Combination Treatment With Intravenous and Oral Calcimimetics for Secondary Hyperparathyroidism in Hemodialysis Patients Who Decline Parathyroidectomy
Ryoichi Nakazawa, Akira Onozaki, Kazuhiro Akiyama, Takashi Uchino, Nakanobu Azuma

TL;DR
This study shows that combining intravenous and oral calcimimetics can effectively lower parathyroid hormone levels in hemodialysis patients who refuse surgery for secondary hyperparathyroidism.
Contribution
The study introduces a combination therapy of intravenous and oral calcimimetics as a non-surgical treatment for refractory SHPT in hemodialysis patients.
Findings
Combination calcimimetic treatment significantly reduced plasma PTH levels in all patients.
No gastrointestinal complications were reported, indicating good tolerability of the regimen.
Two patients developed renal cancer, highlighting the need for long-term safety monitoring.
Abstract
Background and aim: Secondary hyperparathyroidism (SHPT) is a common and serious complication in patients on hemodialysis (HD), leading to significant morbidity and mortality. Parathyroidectomy (PTx) is an established treatment for refractory SHPT, but many patients refuse this surgical option. This study evaluates the efficacy of combination treatment using intravenous and oral calcimimetics in managing SHPT in patients who decline PTx. This study aimed to assess the impact of combination calcimimetic treatment on plasma parathyroid hormone (PTH) levels, mineral metabolism, and clinical outcomes in patients on hemodialysis with SHPT who refuse PTx. Methods: This retrospective study involved seven patients on HD with refractory SHPT who declined PTX. They were treated with various combinations of intravenous (etelcalcetide or upacicalcet), oral (cinacalcet or evocalcet) calcimimetics,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
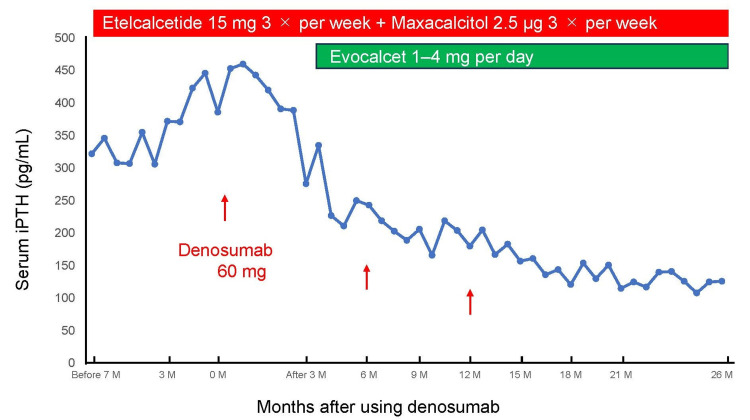 Figure 1
Figure 1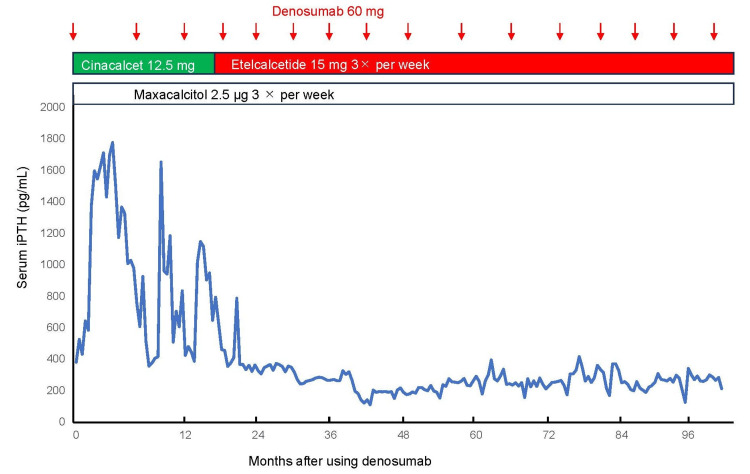 Figure 2
Figure 2| Patient number | Age (years)/ sex | Cause of renal failure | HD vintage (years) | Corrected serum calcium level (mg/dL) | Serum phosphorus level (mg/dL) | Serum ALP level (IU/mL) | Parathyroid gland volume (mm3) | Number of parathyroid glands | iPTH (before the treatment) (pg/mL) | iPTH (after the treatment) (pg/mL) |
| 1 | 54/M | CGN | 36 | 10.2 | 5.3 | 106 | 391 | 2+autograft | 319 | 282 |
| 2 | 63/F | AKI | 12 | 10.4 | 7.2 | 53 | 419 | 3 | 319 | 285 |
| 3 | 59/M | CGN | 16 | 10.5 | 3.4 | 68 | 671 | 4 | 389 | 126 |
| 4 | 69/M | CGN | 25 | 9.8 | 6.4 | 42 | 335 | 5 | 222 | 142 |
| 5 | 58/M | CGN | 8 | 10.1 | 6.0 | 69 | 543 | 3 | 212 | 175 |
| 6 | 52/M | CGN | 28 | 10.7 | 6.6 | 414 | 3,069 | 4 | 583 | 212 |
