).32
Obesity is well known to be associated with OAB and urinary incontinence, particularly in women, where the risk of OAB increases with WC, hip circumference and BMI.33 Central obesity, defined by WC and WHtR, is a key indicator for assessing the risk of various obesity‐related chronic diseases.34 Recent studies have examined new TyG‐related indices that combine the TyG index with obesity indicators, such as TyG‐WC, TyG‐BMI and TyG‐WHtR.35 Compared to the original TyG index, these new indices may offer better value for assessing disease outcomes.36 WHtR serves as a practical marker for both generalized and abdominal adiposity. Evidence indicates that WHtR demonstrates better accuracy than WC and BMI in identifying cardiometabolic risk factors.37 The TyG‐WHtR index, which standardizes adiposity distribution assessment across individuals of varying heights using waist‐to‐height ratio, has been consistently shown in multiple studies to exhibit enhanced value for assessing disease risks.38, 39 In the current study, we found that TyG‐WHtR outperformed the other indices in assessing the occurrence of OAB, both before and after PSM. Our studies also confirmed that the TyG‐WHtR index has a superior value for assessing cardiovascular disease and related mortality risk compared to the TyG index.40 For female OAB patients, regular monitoring of the TyG‐WHtR index may benefit the management of the OAB occurrence. For individuals with high TyG‐WHtR, timely management of blood glucose, triglycerides and waist circumference can potentially reduce the incidence of OAB.
This study is the first comprehensive assessment of the association between OAB and all‐cause and cardiovascular mortality in women, as well as the first evaluation of the association of TyG‐related indices with OAB. The large‐scale population‐based study, combined with a long follow‐up period, enhances the reliability of the data. However, there are several limitations to this study. First, as a retrospective study, the findings need further validation with prospective studies. Second, the diagnosis of OAB was based on OABSS scores, which may be subject to biases, including participant recall bias. NHANES lacks specific data on other comorbidities that may compound the association between overactive bladder and all‐cause mortality. Although the PSM method was used in this study, PSM does not eliminate all potential confounding factors such as lifestyle differences and medication use history. Finally, since the NHANES samples are limited to the US population, the generalizability of the findings to other countries remains unvalidated, highlighting the need for prospective international multicenter studies.
CONCLUSION
5
In conclusion, our study demonstrates that OAB is an independent risk factor for both all‐cause mortality and cardiovascular mortality in the female population. Furthermore, the TyG‐WHtR index exhibits the strongest association with OAB, making it a simple and easily calculated clinical biomarker for OAB management.
AUTHOR CONTRIBUTIONS
Weipu Mao and Sagar Barge: data analysis and writing; Weipu Mao: data collection; Zhaobo Luo: interpretation of the results and revision; WY: interpretation, revision, review and final approval. All authors reviewed the manuscript.
CONFLICT OF INTEREST STATEMENT
We declare no conflicts of interest.
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
NHANES was conducted with approval by the National Center for Health Statistics Ethics Review Board and obtained informed written consent from all the individuals involved in the study.
CONSENT FOR PUBLICATION
Not applicable.
Supporting information
Figure S1. All‐cause and cardiovascular mortality curves between the overactive and non‐overactive bladder groups before 1:1 propensity score matching (PSM).
Figure S2. Forest plots of different models of multivariate Cox regression analysis of the relation between OAB and all‐cause and cardiovascular deaths in women before 1:1 propensity score matching (PSM).
Figure S3. The dose–response analysis between TyG‐related indices and overactive bladder occurrence after propensity score matching (PSM).
Figure S4. Forest plots of different models of multivariate logistic regression analysis of the relation between TyG‐related indices and overactive bladder occurrence before 1:1 propensity score matching (PSM).
Figure S5. Forest plots of different models of multivariate logistic regression analysis of the relation between TyG‐related indices and overactive bladder occurrence after 1:1 propensity score matching (PSM).
Table S1. Conversion of symptom frequencies recorded in NHANES to OABSS scores. Table S2. Baseline characteristics of participants between 2007 and 2018 before PSM. Table S3. Cox regression analysed the relationship between overactive bladder and all‐cause and cardiovascular mortality before PSM. Table S4. Cox regression analysed the relationship between overactive bladder and all‐cause and cardiovascular mortality after PSM. Table S5. Comparison of area under the curve (AUC) between different triglyceride glucose‐related indicators and the presence of overactive bladder before and after PSM.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Haylen BT , de Ridder D , Freeman RM , Swift SE , Berghmans B , Lee J , et al. An international Urogynecological association (IUGA)/international continence society (ICS) joint report on the terminology for female pelvic floor dysfunction. Neurourol Urodyn. 2010;29(1):4–20. 10.1002/nau.20798 19941278 · doi ↗ · pubmed ↗
- 2Stewart WF , Van Rooyen JB , Cundiff GW , Abrams P , Herzog AR , Corey R , et al. Prevalence and burden of overactive bladder in the United States. World J Urol. 2003;20(6):327–336. 10.1007/s 00345-002-0301-4 12811491 · doi ↗ · pubmed ↗
- 3Chuang YC , Liu SP , Lee KS , Liao L , Wang J , Yoo TK , et al. Prevalence of overactive bladder in China, Taiwan and South Korea: results from a cross‐sectional, population‐based study. Low Urin Tract Symptoms. 2019;11(1):48–55. 10.1111/luts.12193 28967230 PMC 7379992 · doi ↗ · pubmed ↗
- 4Irwin D , Milsom I , Hunskaar S , Reilly K , Kopp Z , Herschorn S , et al. Population‐based survey of urinary incontinence, overactive bladder, and other lower urinary tract symptoms in five countries: results of the EPIC study. Eur Urol. 2006;50(6):1306–1314; discussion 14‐5. 10.1016/j.eururo.2006.09.019 17049716 · doi ↗ · pubmed ↗
- 5Mori S , Matsuo T , Honda H , Araki K , Mitsunari K , Ohba K , et al. Relationship between overactive bladder and bone fracture risk in female patients. In Vivo. 2024;38(4):2031–2040. 10.21873/invivo.13661 38936892 PMC 11215605 · doi ↗ · pubmed ↗
- 6Szabo SM , Gooch KL , Walker DR , Johnston KM , Wagg AS . The association between overactive bladder and falls and fractures: a systematic review. Adv Ther. 2018;35(11):1831–1841. 10.1007/s 12325-018-0796-8 30255417 PMC 6223978 · doi ↗ · pubmed ↗
- 7Saeedi P , Petersohn I , Salpea P , Malanda B , Karuranga S , Unwin N , et al. Global and regional diabetes prevalence estimates for 2019 and projections for 2030 and 2045: results from the international diabetes federation diabetes atlas, 9(th) edition. Diabetes Res Clin Pract. 2019;157:107843. 10.1016/j.diabres.2019.107843 31518657 · doi ↗ · pubmed ↗
- 8Ye Z , Li L , Yang L , Zhuang L , Aspatwar A , Wang L , et al. Impact of diabetes mellitus on tuberculosis prevention, diagnosis, and treatment from an immunologic perspective. Exploration (Beijing). 2024;4(5):20230138. 10.1002/EXP.20230138 39439490 PMC 11491313 · doi ↗ · pubmed ↗