Is timing as critical for repair of dextro-transposition of the great arteries with ventricular septal defect without outflow tract obstruction?
Muhammad Faateh, Spencer Hogue, Amir Mehdizadeh-Shrifi, Kevin Kulshrestha, Md Monir Hossain, David G. Lehenbauer, David L.S. Morales, Awais Ashfaq

TL;DR
This study examines the impact of timing on surgical outcomes for a specific heart defect in newborns, finding that earlier surgery may reduce complications and costs.
Contribution
The study identifies an optimal age cutoff for surgery and shows earlier intervention may improve secondary outcomes and reduce hospital costs.
Findings
Most surgeries occurred within the first week of life with similar in-hospital mortality across timing groups.
Surgery after 8 days was linked to a higher risk of a composite outcome and increased hospitalization costs.
Earlier surgery may offer advantages in secondary outcomes despite similar mortality rates.
Abstract
We sought to explore the role of timing on outcomes of the arterial switch operation + ventricular septal defect closure. Neonates undergoing the arterial switch operation + ventricular septal defect closure from the Pediatric Health Information System database (2004-2022) were identified. Patients with outflow tract obstruction were excluded. Baseline features and outcomes were compared by dividing the cohort by age at the arterial switch operation + ventricular septal defect closure: very early (0-7 days), early (8-14 days), late (15-21 days), and very late (>21 days). A cut-point analysis was performed to identify if an age-cutoff predicted the composite outcome (in-hospital mortality/nonhome discharge/postoperative extracorporeal membrane oxygenation/delayed sternum closure/reoperation due to bleeding). A total of 1005 patients were identified. The median age at repair was 6 days…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
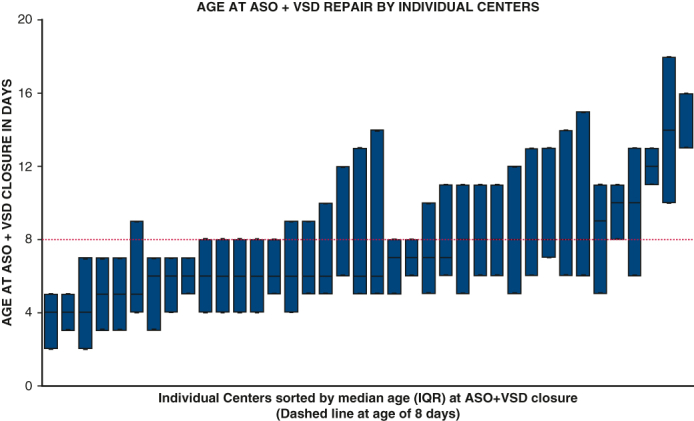 Figure 1
Figure 1 Figure 2
Figure 2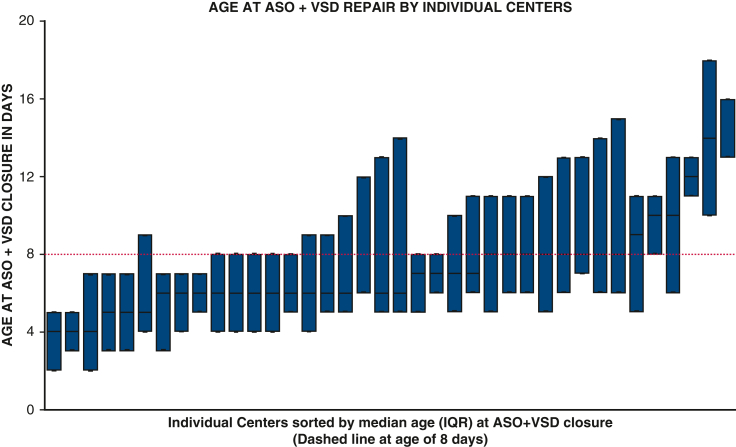 Figure 3
Figure 3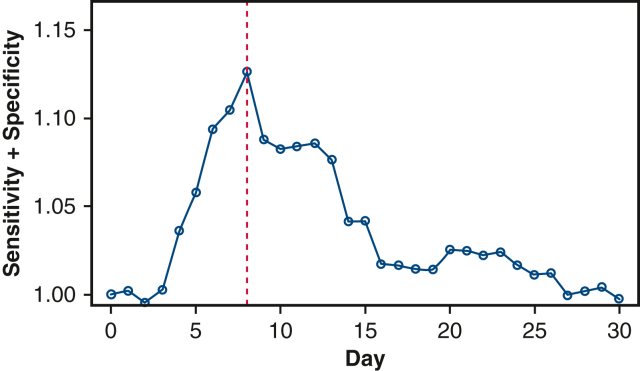 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCongenital Heart Disease Studies · Aortic Disease and Treatment Approaches · Cardiac Structural Anomalies and Repair
Variation in ASO + VSD timing in individual study centers. Central MessageMost patients undergo ASO + VSD closure within the first week of life. Early versus delayed repair within the first month does not affect mortality; however, repair at more than 1 week may result in worse secondary outcomes. PerspectiveThe impact of surgical timing of ASO + VSD closure in patients with d-TGA + VSD is not known well because prior reports examining the impact of ASO timing have often combined their outcomes with patients who have d-TGA + IVS. We aim to explore the characteristics, outcomes, and associated costs of early versus delayed ASO + VSD closure.