| 7 | 67/F | NS | 7 | 10.3 | 5.8 | 155 | 2,068 | 5 | 612 | 126 |
| Mean±SD | 60±6 | - | 19±11 | 10.3±0.3 | 5.8±1.2 | 130±131 | 1,071±1,069 | 3.7±1.1 | 379±161 | 193±69 |
| Patient number | Etelcalcetide (mg) | Upacicalcet (µg) | Evocalcet (mg) | Cinacalcet (mg) | Maxacalcitol (µg) | Denosumab (mg) | Other treatment | Prognosis | Complications | Period (mos) |
| 1 | 15×3 | - | 7 | - | 2.5×3 | - | PTx+AT | Death | - | 13 |
| 2 | - | 300×3 | 6 | - | 2.5×3 | - | - | - | - | 16 |
| 3 | 15×3 | - | 4 | - | 2.5×1 | ×3 | - | - | - | 24 |
| 4 | 15×3 | - | - | 50 | 2.5×3 | - | - | - | - | 15 |
| 5 | 15×3 | - | 2 | - | 2.5×3 | - | - | - | - | 10 |
| 6 | 15×3 | - | - | 12.5 | 2.5×3 | ×16 | - | - | Left renal cancer (Nx) | 100 |
| 7 | 10×3 | - | 12 | - | 2.5×3 | - | - | - | Right renal cancer (Nx) | 54 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsParathyroid Disorders and Treatments · Genetic Syndromes and Imprinting · Thyroid and Parathyroid Surgery
Introduction
Secondary hyperparathyroidism (SHPT) is a prevalent and severe complication of chronic kidney disease (CKD), particularly among patients undergoing long-term hemodialysis (HD). Persistent elevations in plasma parathyroid hormone (PTH) levels in SHPT disrupt calcium and phosphate homeostasis, leading to derangements in bone remodeling and cardiovascular function. These disturbances substantially increase the risks of fractures, vascular calcification, and cardiovascular morbidity and mortality, thereby exacerbating the already poor outcomes observed in this population [1,2].
Parathyroidectomy (PTx) has historically been considered the gold-standard treatment for severe and refractory SHPT. By surgically reducing parathyroid gland mass, PTx effectively achieves sustained biochemical control. However, the advent of calcimimetic agents, such as cinacalcet, has revolutionized SHPT management by offering a non-surgical alternative. Calcimimetics act on the calcium-sensing receptor (CaSR) of parathyroid cells, suppressing PTH secretion pharmacologically [3,4]. This innovation has significantly decreased the frequency of PTx procedures worldwide.
Despite these advancements, managing SHPT in patients who decline PTx remains a significant challenge. Reasons for refusing surgery may include personal preference, perceived risks, or comorbid conditions precluding safe surgical intervention. While monotherapy with either oral or intravenous calcimimetics has shown efficacy in moderate cases, it is often inadequate for achieving optimal biochemical targets in severe or refractory SHPT [5,6]. However, the use of two calcimimetics may not be allowed by insurance.
