Evaluation of prognostic factors for mortality in cancer patients with sepsis in the intensive care unit: systematic review protocol
María Fernanda García-Aguilera, Nayely García-Méndez, Glenn Hernández, Borja M. Fernández-Félix, Harold Alexander-León, Yunqi Yu-Liu, Josue Rivadeneira, Luis Fuenmayor-González, Cristopher Isaac Peña Robayo, Fernanda Villalba, Eduardo Andrés Aragundi Palacios

TL;DR
This study outlines a protocol to identify factors affecting mortality in cancer patients with sepsis in the ICU.
Contribution
The paper introduces a systematic review protocol focused on prognostic factors for mortality in cancer patients with sepsis.
Findings
The review will assess 28-day mortality as the primary outcome.
A meta-analysis will be conducted to generate pooled estimates for identified prognostic factors.
The GRADE approach will evaluate the quality of evidence and strength of recommendations.
Abstract
This systematic review outlines a comprehensive approach to identify and analyze prognostic factors associated with mortality in adult cancer patients with sepsis in the intensive care unit. The review will focus on all-cause 28-day mortality, and where not available, we will use 30-day, intensive care unit, or in-hospital mortality. We present a protocol for the systematic review of prognostic factors for mortality in adult cancer patients with sepsis managed in the intensive care unit. Our primary outcome is 28-day mortality, and where not available, we will use 30-day, intensive care unit, or in-hospital mortality. The secondary outcome is the global mortality incidence. Studies on the basis of the population (sepsis and neoplasms), prognostic study methods and outcome of interest (mortality) will be included. We will search the following databases: Medline, PubMed, EMBASE, SCOPUS,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
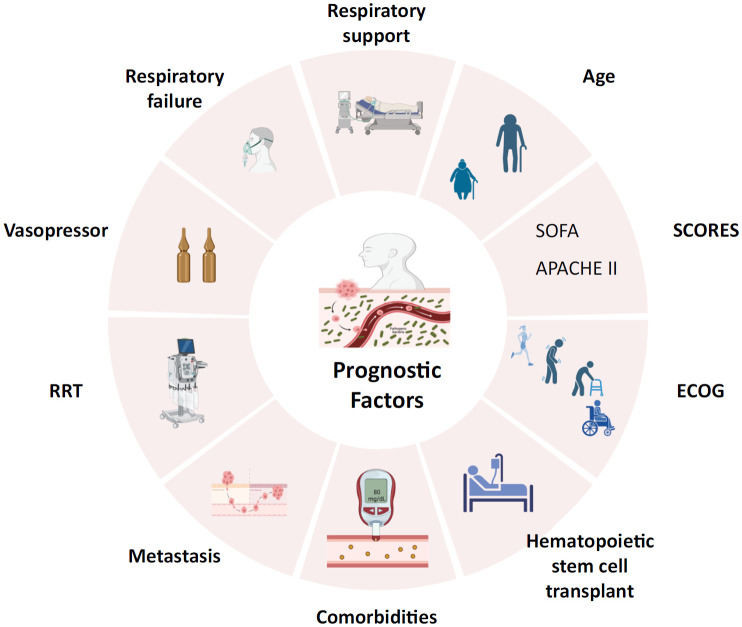 Figure 1
Figure 1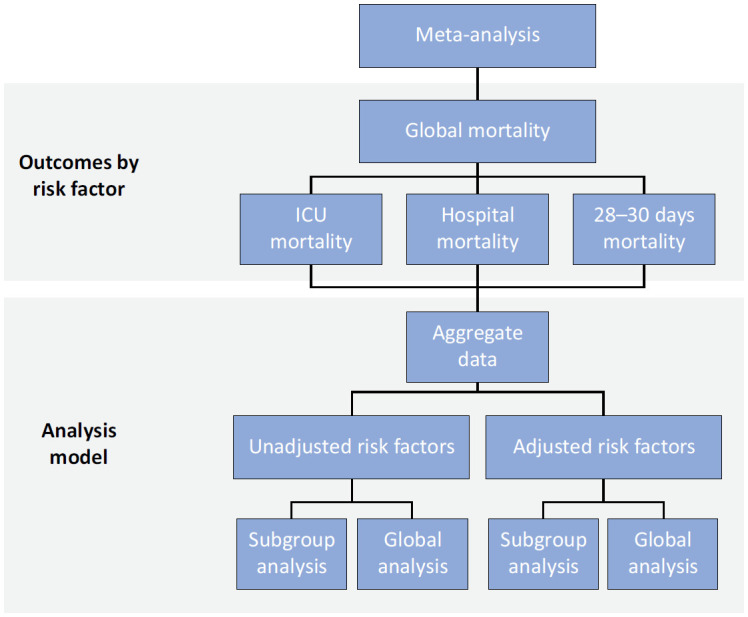 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSepsis Diagnosis and Treatment · Meta-analysis and systematic reviews · Hemodynamic Monitoring and Therapy
INTRODUCTION
The sustained increase in cancer incidence globally poses significant challenges, not only in the management of cancer itself but also in the management of associated severe complications such as sepsis, which is especially prevalent and fatal in this patient population.^(1,2)^ Medical advances have improved cancer survival; however, susceptibility to severe infections such as sepsis remains high due to the immunosuppression induced by the oncological disease and its treatments.^(2-4)^
Cancer patients develop sepsis at an alarming rate and are more likely to be admitted to intensive care units (ICUs), which are associated with high mortality rates.^(2)^ This not only represents a clinical problem but also a considerable economic burden for health systems owing to the extensive resources these patients require.^(5)^
Given this context, it is essential to identify and improve the understanding of the risk factors that contribute to mortality in adult cancer patients with sepsis in the ICU for the future development of strategies that will enhance outcomes and reduce mortality rates. Previous studies have suggested that patient-related and clinical management factors significantly influence outcomes.^(6,7)^ However, variability in study designs and methodological quality has prevented definitive conclusions, highlighting the need for a rigorous and structured systematic review that consolidates and critically evaluates the existing evidence.
