Primiparity, class 3 obesity, intention to breastfeed and breastfeeding initiation
Leandro Cordero, Michael R. Stenger, Bradley J. Needleman, Sabrena Noria, Mark B. Landon, Craig A. Nankervis

TL;DR
The study finds that primiparous women with class 3 obesity who intended to breastfeed faced significant maternal and neonatal health challenges that often prevented them from initiating breastfeeding.
Contribution
This study identifies specific perinatal variables that hinder breastfeeding initiation in primiparous women with class 3 obesity.
Findings
Exclusive breastfeeding was achieved by 38% of women who intended to breastfeed only.
Maternal and neonatal morbidities like preeclampsia and NICU admission were strong predictors of breastfeeding failure.
African American women and those on public healthcare were more likely to switch to formula feeding.
Abstract
During the 2013–21 period, 674 primiparous women with Class 3 obesity delivered in our institution. Their antenatal infant feeding preference on admission was: 518 (77%) intended to breastfeed (BF) only, 101 (15%) intended to feed formula only and 55 (8%) intended to BF and formula feed combined. Intention to BF only is a predictor of BF initiation, however, data concerning this relationship is limited. To determine the perinatal variables that influence success or failure of BF among primiparous women with Class 3 obesity who antenatally declared their intention to only BF. Retrospective cohort study of women who delivered live singletons without major malformations at ≥ 34 weeks gestation. The 518 women who prenatally intended to BF only, were categorized at discharge as exclusive BF (EBF) 197 (38%), any BF (ABF) 212 (41%) and formula feeding (FF) 109 (21%). A lower prevalence of…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
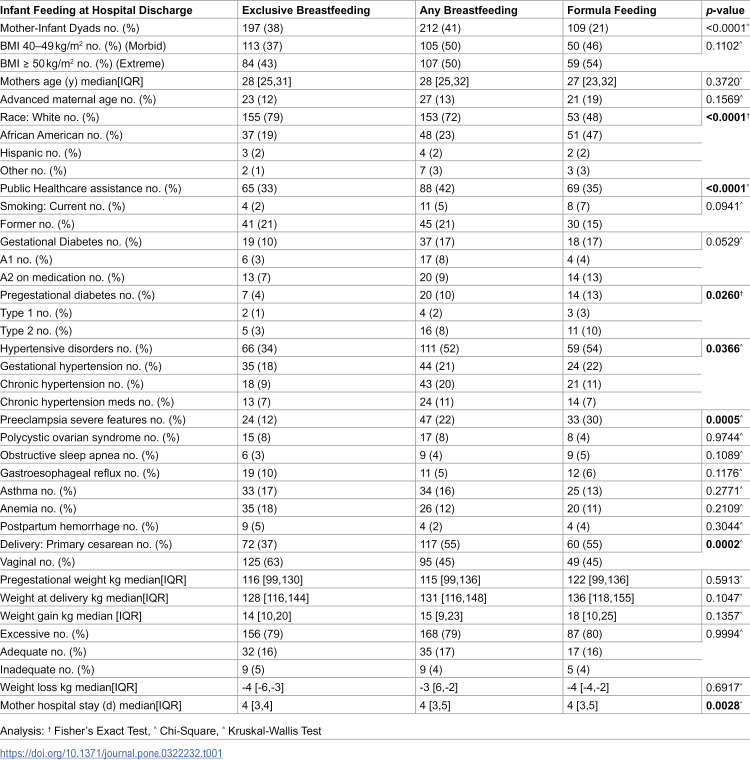 Figure 1
Figure 1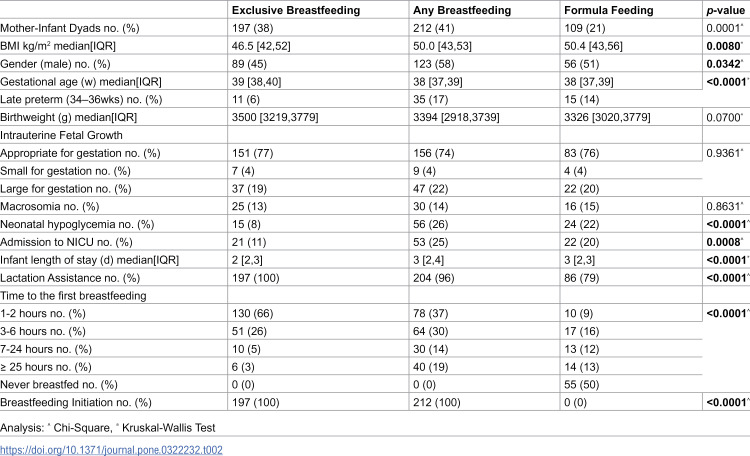 Figure 2
Figure 2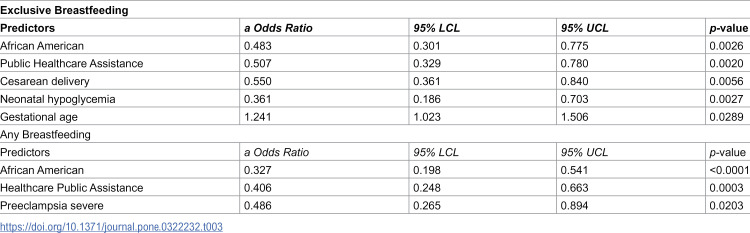 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBreastfeeding Practices and Influences · Gestational Diabetes Research and Management · Maternal Mental Health During Pregnancy and Postpartum
Background
Obesity is the most common medical condition that affects women of reproductive age across the world [1–3]. The prevalence of obesity among women 20–39 years of age increased from 29.8% in 2001–2002 to 39.7% in 2017–2018 [1]. The benefits of lactation on short and long term maternal and infant health have been clearly documented [4–6]. Specifically, exclusive breastfeeding (EBF) or any breastfeeding (ABF) during birth hospitalization and through the first postpartum year are important for both healthy women as well as for those with comorbidities [6–10]. Few studies on perinatal outcomes including BF for women with Class 3 obesity (pregestational body mass index (BMI) 40–49 kg/m^2^ morbid and ≥ 50 kg/m^2^ extreme) have been reported [11–13]. Recently, an inverse relationship between BMI and ABF has been established [14]. Intention to BF only is a strong predictor, although not absolute, of BF success, however, there is limited information on the proportional rates of EBF, ABF or formula feeding (FF) at discharge among primiparous women with Class 3 obesity [10,13].
