CoVimmune COVID-19 Immunity Calculator: Web Application Development and Validation Study
Rebecca Slotkin, Tassos C Kyriakides, Vinni Yu, Xien Chen, Anupam Kundu, Shaili Gupta

TL;DR
A web app was developed to estimate SARS-CoV-2 neutralizing antibody levels based on IgG test results, helping assess vaccine-induced immunity.
Contribution
A novel web-based calculator was developed to translate IgG test results into estimated neutralizing antibody titers for vaccinated individuals.
Findings
The web application uses datasets to correlate IgG and neutralizing antibody titers in vaccinated adults.
The tool incorporates statistically significant clinical factors to improve nAb titer prediction accuracy.
The calculator provides a patient-centered estimate of vaccine-mediated antibody protection.
Abstract
This study illustrates the development of a simple web-based application, which demonstrates the relationship between serum anti-SARS-CoV-2 S1/receptor-binding domain immunoglobulin G (IgG) and anti-SARS-CoV-2 neutralizing antibody (nAb) half-maximal inhibitory concentration (IC50) titers in a vaccinated US adult population and compares them to prior data on nAb titers at different time points after vaccination. The objective of this study is to create an easily accessible calculator that uses the results of commercially available anti-SARS-CoV-2 serum IgG to approximate the underlying ability to neutralize SARS-CoV-2. Our web-based application leveraged two previously published datasets. One dataset demonstrated a robust correlation between nAb and serum IgG. The other dataset measured nAb titers at specific time periods over a year-long interval following a messenger RNA vaccination…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
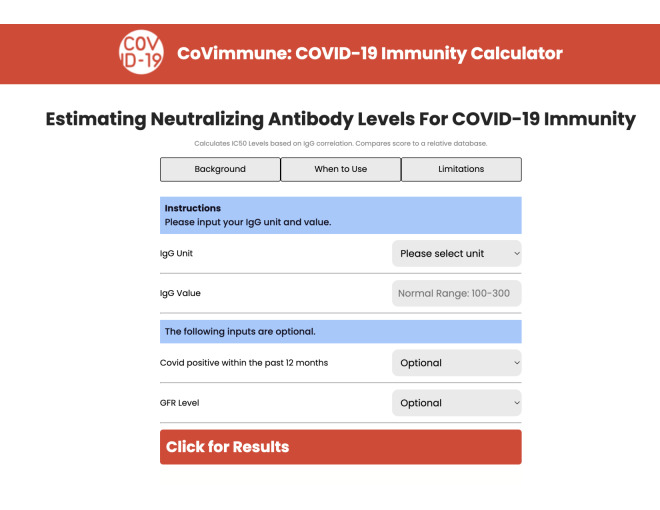 Figure 1
Figure 1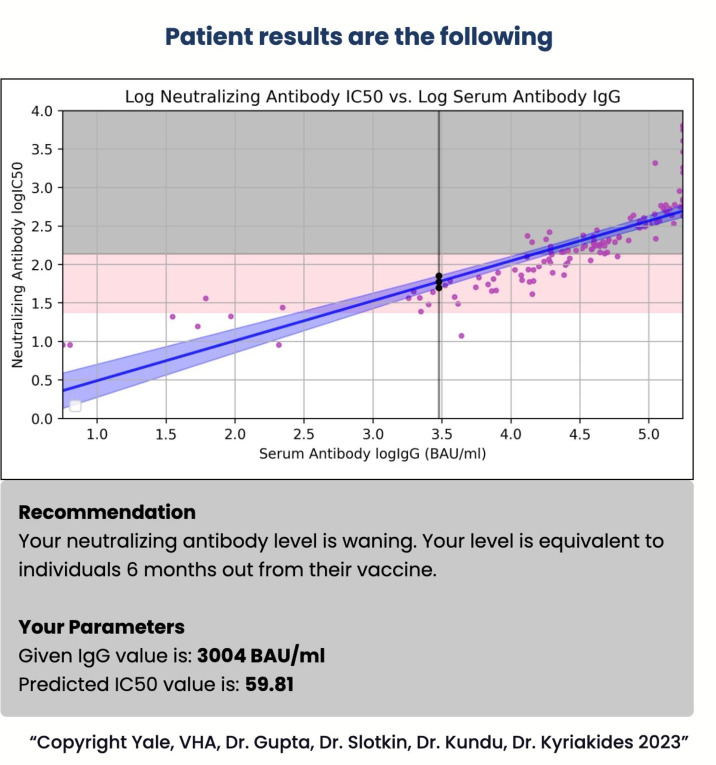 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSARS-CoV-2 and COVID-19 Research · COVID-19 Clinical Research Studies · vaccines and immunoinformatics approaches
Introduction
High levels of anti-SARS-CoV-2 neutralizing antibodies (nAbs) have been shown to be protective against severe SARS-CoV-2 infection [1], but nAbs wane over time following vaccination or infection [23]. In addition, nAbs require significant funding and infrastructure to measure and are largely limited to research settings. Serum anti-SARS-CoV-2 immunoglobulin G (IgG) testing is available in commercial settings at relatively low cost. IgG testing has been sporadically ordered in primary care settings; although, there has been little to guide its clinical interpretation [45].