METHODOLOGY
Record
The protocol has been registered in accordance with the recommendations of the protocol statement of the Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) in the International Prospective Register of Systematic Reviews (PROSPERO) on November 23, 2023.^(8)^ The systematic review will be reported following the PRISMA initiative.^(9)^
Eligibility criteria
Type of study
Experimental and observational studies that report prognostic/risk factors for mortality in adult cancer patients with sepsis and septic shock treated in the ICU will be included.
Types of participants
For a study to be eligible, participants must be adults 18 years of age and older with a diagnosis of cancer and sepsis admitted to the ICU. The study will be required to include information from studies that have reported information on any of the main outcomes of ICU, hospital or 28–30-day mortality. We will include studies published from 2004 onward and perform a stratified meta-analysis by decade to evaluate differences in outcomes between studies published in the first decade (2004 - 2013) and second decade (2014-2024). The definitions of Sepsis-1, Sepsis-2, and Sepsis-3 will be accepted, as well as the definitions provided by the International Classification of Diseases and the Centers for Disease Control and Prevention (CDC).^(10-13)^
Types of outcomes
Primary outcomes
Our primary outcome is 28-day mortality, and where not available, we will use 30-day, ICU, or in-hospital mortality.
Secondary outcomes
Global mortality incidence (the most extended follow-up provided by the study authors).
Information sources
The following databases will be searched:
MEDLINEEMBASEWeb of Science (WoS)ScopusBireme-BVS
Types of prognostic factors
We will include all studies that evaluate any prognostic factors for mortality, and the associations between the detected prognostic factors and the outcomes of patients with sepsis in the ICU will subsequently be assessed.
Core adjustment set
We will assess the role of the identified factors after adjustment for additional covariables. After a consensus among experts, studies will be considered if they have adjusted for at least one of the following factors: 1) sex; 2) age; 3) type of tumor (locoregional solid tumor, metastatic solid tumor, or hematological); 4) severity score (severity score; Sequential Organ Failure Assessment score [SOFA], Eastern Cooperative Oncology Group [ECOG]); 5) comorbidities (type 2 diabetes mellitus, chronic heart failure, chronic pulmonary disease [COPD]; 6) support in the ICU (ventilator support, use of vasopressor, renal replacement therapy, hospital origin, transfusions, chemotherapy); 7) complications (neutropenia, atrial fibrillation, acute renal failure, infections due to viruses, bacteria, fungi and parasites, and respiratory failure); and 8) hematopoietic stem cell transplant (HSCT), recipients for a more accurate mortality assessment than other HSCT types or nontransplanted individuals^(14-16)^ (Figure 1). If new evidence is found, these parameters will be modified.
Prognostic factors of mortality in cancer patients with sepsis in the intensive care unit.