Dextro-transposition of the great arteries (d-TGA) is associated with ventricular septal defects (VSDs) in 20% to 40% of cases.1, 2, 3, 4 Relative to patients with d-TGA with an intact ventricular septum (IVS), the arterial switch operation (ASO) with VSD closure requires longer cardiopulmonary bypass and crossclamp times and is associated with longer postoperative hospital stays, a 2-fold increase in postoperative mortality, and impaired long-term neurological development.2, 3, 4, 5, 6 There is increasing consensus toward early ASO in patients born with d-TGA + IVS. However, d-TGA + VSD physiology can allow for additional volume loading of the left heart, which increases mixing at the atrial level. An unrestrictive VSD is protective against left ventricular deconditioning. Likely due to these reasons, historically there has been a lower perceived urgency with regard to surgical repair in these patients compared with d-TGA + IVS.3^,^7 Repair also may be delayed because of patient factors such as delayed presentation, prematurity, or low birth weight. A few prior reports emphasized improved patient outcomes and reduced hospitalization costs for earlier ASO, especially for patients with restrictive VSDs.8^,^9 However, others have described similar results for early versus delayed ASO + VSD repair.2^,^3^,^10 Most studies examining the impact of ASO + VSD closure timing remain limited to small, single-center patient populations or have not reported outcomes separately for ASO + VSD closure. Moreover, high-risk patients such as low-birthweight and premature patients often have been excluded in these comparisons. Therefore, the present study is a large, multicenter analysis of patient characteristics, institutional variation in timing of early versus delayed repair, and the clinical and financial implications of surgical timing on outcomes of ASO + VSD closure.
Material and Methods
Study Population and Data Source
A retrospective analysis of the Pediatric Health Information System (PHIS) database from January 1, 2004, to December 31, 2022, was performed. The PHIS is an administrative database composed of more than 40 major pediatric hospitals across the United States. Detailed information can be accessed at www.childrenshospitals.org. Patients born with a diagnosis of d-TGA + VSD undergoing ASO + VSD closure between the ages of 0 to 30 days were identified. Patients were excluded if they had a coexisting diagnosis of double-outlet right ventricle, outflow tract obstruction, or aortic arch repair. Diagnoses and procedures were identified by International Classification of Diseases 9th and 10th revision codes using the methodology described by Dhillon and colleagues.11 The Cincinnati Children's Hospital Institutional Review Board approved this study, and the need for individual patient consent was waived because this was a retrospective analysis of de-identified data (IRB #2018-6837; date of approval: October 29, 2018).
Covariates and Outcomes
Race and ethnicity were combined into a single categorical variable. Prematurity was defined as gestational age of less than 37 weeks and derived from PHIS-reported gestational age variable, and in case of missing information it was obtained by gestational age International Classification of Diseases codes. Birth weight was similarly derived. Household income is the median household income of a patient's zip code. This was adjusted for inflation (2022 USD) using urban consumer price index. Prostaglandin or inhaled nitric oxide variables indicate the use of these medications at any time preoperatively. The primary outcomes of interest were in-hospital mortality (death or discharge to hospice status) and postoperative extracorporeal membrane oxygenation (ECMO). Secondary outcomes included delayed sternum closure, reoperation for control of bleeding, and nonhome discharge. Nonhome discharge includes discharge to a rehabilitation/short- or long-term acute care or nursing facility, as well as transfers to other hospitals. A binary composite outcome was created that denotes occurrence of any components of the primary or secondary outcomes. A variable containing primary outcomes indicating in-hospital death or postoperative ECMO was also created. Additional outcomes included length of stay, postoperative dialysis use, permanent pacemaker implantation, and adjusted estimated hospitalization costs. Hospitalization costs were derived from charge-to-cost ratios reported by each hospital and adjusted for inflation (2022 USD) using medical consumer price index. The prevalence of concomitant morbidities/diagnoses, including stroke, heart failure, pulmonary hypertension, acute respiratory distress syndrome, necrotizing enterocolitis, hepatic failure, renal failure, and sepsis, was identified. The timing (preoperative vs postoperative) of these variables could not be distinguished because the database only indicates if they were present at the time of admission to hospital or occurred at any point during the hospitalization.