Methods
Ethical Considerations
Approval for the study from which both datasets were derived (SARS-CoV-2 Vaccine and You, protocol #1599488) was obtained from the Veterans Affairs Connecticut Healthcare System Institutional Review Board (IRB) in December 2020. Participants were eligible for inclusion if they were veterans or health care workers at the Veterans Affairs Connecticut Healthcare System and excluded if they were unable to provide informed consent. Written informed consent was obtained from willing participants prior to study participation and they were aware they could opt out at any time. The ethics approval covered secondary analysis as done for this paper without additional consent. Samples were donated by participants without any compensation and we are immensely grateful for this. All identifiable subject data was secured in encrypted folders accessible only to IRB-approved investigators. All data was de-identified before serological analysis.
Source Data Sets
The first dataset was derived from a prospective cohort study which measured anti-SARS-COV-2 nAb half-maximal inhibitory concentration (IC50) titers against pseudotyped WA-1 (the original SARS-CoV-2 strain) at specific time periods over a year-long interval following the primary messenger RNA vaccination series and a subsequent booster vaccine dose (before dose 1, before dose 2, and after dose 2 at 1, 3, 6, and 12 months, with an additional collection 1 month after dose 3, which was approximately 10 months after dose 2). Clinical variables were collected by manual chart review as previously described. The nAb titers were found to fluctuate over time, peaking 1 month after the primary series, waning at 6 months, and rising again 1 month after the booster dose [2].
The second dataset leveraged the collected serum samples and measured IgG anti-S1/receptor-binding domain values in sera with predetermined nAb titers and clinical variables as previously described [6]. IgG and nAb IC50 titers had a robust linear correlation. Multimedia Appendix 1 illustrates this correlation for each clinical variable (COVID-19 infection status, estimated glomerular filtration rate (GFR), age, sex, history of malignancy, and race). Based on a forward stepwise linear regression, GFR (0‐30, 31‐59, and >60 mL/min/1.73 m²), and history of COVID-19 infection within the past 12 months (yes or no) were found to impact this correlation (R^2^=0.78) [6].
The model had undergone internal validation using repeated k-fold cross-validation. The model’s performance was evaluated using root mean squared error (RMSE), R^2^, and mean absolute error (MAE) across multiple versions of the model and different crossvalidation setups (ten 10-fold repeats, five 10-fold repeats, and three 5-fold repeats). For our model, which included IgG, COVID-19 infection status, and GFR, the RMSE was relatively low (around 0.27‐0.28) across validation setups, suggesting a small average error between the predicted and actual values. The R^2^ values were around 0.77 to 0.81 across validation setups, which indicated that the model explained about 77% to 81% of the variability in the data. The MAE values were around 0.2 for all validation setups, demonstrating a low average error magnitude (Multimedia Appendix 2).
Application Development
Backend (Software)
The application used the model-view-controller pattern. We initially used RStudio 2023.12.1+402 running R 4.3.2 (IBM Corp) and an integrated development environment with a set of tools to complement R. The original R script had initially used its own web application framework (Shiny) to create a local web-based application, but this framework was not compatible with the rest of the tools used in the development process. The R script was converted to Python 3.9.12 (Python Software Foundation) for ease of web development. The main challenge when developing the project was converting the original R script into Python and creating the website using an HTML and cascading style sheets (CSS). Python was chosen over R for several reasons. First, Python’s versatility and ecosystem made integration with other tools like Flask, a popular web framework that simplifies the web application development process, and Docker, which simplifies the process of containerizing applications, much easier. Second, Python’s versatility and rich ecosystem of libraries and web development tools allowed us to keep the backend and front end the same language. Third, Python could handle a high volume of web requests and was better suited for scalable applications, which was a point of consideration. Last, Python was also the better choice for long-term maintainability, as it is more readable and easier to update. The host server emphasized Docker as the primary tool for deployment, making it the easiest tool to use for the development process. The full source code is available on request.
Front End (Web Interface)
The front end was converted from a Shiny package in RStudio to an HTML and CSS. The Python Flask 3.0.0 (Armin Ronacher) module was used to build the CoVimmune website. The website was launched using a YaleInformation Technology Support secured self-service sandbox environment called Spinup. The Waitress Web Server Gateway Interface was used to deploy our application and Docker 4.27.1 (Docker, Inc) was used to package, ship, and run our application.