Search methods
The search strategy will be based on terms related to populations (sepsis; neoplasms), prognostic factor (prognostic factors), outcome (mortality), and predictive study methods,^(17)^ without time and language limits.
Study data management
We will remove duplicate articles and select articles using the Covidence program, followed by manual cross-checking.^(18)^ The resulting unique references will be manually filtered for additional duplicate checking. The nonduplicated data will then be selected to construct the data extraction drafts and extracted.
Study selection and data collection
Two of the researchers will independently review the documents in Covidence according to best practice guidelines to evaluate the inclusion criteria. If there are discrepancies, a third researcher will resolve them. The inclusion criteria will be assessed in a sample of studies to ensure reproducibility. Two researchers will independently extract the data via a predefined form, and a third researcher will resolve any discrepancies. Three studies will be piloted on the data extraction template to ensure suitability. The results will be compared, and a third researcher will resolve any discrepancies.
Data elements
The checklist for critical appraisal and data extraction for systematic reviews of prediction modeling studies for prognostic factor (CHARMS-PF) will be used for critical evaluations and data extraction.^(19,20)^ For each eligible study, we will extract the following data:
General information: author, publication date, number of patients, place (country), and financing of the studies includedSource of data: prospective or retrospective designThe authors’ definitions of "sepsis" and "septic shock"Participant characteristics: clinical and demographic data, eligibility criteria and recruitment criteriaOutcome(s): type of mortality (ICU, hospitalization, and/or at 28 – 30 days), definition and timingMissing data, if applicable: number of participants with missing data on outcome and prognostic factors and methods applied for handling missing dataStatistical analysis: logistic regression model, Cox regression model, machine learning, neural networks, or other methodsPrognostic factor selection: a method to select prognostic factors (all prognostic factors on the basis of prior knowledge or on the basis of univariable associations)Confounder factor selection: method for selecting adjustment confounders: prespecified model, retrospective elimination, prospective selection, horizontal selection, LASSO-based selection, ridge-type regression, or bootstrap-type selectionEstimates reported between the prognostic factor and each outcome: (1) unadjusted estimate: association between sepsis prognostic factors and mortality without any covariate; (2) adjusted approaches: associations between and mortality with at least one covariate from the selected core setType of measure of association: odds ratio (OR)
Assessment of methodological quality and risk of bias
To evaluate the quality and biases of the original articles, the Cochrane methodology and QUality In Prognostic Studies (QUIPS) tool will be used,^(21,22)^ considering that the format is accepted as one of the most precise and useful tools for systematic reviews.^(23,24)^ The domains of the QUIPS will be evaluated independently by two authors, and in the case of discrepancy, they will be resolved by a third author. The selection of studies by inclusion and content evaluation will be conducted with clear, predefined criteria through systematic data collection. Studies will be independently examined on the basis of a set of preestablished criteria to establish the validity of the study.
Data synthesis
For each study and prognostic factor, we will extract the measures of association (overall mortality, ICU, hospital, and 28–30-day mortality) together with their confidence intervals (CIs) or standard errors (SEs). To allow statistical pooling of the estimates, we will transform the measures of association into ORs with 95%CIs. We consider that the association measures and their adjustments may differ from the results. We will develop a set of key-adjusted and unadjusted factors to review each result.
If the adjusted factors match with our groups established for the review, we will proceed with a meta-analysis of the article to penalize the estimates of the results in the evaluation of the risk of bias. If the study presents different estimates for the same result, we will extract the estimation that includes the maximum number of confounding factors. If there are multiple approximations that adjust for the same confounding factors, we will consider only the approximation adjusted for the maximum number of confounding factors to minimize the risk of bias due to confounding factors in the approach. The results of each study will be tabulated using Microsoft Excel V. 16. and the prebuilt CHARMS-PROBAST format.^(21)^
We plan to combine the results from individual studies in a meta-analysis to provide a pooled effect estimate for each prognostic factor and outcome. We will aggregate the data via a DerSimonian-Laird random-effects restricted maximum likelihood (REML) meta‐analysis model providing pooled estimates and Knapp-Hartung 95%CIs, and between-study variance estimates in Stata (Version 18) will be used.^(25)^ If we cannot obtain pooled estimations, we will describe the results in a narrative way.
Finally, the prevalence of mortality will be examined in proportions. We will aggregate the data using a random‐effects model using the inverse Freeman–Tukey transformation. We will carry out subgroup analysis by type of malignancy (solid tumors and hematologic malignancies) and geographical area (i.e., continent) (Figure 2).