A positive BF experience for a woman, primiparous or multiparous, will improve her chances for success in the next pregnancy, however an unsuccessful experience will lower the probability of BF subsequent infants [15]. Considering the above, it is important to identify the obstacles that lead to BF failure in primiparous women with Class 3 obesity who intended to BF only.
Objective
To determine perinatal variables that may influence the achievement of EBF and ABF among 518 primiparous women with Class 3 obesity who declared prenatally their intention to BF only.
Subjects and methods
This retrospective study of medical records was approved by the Biomedical Sciences Institutional Review Board of The Ohio State University (IRB 2010H0198) with waivers of informed consent and HIPAA research authorization, in accordance with the relevant guidelines and regulations of the declaration of Helsinki. The de-identified and coded data from electronic maternal and neonatal records (2013–2021) were reviewed. According to their pregestational BMI, women were classified as normal (BMI 18.5–24.9 kg/m^2^), overweight (BMI 25–29.9 kg/m^2^), obese Class 1 (BMI 30–34.9 kg/m^2^), Class 2 (BMI 35–39.9 kg/m^2^) or Class 3 (divided into morbid obesity BMI 40–49 and extreme obesity ≥ 50 kg/m^2^) [2,14]. The study population was composed of women with Class 3 obesity who delivered at ≥ 34 weeks of gestation singleton live births without major malformations. Infants born between 34 and 36 6/7 weeks were considered late prematures.
During their prenatal care visits, on arrival to Labor and Delivery and shortly after delivery, women were asked about their anticipated infant feeding preference (BF only, BF and FF combined or FF only) [10,13]. Gestational diabetes mellitus (GDM), Type 1 and Type 2 DM, chronic hypertension (CHTN), severe preeclampsia, anemia, polycystic ovary syndrome (PCOS), obstructive sleep apnea (OSA) and gastroesophageal reflux disease (GERD) were diagnosed and treated following established guidelines [16–18]. Gestational weight gain (GWG) was categorized as adequate, inadequate or excessive [19]. Clinical and demographic data from some women included in this investigation have been reported earlier [10,13,20].
Women were also informed of our hospital practices that encourage BF including early BF and formula supplementation only if medically indicated, rooming in and availability of full-time lactation consultants and post discharge BF support [10,13,20,21]. As required for hospital accreditation, our institution reports BF data to the Joint Commission [7].
