Forward-viewing echoendoscope provides single sessional three biliary drainage routes in a patient with pancreatoduodenectomy
Tesshin Ban, Yoshimasa Kubota, Shun Sasoh, Tomoaki Ando, Takashi Joh

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
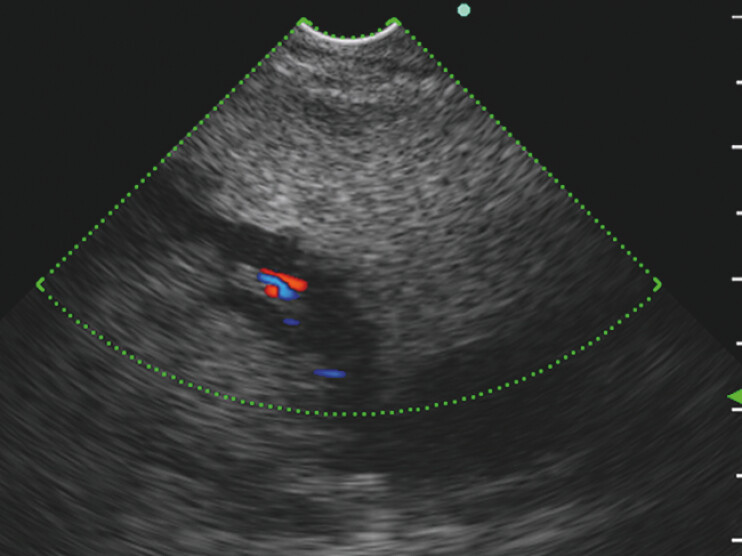 Fig. 1
Fig. 1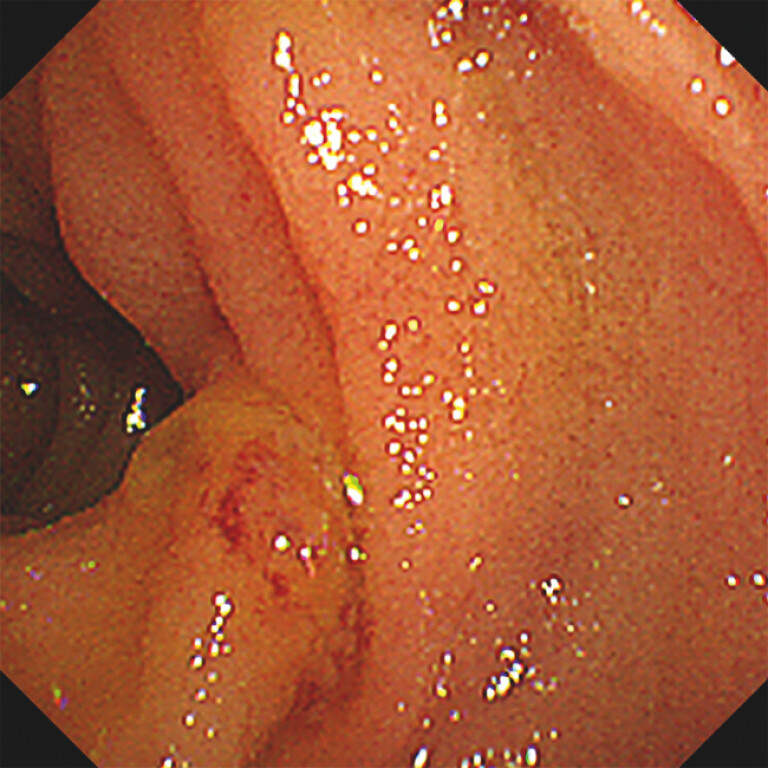 Fig. 2
Fig. 2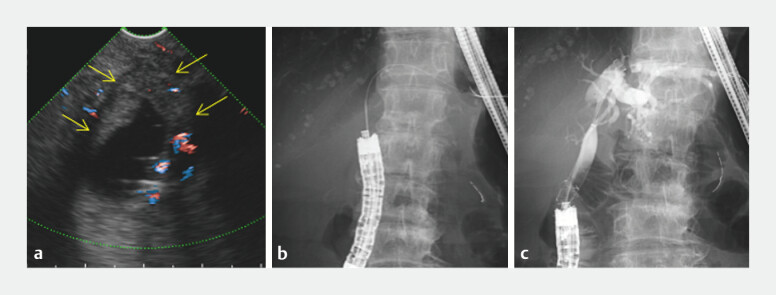 Fig. 3
Fig. 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPancreatic and Hepatic Oncology Research · Gallbladder and Bile Duct Disorders · Pancreatitis Pathology and Treatment
In patients with pancreatoduodenectomy, echoendoscopic intubation to the hepaticojejunostomy site on the jejunal limb is necessary to visualize the perihilar area 1 . Therefore, intubation of a forward-viewing curvilinear echoendoscope (FV-CLS) may be considered when balloon enteroscopy-assisted cholangiopancreatography fails 1 2 3 . A dedicated partially covered self-expandable metal stent (PCSEMS) with an excellent anchoring system has been developed for use in endoscopic ultrasound-guided biliary drainage (EUS-BD) 4 5 . Herein, we present the initial FV-CLS intubation, which provided three single-session biliary drainage routes, in a patient with perihilar recurrence after pancreatoduodenectomy.