Results
This web-based application was based on 127 sera samples in 100 unique participants aged 20‐93 years (mean 63.83, SD 15.63 years; 29% female; 67% White) from the second dataset. The user can input their IgG value, and the units can be from any of 4 commonly used platforms (Abbott-arbitrary U/ml, Siemens-U/ml, Roche-U/ml, and Euroimmune-relative U/ml) or the World Health Organization’s standardized IgG value in binding antibody U/mL. The user can choose to select their COVID-19 infection status and GFR category from drop down lists. The application then generates an estimated nAb titer, which is compared to individuals with matching renal function and COVID-19 status from the first dataset, to provide a contextualized range of nAb titers at different time points after vaccination (Figure 1 and Figure 2). The application also visualizes the results in the context of time from the last vaccination among individuals with similar values in the application dataset. The application is free and available on the internet [7].
CoVimmune COVID-19 immunity calculator website interface for the application. GFR: glomerular filtration rate; IC50: half-maximal inhibitory concentration; IgG: immunoglobulin G.
CoVimmune COVID-19 immunity calculator results with an example input. BAU: binding antibody unit; IC50: half-maximal inhibitory concentration; IgG: immunoglobulin G.
Discussion
The application illustrates the relationship between serum anti-SARS-CoV-2 IgG and anti-SARS-CoV-2 nAb IC50 titers in a vaccinated US adult population and allows for the adjustment of that relationship based on renal function and prior COVID-19 infection. It brings bench research into the clinical context and may provide a tool for physicians to personalize discussions about vaccine booster timing for patients where yearly vaccination may not be appropriate [8] or for those who are hesitant to get revaccinated.
This application is not intended to replace clinical judgment or offer conclusions about immune protection from COVID-19 or vaccine efficacy. The nAb titers are only one component of the immune response to infection. We cannot extrapolate cellular immunity from these data. This application is based on a small sample of patients and there were limited numbers of immunocompromised individuals within the sample, which may have limited generalizability to those individuals [9]. Ultimately, this application is a user-friendly example of how SARS-CoV-2 IgG nAb vaccine research, which has high barriers to replication and clinical application due to cost and infrastructure requirements, can be transformed into a practical tool.
Supplementary material
10.2196/59467Multimedia Appendix 1Correlation between the log immunoglobulin G values and the log half-maximal inhibitory concentration titers by clinical variable.
10.2196/59467Multimedia Appendix 2Repeated k-fold cross validation results.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Khoury DS Cromer D Reynaldi A et al Neutralizing antibody levels are highly predictive of immune protection from symptomatic SARS-Co V-2 infection Nat Med 07202127712051211 doi 10.1038/s 41591-021-01377-8Medline 34002089 · doi ↗ · pubmed ↗
- 2Zhao M Slotkin R Sheth AH et al Serum neutralizing antibody titers 12 months after coronavirus disease 2019 messenger RNA vaccination: correlation to clinical variables in an adult, US population Clin Infect Dis Feb 82023763 e 391e 399doi 10.1093/cid/ciac 416Medline 35639598 PMC 9278145 · doi ↗ · pubmed ↗
- 3Link-Gelles R Weber ZA Reese SE et al Estimates of bivalent m RNA vaccine durability in preventing COVID-19-associated hospitalization and critical illness among adults with and without immunocompromising conditions - VISION Network, September 2022-April 2023 MMWR Morb Mortal Wkly Rep 052620237221579588 doi 10.15585/mmwr.mm 7221 a 3Medline 37227984 PMC 10231940 · doi ↗ · pubmed ↗
- 4Wiencek JR Head CL Sifri CD Parsons AS Clinical ordering practices of the SARS-Co V-2 antibody test at a large academic medical center Open Forum Infect Dis Oct 2020710 faa 406doi 10.1093/ofid/ofaa 406Medline 33072813 PMC 7553244 · doi ↗ · pubmed ↗
- 5Zarif A Mc Gagh D Hoang U de Lusignan S The role of antibody tests for COVID-19 in primary care Br J Gen Pract 202171704131134 doi 10.3399/bjgp 21X 715169 Medline 33632693 PMC 7909929 · doi ↗ · pubmed ↗
- 6Slotkin R Kyriakides TC Kundu A Stack G Sutton RE Gupta S Correlation of a commercial platform’s results with post-vaccination SARS-Co V-2 neutralizing antibody response and clinical host factors P Lo S ONE 2023188 e 0289713 doi 10.1371/journal.pone.0289713 Medline 37643190 PMC 10464955 · doi ↗ · pubmed ↗
- 7Estimating neutralizing antibody levels for COVID-19 immunity Co Vimmune: COVID-19 Immunity Calculator UR Lhttps://covimmune.yale.edu/Accessed 02-04-2024
- 8Townsend JP Hassler HB Dornburg A Infection by SARS-Co V-2 with alternate frequencies of m RNA vaccine boosting J Med Virol Feb 2023952 e 28461 doi 10.1002/jmv.28461 Medline 36602045 · doi ↗ · pubmed ↗