Following delivery, symptomatic infants were transferred directly to the neonatal intensive care unit (NICU) for further care. Holding, skin-to-skin contact, and BF were encouraged depending on the mother-infant dyad condition. Asymptomatic infants able to feed were taken to the Newborn Nursery for routine care and glucose monitoring if indicated [10,13,20,21]. Using intrauterine growth charts, infants were identified as appropriate for gestational age (AGA), small (SGA), large (LGA) or macrosomic (birthweight ≥ 4000g) [10,13,20,21].
If indicated, blood glucose was assessed with Accu-Chek^®^ or by plasma glucose measurements starting during the first hour of life. Neonatal hypoglycemia was defined by blood glucose of < 40 mg/dl before 4 hours of life and by < 45 mg/dl thereafter. Infants with hypoglycemia were treated with glucose gel, BF or formula feeding and those with persistent hypoglycemia were transferred to the NICU for further care [10,13,20,21]. EBF was defined as direct feedings from the breast, expressed breast milk or donor human milk (DHM) [10,13,20,21]. ABF consisted of direct BF, expressed breast milk or DHM supplemented with formula [10,13,20,21]. BF was considered initiated if, during the 24 hours preceding hospital discharge, infants were EBF or ABF [10,13,20,21]. Due to the study design, information on post-discharge infant feeding was not available.
Statistical analysis
Comparisons of BF outcomes (EBF, ABF or FF) were made with T-Tests for continuous variables following a normal distribution, and Wilcoxon Two-Sample tests for continuous variables that were not normally distributed. Chi-square analysis was used for categorical variables. Multivariate logistic regressions were used to determine the probability of BF initiation and the probability of EBF at discharge. Explanatory variables in both logistic models included BMI, DM, CHTN, race, healthcare public assistance, mode of delivery, infant feeding intention, fetal growth, preeclampsia, late prematurity, macrosomia, hypoglycemia, and admission to the NICU. Logistic models used backward elimination method for predictor selection, although forward and stepwise selection methods produced the same results. Significance was established at a p-value < 0.05. Analyses were performed with SAS version 9.4 (Cary, NC).
Results
Perinatal outcomes of women who intended to BF only
The study population was composed of 518 primiparous women with Class 3 obesity who prenatally declared their intention to BF only. Based on infant feeding at discharge, the 518 mother-infant dyads were divided into EBF (38%), ABF (41%) and FF (21%) (Table 1). The three groups were similar in age at delivery and current and former smoking combined but were different in rate of advanced maternal age, white race and public healthcare assistance.
Table 1: Perinatal outcomes of women who intended to breastfeed only.
The rate of GDM (A1 combined with A2) was lower in the EBF group than in the other 2 groups (10,17 vs 17%) and Type 2 DM was also lower (3,8 vs 10%). CHTN with and without medication combined was higher in the ABF (31%) than in the other two groups (16 vs 18%). Severe preeclampsia was less prevalent in the EBF group (12,22 vs 30%), however, it was superimposed on diabetes mellitus in 25% of the EBF, 43% of the ABF and 42% of the FF group. Concurrently, preeclampsia was also superimposed on CHTN in 33% of EBF, 53% of ABF and 45% of FF group. Equally prevalent were OSA (3,4 vs 5%), PCOS (8,8 vs 4%), GERD (10,5 vs 6%), asthma (17,16 vs 13%) and anemia (18,12 vs 11%).
Vaginal delivery was more frequent in the EBF group (63,45 vs 45%) while primary cesarean was more common in the ABF and FF groups (37,55 vs 55%). Median pregestational weight (116,115 vs 122 kg), median weight at delivery (128,131 vs 136 kg) and rate of excessive (79,79 vs 80%), adequate (16,17 vs 16%) and inadequate GWG (5,4 vs 4%) were similar in all groups.
Neonatal outcomes in the exclusive, any breastfeeding and formula feeding groups
Infants born to the 197 women from the EBF, 212 infants from the ABF and 109 from the FF group were comparable in male gender (45,58 vs 51%), median birth weight (3500,3394 vs 3326g), AGA (77,74 vs 76%), LGA (19,22 vs 20%) and SGA (4,4 vs 4%), but differed in median GA (39,38 vs 38w), late prematurity (6,17 vs 14%), hypoglycemia (8,26 vs 22%), admission to the NICU (11,25 vs 20%), and infant length of stay (2,3 vs 3d) (Table 2).