Combination therapy involving both intravenous and oral calcimimetics has emerged as a promising strategy to address these therapeutic limitations. This approach leverages the complementary pharmacokinetic and pharmacodynamic properties of different calcimimetic formulations to enhance PTH suppression and mineral metabolism control. However, evidence regarding the clinical efficacy, safety, and long-term outcomes of combination calcimimetic therapy remains sparse, particularly in patients who refuse PTx.
This retrospective study aimed to assess the impact of combination treatment using intravenous and oral calcimimetics on PTH levels, mineral metabolism, and clinical outcomes in patients on HD with refractory SHPT who decline PTx. By addressing this critical gap in the literature, the findings seek to inform personalized management strategies and improve care for this challenging patient population.
Materials and methods
Study design and patient selection
This retrospective clinical study was conducted as part of a routine clinical audit at the hemodialysis center of Tokatsu Clinic Hospital and its affiliated clinics in Matsudo, Japan. The study focused on patients undergoing HD who received calcimimetics, vitamin D receptor activators (VDRAs), and denosumab as part of their treatment for SHPT. The study design adhered to institutional data-handling protocols and was exempt from institutional review board approvals, as it used aggregated, de-identified patient data. Patients included in the study had refractory SHPT and were managed with calcimimetics, VDRAs, and denosumab between November 2015 and March 2024. Seven patients who declined PTx despite clinical indications were selected for analysis. PTx was recommended in cases where the intact PTH levels exceeded 500 pg/mL, plasma PTH levels were unresponsive to maximal doses of calcimimetics and VDRAs, or hyperphosphatemia or hypercalcemia could not be controlled medically [7]. This study was conducted according to the principles outlined in the Declaration of Helsinki. The Ethics Committee of the Tokatsu Clinic Hospital granted ethical approval (approval number 2024-4).
Data collection
Data were retrospectively extracted from electronic medical records as part of a one-time audit. Demographic information, health-related variables, and treatment regimens were collected using a clinical dashboard. The data included starting and maximum doses of calcimimetics, duration of treatment on HD, plasma intact PTH (iPTH) levels (measured biweekly), serum corrected calcium (calcium concentration {mg/dL} + 4-serum albumin {g/dL}), phosphorus, and alkaline phosphatase levels, dialysate calcium concentrations, and concomitant medications and reasons for treatment discontinuation. Laboratory analyses were performed using standard methods at the Department of Laboratory, Tokatsu Clinic Hospital. Plasma iPTH levels were measured using the Abbott ARCHITECT i2000SR PLUS analyzer with an electrochemiluminescence-based method, while calcium, phosphorus, and alkaline phosphatase were determined using a HITACHI LABOSPECT008a analyzer. Target ranges for serum phosphorus, corrected calcium, and iPTH levels were based on the Japanese Society for Dialysis Therapy guidelines as follows: 3.5-6.0 mg/dL, 8.4-10.0 mg/dL, and 60-240 pg/mL, respectively [7]. Once a year, parathyroid gland size was measured by neck ultrasound using the ellipsoid formula (π/6 × a × b × c, where a, b, and c represent the diameters of the gland in three dimensions) with a Canon Aplio flex ultrasound system [8].
Treatment protocol
Initial treatment involved a single calcimimetic at the maximum dose allowed by Japanese insurance, combined with a VDRA. When PTH control remained inadequate and PTx declined, alternative calcimimetic regimens or denosumab were introduced. Among the seven cases, one patient received a combination of etelcalcetide, VDRA, and denosumab. Four patients were treated with a regimen of etelcalcetide, evocalcet, and VDRA. One patient received etelcalcetide, cinacalcet, and VDRA. One patient was managed with upacicalcet, evocalcet, and VDRA. All patients received dialysis with a dialysate calcium concentration of 2.75 mEq/L to manage calcium-phosphorus balance effectively.
Outcomes measures
The primary outcomes included changes in plasma PTH levels, serum calcium, and phosphorus concentrations. Secondary outcomes included adverse effects such as gastrointestinal intolerance or other clinically significant events. Treatment efficacy and tolerability were assessed using routine laboratory and clinical evaluations.