An 84-year-old woman who underwent pancreatoduodenectomy with modified Child reconstruction for stage IIB pancreatic cancer was referred to our hospital due to perihilar obstruction with a dilated biliary tree ( Video 1 ). Our biliary drainage strategy involved direct cannulation of the biliary anastomosis or EUS-BD via the anastomosis site or residual stomach, all of which were attempted in a single session using FV-CLS (TGF-UC260J; Olympus Medical Systems, Tokyo, Japan). The FV-CLS was advanced into the reconstructed alimentary tract. However, the left intrahepatic biliary branch was 3.1 mm in diameter on endosonography of the residual stomach ( Fig. 1 , Video 1 ), and the anastomosis was obscured owing to tumor involvement ( Fig. 2 , Video 1 ). Therefore, we selected EUS-BD via the anastomosis site as follows: a 19-gauge needle puncture with a 0.025-inch guidewire advancement to the left bile duct, a 4-mm balloon dilation, and a PCSEMS (Niti-S Spring Stopper, 8 mm/10 cm; Taewoong Medical, Gimpo, Korea) deployment ( Fig. 3 , Video 1 ). The patient’s clinical course was uneventful.
Forward-viewing echoendoscope provides single sessional three biliary drainage routes in a patient with pancreatoduodenectomy.Video 1
Left intrahepatic biliary branch depicted by forward-viewing curved linear echoendoscope (FV-CLS) from the residual stomach. Endoscopic ultrasonography-guided biliary drainage (EUS-BD) via the residual stomach was likely achieved; however, we hesitated to perform a puncture because the left intrahepatic biliary branch was narrow (3.1 mm in diameter).
Biliary anastomosis area on the jejunal limb in the endoscopic view of FV-CLS. We sought a biliary anastomosis point for cannulation; however, this was challenging because of the deformity caused by tumor invasion.
EUS-BD via the anastomosis site on the jejunal limb using FV-CLS. a FV-CLS revealed perihilar recurrence obstructing the dilated left hepatic duct after pancreatoduodenectomy. EUS-BD was feasible via the anastomosis site. Yellow solid arrows indicate the left hepatic duct involved in tumor recurrence. b A 19-gauge needle with a 0.025-inch guidewire was then advanced into the left hepatic duct. c A partially covered self-expandable metal stent with an antimigration system recanalized the obstruction.
Direct intubation with FV-CLS potentially provides three biliary access routes in a single session for patients with pancreatoduodenectomy and reconstruction, followed by biliary obstruction caused by perihilar recurrence: first, cannulation to the anastomosis if visible; second, EUS-BD via the afferent limb; and third, EUS-BD via the residual stomach.
Endoscopy_UCTN_Code_TTT_1AS_2AH
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Katanuma A Hayashi T Kin T Interventional endoscopic ultrasonography in patients with surgically altered anatomy: Techniques and literature review Dig Endosc 20203226327431643105 10.1111/den.13567 · doi ↗ · pubmed ↗
- 2Hara K Okuno N Haba S Forward viewing liner echoendoscopy for therapeutic interventions Clin Endosc 20245717518010.5946/ce.2023.27138419166 PMC 10984744 · doi ↗ · pubmed ↗
- 3Testoni PA Mariani A Aabakken L Papillary cannulation and sphincterotomy techniques at ERCP: European Society of Gastrointestinal Endoscopy (ESGE) Clinical Guideline Endoscopy 20164865768310.1055/s-0042-10864127299638 · doi ↗ · pubmed ↗
- 4Takasaki Y Isayama H Shin KS Measurement of the anchoring force of covered self-expandable and lumen-apposing metal stents for interventional endoscopic ultrasonography Dig Endosc 2023359610210.1111/den.1440635837746 · doi ↗ · pubmed ↗
- 5Ishii S Isayama H Sasahira NA pilot study of Spring Stopper Stents: Novel partially covered self-expandable metallic stents with anti-migration properties for EUS-guided hepaticogastrostomy Endosc Ultrasound 20231226627237148139 10.4103/EUS-D-22-00104 PMC 10237616 · doi ↗ · pubmed ↗