Statistical Analysis
The entire cohort was divided into 4 subgroups based on age at ASO + VSD closure. The groups were very early (0-7 days), early (8-14 days), late (15-21 days), and very late (>21 days). Baseline characteristics, outcomes, and hospitalization costs were compared by these groups. A cut-point analysis was performed by using a predictive ability metric, plotting the sum of sensitivity and specificity against age (in days) by serially dichotomizing the data by age at surgery (ie, age 0 day vs > 0, age 0-1 day vs > 1, age 0-29 vs 30 days) to identify if a clear cutoff day/range for ASO + VSD closure was a predictor of developing the composite outcome. The cut-point with the highest sum of sensitivity + sensitivity was chosen for the final comparisons.
In addition, subanalyses of outcomes by age at ASO + VSD closure were performed stratified by prematurity (<37 weeks), low birth weight (<2.5 kg), and delayed presentation (admission age >3 days). The median age and interquartile range (IQR) of ASO + VSD closure for individual hospitals were computed to assess variation in timing of ASO by center. Chi-square, t test, rank sum, Kruskal–Wallis with pairwise comparisons, and analysis of variance were used to compare baseline characteristics and outcomes as appropriate. Multivariable logistic regression analysis was performed by adjusting for clinically significant predictors of the composite outcome. All analyses were performed using Stata 18.0 (Stata Corp).
Results
A total of 1005 patients undergoing ASO + VSD were identified. The median age at ASO + VSD closure for the entire cohort was 6 days (IQR, 4-9). Overall, 31 patients (3.1%) experienced in-hospital death. The distribution of patients by age at ASO + VSD closure groups was as follows: very early 652 (64.9%), early 247 (24.6%), late 72 (7.2%), and very late 34 (3.4%). Patients in the late and very late groups were more likely to be preterm (39 [6.3%] vs 33 [13.8%] vs 16 [23.2%] vs 9 [26.5%], respectively, P < .001, very early vs all other groups pairwise <.05) and to have low birth weight (35 [5.8%] vs 21 [9%] vs 14 [21.9%] vs 6 [20%], respectively, P < .001, all pairwise <.05). The latter groups had a higher proportion of patients with delayed presentation (admission age >3 days) (26 [3.9%] vs 31 [12.6%] vs 24 [33.3%] vs 16 [47.1%], respectively, P < .001). Patients across groups were similar in terms of race/ethnicity, gender, insurance, preoperative stroke (on admission), presence of atrial septal defect (ASD), coronary anomalies, or balloon atrial septostomy (all P > .05). Detailed baseline comparisons are shown in Table 1.Table 1. Baseline characteristics of patients with dextro-transposition of the great arteries + ventricular septal defect by age at arterial switch operation + ventricular septal defect closureVariablesVery early(0-7 d)n (%) = 652 (64.9)Early(8-14 d)n (%) = 247 (24.6)Late(15-21 d)n (%) = 72 (7.2)Very late(>21 d)n (%) = 34 (3.4)P valueMedian (IQR) age at ASO + VSD closure5, 3-6 d10, 8-12 d18, 16-20 d25, 23-28 d-Mean, SD4.6, 1.8 d10.3, 1.9 