Statistical analysis
Continuous variables were compared using the Wilcoxon signed-rank test in EZR (Easy R). A p-value <0.05 was considered statistically significant. Data analyses were performed using standard statistical software.
Results
Patient characteristics
This retrospective study analyzed seven patients on HD with confirmed indications for PTx who declined surgery. The study spanned from November 2015 to March 2024 and included five men and two women aged 52-69 years. The duration of HD ranged from 7 to 36 years (Table 1). Six patients presented with hypercalcemia (serum calcium >10.0 mg/dL), and plasma iPTH levels ranged from 212 to 612 pg/mL despite treatment with calcimimetics and VDRAs (Table 2). High-resolution ultrasonography revealed parathyroid gland volumes ranging from 335 to 3,069 mm^3^, with gland counts varying from two (with autografts in the forearm) to five (Table 1). No fractures were observed during the study period.
Reduction of plasma PTH levels
Combination treatment regimens led to a significant reduction in plasma PTH levels across all patients. Detailed changes in PTH levels are presented in Table 1, with trends illustrated in Figures 1, 2. Median PTH levels decreased from 379 pg/mL to 193 pg/mL after initiating combination therapy, demonstrating its efficacy in managing severe SHPT in patients who declined PTx. The consistency of the observed reduction across different treatment combinations highlights the therapeutic potential of this approach.
Changes in patient 3's plasma iPTH levels during combination treatment.iPTH: plasma intact PTH
Changes in patient 6's plasma iPTH levels during combination treatment.iPTH: plasma intact PTH
Tolerability
The combined calcimimetic regimens were well-tolerated, with no gastrointestinal complications reported during the observation period. This supports the feasibility of these regimens, especially for patients with known sensitivities to conventional calcimimetic monotherapy.
Adverse events
Although the treatment effectively controlled PTH levels, two significant adverse events were noted as follows: (1) renal cancer - two patients were diagnosed with renal cancer by annual abdominal echography, CT imaging, and hematuria, which was confirmed to be derived from acquired cystic disease of the kidney with unilateral removal of the kidney. (2) Cardiovascular mortality - one patient, who had been on dialysis for 36 years, succumbed to cardiovascular disease, a leading cause of mortality among the dialysis population. These findings underscore the complexity of managing SHPT in patients with advanced CKD and highlight the interplay between SHPT, its treatment, and the comorbidities inherent to this population.
Clinical implications
The study findings emphasize the necessity of combination calcimimetic therapy for achieving biochemical control of SHPT in patients who refuse PTx. However, the observed risks associated with long-term treatment underscore the importance of vigilant monitoring and individualized care to mitigate potential adverse effects.
Discussion
This study highlights two critical aspects of managing SHPT in patients on HD who refuse PTx. First, the results demonstrate that combination treatment with intravenous and oral calcimimetics, targeting distinct domains of the CaSR, effectively reduces plasma PTH levels in this challenging patient population. Second, the unexpected diagnosis of renal cancer in two patients during the study period underscores the complexity of long-term SHPT management and necessitates further investigation into its etiology and implications.
Since the advent of calcimimetics, the therapeutic paradigm for SHPT has shifted substantially from surgical to medical management. This shift is particularly evident in Japan, where the annual number of PTx procedures for SHPT decreased from 1,771 in 2007 to just 67 in 2022 [9,10]. The availability of multiple calcimimetic agents - cinacalcet, etelcalcetide, evocalcet, and upacicalcet - has broadened the range of treatment options. However, patient reluctance to undergo PTx, often due to concerns about surgical risks and personal preferences, has amplified reliance on pharmacological interventions.
The findings of this study align with in vitro evidence suggesting enhanced CaSR activation when intravenous and oral calcimimetics are combined. For instance, the concurrent use of etelcalcetide and cinacalcet has been shown to produce significantly higher intracellular inositol-1-phosphate levels in HEK-293T cells than either agent alone [11-13]. This pharmacological synergy likely underpins the substantial PTH reductions observed in our cohort. Despite these promising results, combination treatments' long-term safety and efficacy remain uncertain and warrant further investigation, as current evidence is predominantly limited to small-scale or preclinical studies.
