Endoscopic drainage for a thoracic abscess caused by delayed perforation after endoscopic submucosal dissection for gastric tube cancer: a case report
Aiji Hattori, Yuji Owaki, Atsushi Inaba, Daisuke Kajiyama, Kazuma Sato, Takeo Fujita, Tomonori Yano

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
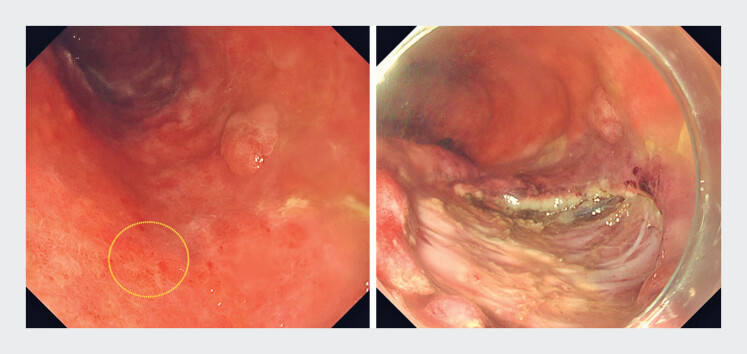 Fig. 1
Fig. 1 Fig. 2
Fig. 2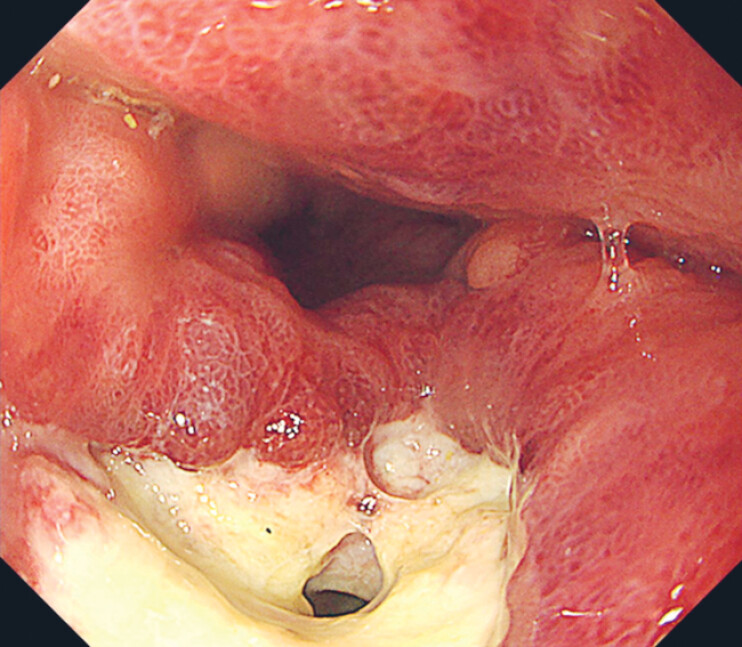 Fig. 3
Fig. 3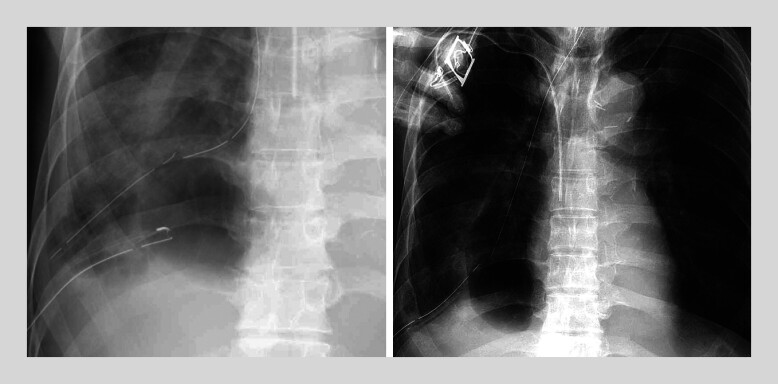 Fig. 4
Fig. 4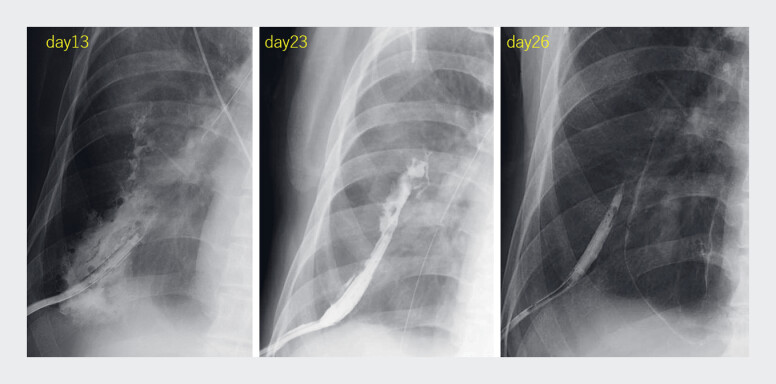 Fig. 5
Fig. 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGastric Cancer Management and Outcomes · Esophageal and GI Pathology · Tracheal and airway disorders
A 75-year-old man with a history of esophageal cancer treated with subtotal esophagectomy developed a 10-mm early gastric tube cancer (GTC) ( Fig. 1 ). Endoscopic submucosal dissection (ESD) was performed without immediate complications, and he was discharged six days later. Four days post-discharge, the patient presented with fever and lower back pain. Computed tomography (CT) revealed gastric wall thinning and a thoracic abscess in the right lower lung field ( Fig. 2 ). We diagnosed the patient with delayed perforation after ESD with a thoracic abscess. We initiated thoracic drainage, nasogastric tube insertion, and antibiotics.
