A Fragmented Rib as the First Clue to Advanced Lung Adenocarcinoma
Hiroshi Ishii, Takuhide Utsunomiya, Yoshiaki Kinoshita, Hisako Kushima

TL;DR
A severely fragmented rib can be an early sign of advanced lung adenocarcinoma, even before breathing symptoms occur.
Contribution
This paper presents a rare case where rib fragmentation was the first indicator of advanced lung cancer.
Findings
Rib destruction on imaging can precede respiratory symptoms in lung adenocarcinoma.
Uncommon radiographic features like rib fragmentation may signal underlying malignancy.
Abstract
Severe rib destruction on initial imaging can be the first clue to advanced lung adenocarcinoma with skeletal metastases, even before respiratory symptoms appear. Osteolytic bone metastases are common in advanced lung cancer, particularly adenocarcinoma; however, here we present a rare case of a patient presenting with dramatic rib fragmentation. This case highlights the importance of recognising uncommon radiographic features that may reflect underlying malignancy.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1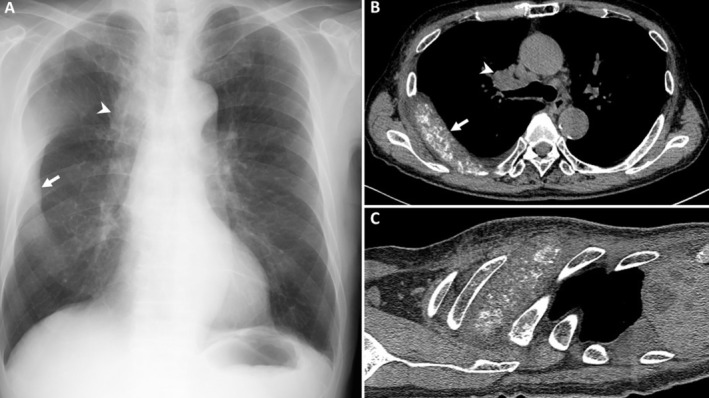 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsLung Cancer Treatments and Mutations · Peptidase Inhibition and Analysis · Cancer Diagnosis and Treatment
A man in his 80s with a history of chronic smoking presented with left shoulder pain. Computed tomography (CT) of the shoulder incidentally revealed nodules in the right upper lobe of the lung. Chest radiography showed a banana‐shaped opacity and a tumorous shadow in the right lung field (Figure 1A). Chest CT identified a fragmented and markedly enlarged rib, consistent with osteolytic metastasis (Figure 1B,C). Additionally, CT showed a right upper lobe mass, pulmonary nodules, and mediastinal lymphadenopathy.
Laboratory testing revealed elevated carcinoembryonic antigen (502 ng/mL; normal ≤ 5) and alkaline phosphatase (1125 U/L; normal ≤ 322), suggestive of active tumour burden and bone involvement. A biopsy confirmed primary lung adenocarcinoma. Whole‐body evaluation revealed multiple skeletal metastases to vertebrae and ribs.
Osteolytic bone metastases are common in advanced lung cancer [1, 2], particularly adenocarcinoma, but such dramatic rib fragmentation at presentation is rare. It can easily be misinterpreted or overlooked if clinicians are not vigilant. This case highlights the importance of recognising uncommon radiographic features that may reflect underlying malignancy.
Author Contributions
H.I.: patient evaluation, manuscript drafting, image selection, final approval of the manuscript. T.U.: investigation; writing – review and editing, visualisation, final approval of the manuscript. Y.K.: writing review and editing, final approval of the manuscript. H.K.: writing – review and editing, final approval of the manuscript.
Consent
The authors declare that written informed consent was obtained for the publication of this manuscript and accompanying images using the consent form provided by the Journal.
Conflicts of Interest
The authors declare no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Y. J. Cho , Y. M. Cho , S. H. Kim , K. H. Shin , S. T. Jung , and H. S. Kim , “Clinical Analysis of Patients With Skeletal Metastasis of Lung Cancer,” BMC Cancer 19 (2019): 303.30943924 10.1186/s 12885-019-5534-3PMC 6446278 · doi ↗ · pubmed ↗
- 2K. Cetin , C. F. Christiansen , J. B. Jacobsen , M. Nørgaard , and H. T. Sørensen , “Bone Metastasis, Skeletal‐Related Events, and Mortality in Lung Cancer Patients: A Danish Population‐Based Cohort Study,” Lung Cancer 86 (2014): 247–254.25240518 10.1016/j.lungcan.2014.08.022 · doi ↗ · pubmed ↗