Table 2: Neonatal outcomes in the exclusive, any breastfeeding and formula feeding groups.
Of the 96 infants admitted to the NICU, two thirds were transported directly from the delivery room while the other third remained with their mothers briefly before transfer. Considering the similarities between the three feeding groups, the main NICU admission diagnoses combined were respiratory distress (42%), hypoglycemia (34%), prematurity (19%) and miscellaneous (5%).
Exclusive, partial and formula feeding at discharge
Of the 518 women who intended BF only, 197 (38%) EBF, 212 (41%) ABF and 109 (21%) FF at the time of hospital discharge (Table 2). There were 268 women with morbid (BMI 40–49 kg/m^2^) and 250 others with extreme obesity (BMI ≥ 50 kg/m^2^). The latter was lower in EBF (33 vs 40%) and higher in FF (24 vs 18%), however, these differences were not statistically significant. Lactation support was accepted by every woman in the EBF, by 96% of those in the ABF and by only 79% of those in the FF group. DHM contributed to BF in 22% of the EBF and to 8% of the dyads in the ABF group.
BF during the first 2 hours of life occurred in 66% of infants in the EBF, 37% in the ABF and only in 9% of infants in the FF group. In contrast, among women with severe preeclampsia, BF in the first two hours was recorded in 46% of EBF, 21% for those in ABF and 6% of the FF group. First BF occurred between 3 and 6 hours among 26% of women in the EBF, 30% on the ABF and 16% of the FF group. The remaining women in the EBF, ABF and one half of those in the FF group BF within 48 hours after birth. Unfortunately, the other half of those in the FF group never BF (Table 2). Eleven of the 197 (6%) infants in the EBF group had a formula supplement prescribed during the first 6 hours and 20 (10%) other infants during the first 24 hours. Concurrently, formula supplementation was prescribed within the first 6 hours in 57% of the infants in the ABF and in 77% of those who FF at discharge. In the ABF group on the day of discharge 31 (15%) of the 212 mothers BF three times while 104 (49%) others BF four times or more.
Regression analysis confirmed that race other than white (aOR 0.483 CI 95% 0.301, 0.775), public healthcare assistance (aOR 0.507 CI 95% 0.329, 0.780), and neonatal hypoglycemia (aOR 0.361 CI 95% 0.186, 0.703) were associated with EBF failure (Table 3). Concurrently late prematurity and admission to the NICU were significant obstacles to EBF (Table 2). In contrast, the likelihood of EBF increases with increasing weeks of gestational age (aOR 1.241 CI 95%1.023, 1.506) (Table 3). Regression analysis showed that African American women (aOR 0.327 CI 95% 0.198, 0.541), those who received public healthcare assistance (aOR 0.406 CI 95% 0.248, 0.663) or who had severe preeclampsia (aOR 0.486 CI 95% 0.265, 0.894) were less likely to initiate BF at discharge (Table 3).
Table 3: Logistic regressions for exclusive and any breastfeeding.
Neither iron deficiency anemia, postpartum hemorrhage nor intraoperative bleeding were independent predictors of BF success. Similarly, regardless of infant feeding outcomes, excessive, adequate or inadequate rates of GWG, were not independent predictors of EBF or ABF in this investigation.
Discussion
Maternal preference for feeding their infants after birth included BF only, FF only or BF and FF combined (ABF). Although intention to BF is the preferable choice, it is not always a predictor of BF initiation [10,22–24]. In the past we have consistently reported discordance between intention to BF and achievement of BF outcomes [10,25–29]. The current analysis of 518 primiparous women with Class 3 obesity who intended BF only, showed that the rates of 38% EBF, 41% ABF and 21% FF at discharge are consistent with those we have reported in other high risk obstetrical populations [10,13,20,28,29].
The American Academy of Pediatrics, The Academy of Breastfeeding Medicine and the World Health Organization recommend EBF for all infants during birth hospitalization and beyond [7–8]. As recently as 2019, EBF was reported in the U.S. to be 62.6% at the time of discharge [9]. These rates are indeed quite different from those of 47% for infants born to women with CHTN and severe obesity [27], 37% with severe preeclampsia [13] and 19% with CHTN superimposed on PGDM [28]. Considering the above, the 38% EBF rate reported here for women who intended to BF only although disappointing is not surprising. Conrey et al. suggested that to improve EBF and BF duration one must focus on strengthening BF intention and identify effective interventions to support women with comorbidities and higher pregestational BMI [24].