d17.7, 2.1 d25.3, 2.7 d-Female gender197 (30.2)77 (31.2)21 (29.2)17 (50.0).11Race/ethnicity.57 White344 (52.8)127 (51.4)43 (59.7)22 (64.7) Black51 (7.8)24 (9.7)5 (6.9)1 (2.9) Other94 (14.4)43 (17.4)10 (13.9)2 (5.9) Hispanic116 (17.8)43 (17.4)11 (15.3)7 (20.6) Unknown47 (7.2)10 (4.1)3 (4.2)2 (5.9)Gestational age, wk<.001 ≥37585 (89.7)206 (83.4)53 (73.6)25 (73.5)A vs B <.001 33-3638 (5.8)29 (11.7)13 (18.1)8 (23.5)A vs C <.001 29-321 (0.2)3 (1.2)2 (2.8)1 (2.9)A vs D <.001 ≤280 (0)1 (0.4)1 (1.4)0 (0.0) Unknown28 (4.3)8 (3.2)3 (4.2)0 (0.0)Birth weight, g<.001 ≥2500570 (87.4)212 (85.8)50 (69.4)24 (70.6)A vs B <.001 2000-249930 (4.6)18 (7.3)11 (15.3)4 (11.8)A vs C <.001 <20005 (0.8)3 (1.2)3 (4.2)2 (5.9)A vs D = .003 Unknown47 (7.2)14 (5.7)8 (11.1)4 (11.8)Median age at admission0, 0-1 d0, 0-2 d1, 0-12 d3, 0-20 d<.001Admission age >3 d26 (3.9)31 (12.6)24 (33.3)16 (47.1)<.001Origin of admission<.001 Birth171 (26.2)43 (17.4)6 (8.3)3 (8.8) Transfer46 (7.1)19 (7.7)14 (19.4)10 (29.4) Outpatient381 (58.4)162 (65.6)40 (55.6)17 (50.0) Unknown54 (8.3)23 (9.3)12 (16.7)4 (11.8)Government/state insurance273 (43.3)122 (50.0)35 (49.3)15 (44.1).31Median household income (IQR)52,875, 41,969- 66,53449,753, 40,086-71,972.04Era.56 2004-2010300 (46.0)101 (40.9)37 (51.4)12 (35.3) 2011-2016206 (31.6)87 (35.2)22 (30.6)12 (35.3) 2017-2022146 (22.4)59 (23.9)13 (18.1)10 (29.4)PDA503 (77.2)210 (85.0)59 (81.9)22 (64.7).01ASD594 (91.1)222 (89.9)65 (90.3)29 (85.3).69Coronary anomalies70 (10.7)34 (13.8)14 (19.4)3 (8.8).13Preoperative stroke (on admit)15 (2.3)12 (4.9)0 (0)2 (5.9).04BAS251 (38.5)104 (42.1)30 (41.7)15 (44.1).71Age at BAS, median, IQR1, 0-1 d1, 1-2 d1, 1-14 d2, 1-14 d<.001ASD repair551 (84.5)208 (84.2)64 (88.9)30 (88.2).78Preoperative ECMO2 (0.3)3 (1.2)1 (1.4)0 (0).22Preoperative PGE-1 infusion525 (85.2)182 (79.8)44 (65.7)19 (57.6)<.001Preoperative iNO43 (7.0)19 (8.3)4 (5.9)3 (9.1).82IQR, Interquartile range; ASO, arterial switch operation; VSD, ventricular septal defect; PDA, patent ductus arteriosus; ASD, atrial septal defect; BAS, balloon atrial septostomy; ECMO, extracorporeal membrane oxygenation; PGE-1, prostaglandin E-1; iNO, inhaled nitric oxide.
Outcomes Stratified by Repair Age
Patients in all 4 age groups (very early vs early vs late vs very late) had similar in-hospital mortality (17 [2.6%] vs 11 [4.5%] vs 2 [2.8%] vs 1 [2.9%], respectively, P = .47) and postoperative ECMO requirement (21 [3.2%] vs 11 [4.5%] vs 4 [5.6%] vs 2 [5.9%], respectively, P = .40). Patients in the very late group had the highest proportion of delayed sternum closure (47 [7.2%] vs 23 [9.3%] vs 8 [11.1%] vs 8 [23.5%], respectively, P = .007). The composite outcome was lowest in the very early age group (106 [16.3%] vs 61 [24.7%] vs 17 [23.6%] vs 10 [29.4%], respectively, P < .001, very early vs early P = .004, very early vs late P = .115, very early vs very late, respectively, P = .046). The postoperative length of stay was similar across groups (P = .66). Median hospitalization costs were lowest in the very early group (177,376 vs 202,268, respectively, P < .001).