Analysis model.
Heterogeneity between studies
Heterogeneity will be examined when there are at least two articles, and the prediction interval will be calculated to report the variation in effects between populations.
Sensitivity analysis
Through sensitivity analysis, the robustness and stability of the results obtained will be evaluated against the methodology and study inclusion criteria. This analysis will also help identify potential biases and the influence of individual studies on generalizable conclusions.
The sensitivity analysis will exclude studies that present a high risk of bias, according to the criteria established in the "Quality Assessment of Studies" section. This will allow us to determine whether studies with lower methodological quality significantly affect the results of the meta-analysis so that they can be excluded according to quality.
Sensitivity analyses will be considered within specific subgroups (e.g., cancer type, patient age) to examine whether these variables may influence the relationship between prognostic factors and mortality in this population. This is to identify whether the associations vary significantly between different population groups or according to different conditions.
Publication bias
To detect the presence of publication bias in our review, the funnel plot method will be used, where the effect sizes of individual studies will be plotted against their precision (inverse standard error). An asymmetric distribution of research in the graph will suggest the possible existence of publication bias.
We will complement the graphical analysis with statistical tests, including the Egger test to evaluate asymmetry in the funnel plot through an intercept regression and the Begg test for the correlation between the ranges of estimated effects and their variances.^(26)^ A significant result in these tests will indicate a possible presence of publication bias.
If publication bias is detected, we will apply adjustment techniques such as the "trim and fill" method, which estimates the number of missing studies in the funnel plot and adds them to correct the estimated combined effect. This method will help provide a tighter estimate of the true effect, considering publication bias.
We will evaluate the limitations that publication bias could impose on the interpretation of our findings. To ensure that users of our systematic review understand the potential influence of publication bias on the confidence and applicability of the results.
Confidence in cumulative evidence
We will apply the Grading, Development and Evaluation of Recommendations (GRADE) approach^(27)^ and present each main result in a table, following the principles of Hughes et al. for prognostic questions, considering that the GRADE approach has been widely used to evaluate the certainty of evidence for prognostic factors.^(28)^
Patient and public participation
The public and patients will not participate in this systematic review.
Dissemination and ethics
Approval from an ethics committee is not required when summarizing already published data. The study will be coordinated by the Universidad Central del Ecuador, Hospital Oncológico SOLCA, Núcleo de Quito—Research Department. We will publish and disseminate our results through a peer-reviewed indexed journal, at conferences, and in the media.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Sung H Ferlay J Siegel R Laversanne M Soerjomataram I Jernal A Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries CA Cancer J Clin 20217132092493353833810.3322/caac.21660 · doi ↗ · pubmed ↗
- 2Cecconi M Evans L Levy M Rhodes A Sepsis and septic shock Lancet 2018392101475872993719210.1016/S 0140-6736(18)30696-2 · doi ↗ · pubmed ↗
- 3National Cancer Institute (NIH) Cancer Trends Progress Report. Mortality. NIH Online Summary of Trends in US Cancer Control Measures Bethesda NIH 2024 cited 2025 Feb 25Available from: https://progressreport.cancer.gov/end/mortality
- 4Siegel RL Miller KD Wagle NS Jemal A Cancer statistics, 2023 CA Cancer J Clin 202373117483663352510.3322/caac.21763 · doi ↗ · pubmed ↗
- 5Bradley CJ Yabroff KR Dahman B Feuer EJ Mariotto A Brown ML Productivity costs of cancer mortality in the United States: 2000-2020 J Natl Cancer Inst 200810024176317701906627310.1093/jnci/djn 384PMC 2720777 · doi ↗ · pubmed ↗
- 6Zugazagoitia J Guedes C Ponce S Ferrer I Molina-Pinelo S Paz-Ares L Current Challenges in Cancer Treatment Clin Ther 2016387155115662715800910.1016/j.clinthera.2016.03.026 · doi ↗ · pubmed ↗
- 7Santucci C Carioli G Bertuccio P Malvezzi M Pastorino U Boffetta P Progress in cancer mortality, incidence, and survival: a global overview Eur J Cancer Prev 20202953673813274016210.1097/CEJ.0000000000000594 · doi ↗ · pubmed ↗
- 8Shamseer L Moher D Clarke M Ghersi D Liberati A Petticrew M Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015: elaboration and explanation BMJ 2015350 g 7647 g 76472555585510.1136/bmj.g 7647 · doi ↗ · pubmed ↗