Antenatal intention to provide BF and FF instead of BF only, at least in our experience, leads to lower rates of EBF and higher rates of ABF and FF at hospital discharge [20,29]. The results of the current study highlight the discordance between intention to BF only and EBF and BF initiation among women with high-risk obstetrical conditions including obesity [27–29]. The experience of 212 women who intended to BF only, but provided ABF at discharge instead could offer, however, a somewhat optimistic perspective since these women were able to BF 66% of their babies within 6 hours from birth and at the time of discharge, 135 (64%) of the infants were still BF up to four times per day. It is also possible that some of these women with support and encouragement could reinitiate and maintain EBF longer [10,20,24].
According to standard definitions, EBF and ABF infants combined represent a BF initiation rate of 79% for the 518 primiparous women with Class 3 obesity who prenatally intended to BF only [7–9]. Furthermore, in subsequent pregnancies these women will acknowledge a prior BF experience. The importance of this information is supported by multiple studies that showed that prior BF experience is a very strong predictor of BF initiation [15,30,31]. In a recent study of multiparous with PGDM we reported intention to BF only in 79% of 170 women with prior experience and in 46% of 134 others without prior BF experience [31]. Concurrently, their BF initiation following the subsequent pregnancy was 81% in the prior BF group and only 36% among those without prior experience [31].
While abundant literature addresses the impact of intention to BF on BF initiation, the reasons why women who intended to BF only succeed or fail are unclear. FF at discharge, by 109 (21%) of women in the current study is concerning because none of them changed their decision even after interactions with lactation consultants [10,13,20,29–31].
Time to the first BF is important because many critical maternal and neonatal physiological interactions occur during the first hour after birth [28,32–34]. In a recent study of infants born to women with PGDM, we reported that rates of EBF and of BF initiation at discharge were similar for infants who BF at birth or during the first six hours while those who BF later had lower rates of either type of BF [10]. The data presented here showed that the time of the first BF strongly associates with EBF at discharge as compared to those infants in the ABF and FF groups. Conversely, FF shortly after birth or during the hospitalization remain a strong predictor of BF initiation failure [35]. While early BF is preferable, maternal complications, neonatal morbidities or maternal-infant separation often preclude or delays BF initiation [21,32,33]. Formula supplementation even when medically indicated is an obstacle to EBF and BF initiation [32–35]. However, parents and health providers should be reminded that temporary formula supplementation needs not to deter resumption or continuation of BF [32–35].
Hypertensive disorders of pregnancy are common complications especially among women with severe obesity [13,26–29]. The data presented here showed a strong association between severe preeclampsia and failure to establish EBF (18%) or ABF (54%) (a OR 0.486 CI 95% 0.265, 0.894). The adverse effects of preeclampsia are also compounded by its severity, by the superimposition of CHTN and DM, by the need for magnesium sulfate treatment or by the often urgency for cesarean delivery [13,18,36,37].
Our data also showed that cesarean delivery was a strong predictor of EBF failure (a OR 0.550 CI 95% 0.361, 0.840). Delays in BF initiation accompanying cesarean delivery are associated with maternal-infant separation, reduced sucking ability and insufficient milk supply, all factors predictive of low BF initiation and shortened BF duration [36–39]. Furthermore, some of these obstacles may be compounded by delayed lactogenesis, especially in women with severe obesity [38]. Regardless of the mechanism, mother-infant separation undoubtedly has an emotional impact on the mother and a likely physiological effect on mother and infant [37–39].
The rate of NICU admission among the ABF and FF groups was higher than in the EBF group. NICU admission has been a global marker of undesirable perinatal outcomes and low BF initiation and duration for women with complex pregnancies such as DM, CHTN, preeclampsia and obesity [13,21,28,29,31]. As reported in the current manuscript, the number of NICU admissions due to hypoglycemia is lower than that reported in the past [21,32,33]. The treatment of hypoglycemia by early BF, FF or glucose gel administration in the Newborn Nursery may have prevented the need for intravenous glucose infusions given at the NICU [21,32,33]. Changes in our neonatal practices decreased the number of asymptomatic infants born to women with PGDM admitted to the NICU from the 2008–11 to the 2013–16 period, concurrently, EBF increased from 13 to 24% and ABF from 45 to 60%, respectively [33]. In spite of the progress made, the prevalence of late prematurity and the unavoidable mother-infant separation created by the NICU admission remained significant obstacles to BF [21,33].