A 10-mm early gastric tube cancer was identified on the posterior wall of the middle gastric tube (illustrated by the circle). Endoscopic submucosal dissection was performed on the lesion.
Computed tomography (CT) revealed the presence of gastric tube contents, a reduction in the thickness of the gastric tube wall as well as the presence of pleural effusion in the right posterior lower lung field.
Despite the initial interventions, his symptoms did not improve. An endoscopic examination was performed to assess the perforation site and revealed food residue in the gastric tube, which was removed. We attempted fistula closure with clips but failed due to mucosal edema and fibrosis ( Fig. 3 ). With persistent symptoms and inadequate drainage on follow-up CT, we attempted endoscopic drainage collaborating with thoracic surgeons.
The locus of perforation was duly recognized. The attempted closure of the fistula utilizing clips was deemed unsuccessful owing to considerable edema and fibrotic tissue surrounding the ulcer.
An ultrathin endoscope was inserted directly through the fistula into the abscess cavity for washing, removing septa within the abscess, and placing the guidewire, followed by nasogastric tube placement near the thoracic drain tube to make the communication ( Video 1 , Fig. 4 ).
Direct endoscopic drainage for a thoracic abscess caused by delayed perforation after endoscopic submucosal dissection for gastric tube cancer.Video 1
A nasogastric tube was placed near the thoracic drain tube to make the communication.
Continuous saline irrigation led to abscess shrinkage ( Fig. 5 ), symptom improvement, and discharge at 35 days post-admission.
Following the procedures, systematic saline irrigation was conducted on a daily basis via the nasogastric tube, resulting in a progressive reduction in the size of the abscess.
Only four cases of delayed perforation after ESD for GTC have been reported, all diagnosed early (1–3 days) post-ESD and treated conservatively 1 2 3 4 . In this case, the perforation was diagnosed 10 days after ESD. As time passed after the perforation, endoscopic closure of the fistula became challenging because of edema and fibrosis of the mucosa. Surgery for delayed perforation of GTC is highly invasive and difficult owing to its adhesion to vital organs. We performed direct endoscopic abscess drainage as an effective conservative treatment to avoid surgery.
Endoscopy_UCTN_Code_CPL_1AH_2AZ_3AD
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Osumi W Fujita Y Hiramatsu M Endoscopic submucosal dissection allows less-invasive curative resection for gastric tube cancer after esophagectomy – a case series Endoscopy 20094177778019746318 10.1055/s-0029-1215024 · doi ↗ · pubmed ↗
- 2Nonaka S Oda I Sato C Endoscopic submucosal dissection for gastric tube cancer after esophagectomy Gastrointest Endosc 20147926027010.1016/j.gie.2013.07.05924060521 · doi ↗ · pubmed ↗
- 3Suzuki H Oda I Sekiguchi M Management and associated factors of delayed perforation after gastric endoscopic submucosal dissection World J Gastroenterol 201521126351264310.3748/wjg.v 21.i 44.1263526640340 PMC 4658618 · doi ↗ · pubmed ↗
- 4Hirayama Y Fujisaki J Yoshimizu S Efficacy and safety of endoscopic resection for gastric tube cancer after surgical resection of esophageal squamous cell carcinoma Esophagus 20191619420010.1007/s 10388-018-00653-w 30600485 · doi ↗ · pubmed ↗