The diagnosis of renal cancer in two patients during the study period raises pertinent questions about the potential relationship between SHPT, its treatments, and malignancy risk. Patients on HD are at an elevated risk of renal cancer, with a standardized incidence ratio of 4.03 compared to the general population [14,15]. While the causal link between SHPT treatments and cancer remains speculative, this finding underscores the importance of vigilant monitoring and necessitates additional research to elucidate potential mechanisms.
Strict PTH control is central to SHPT management. Recent studies suggest that achieving plasma iPTH levels below 60 pg/mL is not associated with increased mortality, supporting the strategy of aggressive PTH suppression through pharmacological or surgical means [16,17]. However, the benefits of such approaches must be carefully balanced against the potential risks, including possible malignancy development.
This study's limitations include its small sample size, retrospective design, and relatively short follow-up period. These factors constrain the generalizability of the findings and preclude definitive conclusions regarding causality or broader clinical implications. Prospective, large-scale studies are needed to validate the efficacy and safety of combination calcimimetic regimens and to investigate the potential links between SHPT treatments and long-term outcomes, including cancer risk.
Conclusions
Managing SHPT in patients on HD who decline PTx requires intricate and individualized pharmacotherapy strategies. This study demonstrates that combining dual calcimimetics with a VDRA can effectively control plasma PTH levels in this complex patient population. However, the occurrence of adverse events, such as renal cancer, highlights the need for cautious application of these therapies and further exploration of their long-term safety and clinical implications. Comprehensive, prospective research is essential to establish optimal treatment protocols for SHPT in patients unwilling or unable to undergo PTx.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Effect of cinacalcet on cardiovascular disease in patients undergoing dialysis N Engl J Med Chertow GM Block GA Correa-Rotter R 2482249436720122312137410.1056/NEJ Moa 1205624 · doi ↗ · pubmed ↗
- 2The regulation of parathyroid hormone secretion and synthesis J Am Soc Nephrol Kumar R Thompson JR 2162242220112116402110.1681/ASN.2010020186 PMC 5546216 · doi ↗ · pubmed ↗
- 3Calcium-mediated parathyroid hormone release changes in patients treated with the calcimimetic agent cinacalcet Nephrol Dial Transplant de Francisco AL Izquierdo M Cunningham J 289529012320081842482010.1093/ndt/gfn 191 · doi ↗ · pubmed ↗
- 4Structural mechanism of ligand activation in human calcium-sensing receptor Elife Geng Y Mosyak L Kurinov I 5201610.7554/e Life.13662 PMC 497715427434672 · doi ↗ · pubmed ↗
- 5Effect of etelcalcetide vs cinacalcet on serum parathyroid hormone in patients receiving hemodialysis with secondary hyperparathyroidism: a randomized clinical trial JAMA Block GA Bushinsky DA Cheng S 15616431720172809735610.1001/jama.2016.19468 · doi ↗ · pubmed ↗
- 6Head-to-head comparison of the new calcimimetic agent evocalcet with cinacalcet in Japanese hemodialysis patients with secondary hyperparathyroidism Kidney Int Fukagawa M Shimazaki R Akizawa T 8188259420183004947310.1016/j.kint.2018.05.013 · doi ↗ · pubmed ↗
- 7Clinical practice guideline for the management of chronic kidney disease-mineral and bone disorder Ther Apher Dial Fukagawa M Yokoyama K Koiwa F 2472881720132373514210.1111/1744-9987.12058 · doi ↗ · pubmed ↗
- 8Cinacalcet effectively reduces parathyroid hormone secretion and gland volume regardless of pretreatment gland size in patients with secondary hyperparathyroidism Clin J Am Soc Nephrol Komaba H Nakanishi S Fujimori A 23052314520102079825110.2215/CJN.02110310 PMC 2994093 · doi ↗ · pubmed ↗