Our data shows that socio-economic and racial discrepancies are associated with low rates of EBF and BF initiation in African Americans as compared to non-Hispanic Whites. In light of these findings, we agree that although BF rates in the U.S. have improved in the last decade, racial/ethnic disparities persist [40]. Additionally, we also acknowledge that maternal and child health is significantly influenced by a variety of factors including but not limited to race, ethnicity, education, insurance and multiple comorbidities, and that major efforts are still needed to improve BF and BF duration rates in the U.S [25-26, 40-41].
This investigation is limited by the lack of an infant feeding intention scale and follow-up information regarding infant feeding after discharge from the hospital. Also, the definition of BF initiation at discharge may be only applicable to women with complex pregnancies or whom early mother-infant contact may be delayed. The strength of this investigation rests on the size of the high risk obstetrical and neonatal population and the fact that the data were obtained directly from hospital records not via post-delivery maternal questionnaires.
Conclusion
In summary, we provided further evidence that intention to BF only is not an absolute predictor of EBF and of BF initiation for pregnancies complicated by severe obesity alone or superimposed on CHTN, preeclampsia and diabetes mellitus. Late prematurity, admission to NICU, neonatal hypoglycemia and racial and economic disparities remain obstacles to BF initiation. Although the rate of EBF and ABF reported here may seem disappointing, they still provide some optimism because multiparous women with prior BF experience are more likely to provide EBF or ABF in subsequent pregnancies. The fact that approximately twenty percent of primiparous women who intended to BF only failed to do so and FF their infants at hospital discharge represents a major challenge. Recognition that among women who intend to BF only, especially those in high-risk populations, a significant number fail to achieve their goal should prompt the implementation of strategies prior to discharge from the hospital to further successful BF initiation.
Supporting information
S1 DataRaw data.(XLSX)
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Creanga AA, Catalano PM, Bateman BT. Obesity in Pregnancy. N Engl J Med. 2022;387(3):248–59. doi: 10.1056/NEJ Mra 1801040 35857661 · doi ↗ · pubmed ↗
- 2ACOG Practice Bulletin #230. Obesity in pregnancy. Obstet Gynecol 2021;137: e 128–e 137.34011890 10.1097/AOG.0000000000004395 · doi ↗ · pubmed ↗
- 3Langley-Evans SC, Pearce J, Ellis S. Overweight, obesity and excessive weight gain in pregnancy as risk factors for adverse pregnancy outcomes: a narrative review. J Hum Nutr Diet. 2022;35(2):250–64. doi: 10.1111/jhn.12999 35239212 PMC 9311414 · doi ↗ · pubmed ↗
- 4Stuebe A. Associations between lactation, maternal carbohydrate metabolism, and cardiovascular health. Clin Obstet Gynecol. 2015;58(4):827–39. doi: 10.1097/GRF.0000000000000155 26457850 PMC 4968698 · doi ↗ · pubmed ↗
- 5Nguyen B, Jin K, Ding D. Breastfeeding and maternal cardiovascular risk factors and outcomes: a systematic review. P Lo S One. 2017;12(11):e 0187923. doi: 10.1371/journal.pone.0187923 29186142 PMC 5706676 · doi ↗ · pubmed ↗
- 6Fox R, Kitt J, Leeson P, Aye CYL, Lewandowski AJ. Preeclampsia: risk factors, diagnosis, management, and the cardiovascular impact on the offspring. J Clin Med. 2019;8(10):1625. doi: 10.3390/jcm 8101625 31590294 PMC 6832549 · doi ↗ · pubmed ↗
- 7Barrera CM, Beauregard JL, Nelson JM, Perrine CG. Association of maternity care practices and policies with in-hospital exclusive breastfeeding in the United States. Breastfeed Med. 2019;14(4):243–8. doi: 10.1089/bfm.2018.0196 30807205 PMC 6681453 · doi ↗ · pubmed ↗
- 8Meek JY, Noble L. Section on breastfeeding. policy statement: breastfeeding and the use of human milk. Pediatrics 2022;150:e 2022057988.35921640 10.1542/peds.2022-057988 · doi ↗ · pubmed ↗