Concomitant diagnoses/outcomes (occurring preoperatively or postoperatively) were as follows: heart failure (108 [16.6%] vs 52 [21.1%] vs 17 [23.6%] vs 12 [35.3%], P = .018), stroke (37 [5.7%] vs 26 [10.5%] vs 6 [8.3%] vs 4 [11.8%], P = .04), necrotizing enterocolitis (8 [1.2%] vs 3 [1.2%] vs 3 [4.2%] vs 5 [14.7%], P < .001), and renal failure (75 [11.5%] vs 37 [14.9%] vs 8 [11.1%] vs 10 [29.4%], respectively, P = .015) (Table 2).Table 2. Outcomes by age at arterial switch operation + ventricular septal defect closureVery early(0-7 d)n (%) = 652 (64.9)Early(8-14 d)n (%) = 247 (24.6)Late(15-21 d)n (%) = 72 (7.2)Very late(>21 d)n (%) = 34 (3.4)P valueDeath17 (2.6)11 (4.5)2 (2.8)1 (2.9).47Postoperative ECMO21 (3.2)11 (4.5)4 (5.6)2 (5.9).40Death or ECMO28 (4.3)16 (6.5)5 (6.9)2 (5.9).38Delayed sternum closure47 (7.2)23 (9.3)8 (11.1)8 (23.5).007Reoperation for bleeding28 (4.3)23 (9.3)3 (4.2)2 (5.9).03Composite of the above outcomes106 (16.3)61 (24.7)17 (23.6)10 (29.4)<.001A vs B = .004A vs C = .115A vs D = .046Permanent pacemaker23 (3.5)6 (2.4)2 (2.8)0 (0).77Postoperative dialysis11 (1.8)7 (3.1)4 (5.9)0 (0).12Nonhome discharge (survivors)17 (2.7)9 (3.8)3 (4.3)0 (0).59Total LOS, median, IQR17, 13-23 d22, 18-29 d28, 20-39 d34, 21-48 d<.001Postoperative LOS, median, IQR13, 9-18 d12, 9-19 d15, 9-25 d12, 9-25 d.66Total ICU LOS, median, IQR13, 10-19 d18, 15-24 d25, 12-35 d21, 10-45 d<.001Postoperative ICU LOS, median, IQR8, 5-14 d8, 5-13 d11, 6-19 d9, 6-21 d.22Hospitalization costs, median, IQR177,376, 137,929-247,703202,268, 136,146-367,160<.001A vs B <.001A vs C <.001A vs D = .001Concomitant outcomes/diagnoses for the entire admission (occurring preoperatively or postoperatively) Stroke37 (5.7)26 (10.5)6 (8.3)4 (11.8).04 Heart failure108 (16.6)52 (21.1)17 (23.6)12 (35.3).018 Pulmonary hypertension9 (1.4)3 (1.2)3 (4.2)0 (0).31 ARDS93 (14.3)39 (15.8)13 (18.1)4 (11.8).75 Necrotizing enterocolitis8 (1.2)3 (1.2)3 (4.2)5 (14.7)<.001 Hepatic failure0 (0)1 (0.4)0 (0.0)1 (2.9).028 Renal failure75 (11.5)37 (14.9)8 (11.1)10 (29.4).015 Sepsis14 (2.2)5 (2.0)3 (4.2)0 (0).62ECMO, Extracorporeal membrane oxygenation; LOS, length of stay; IQR, interquartile range; ICU, intensive care unit; ARDS, acute respiratory distress syndrome.
Outcomes in Preterm (<37 Weeks), Low-Birthweight (<2.5 kg), and Delayed Presentation (Admission Age >3 Days) Groups
The overall mortality in preterm neonates was 10 of 97 (10.3%) and similar by age at surgery (P = .23). The composite outcome in preterm patients was also similar across groups (14 [35.9%] vs 12 [36.4%] vs 5 [31.3%] vs 5 [55.6%], respectively, P = .67). Likewise, the mortality and composite outcomes were similar in low-birthweight patients and patients with delayed presentation (all P > .05). Patients who were born at term, had normal birth weight, and were admitted within 3 days of birth had similar mortality by age at surgery (P = .67); however, there was a lower proportion of patients who had delayed sternum closure or composite outcome in the very early group (both P < .05) (Table 3).Table 3. Logistic regression comparing arterial switch operation + ventricular septal defect closure outcomes by age cutoff (0-8 vs >8 days)Univariable OR (95% CI)P valueAdjusted OR∗ (95% CI)P valueIn-hospital mortality1.40 (0.66-2.96).38--Postoperative ECMO1.67 (0.86-3.26).13--Death or ECMO1.53 (0.85-2.74).16--Delayed sternum closure1.39 (0.87-2.21).17--Reoperation for bleeding1.55 (0.89-2.71).13--Nonhome discharge1.14 (0.52-2.53).75--Composite outcome1.51 (1.08-2.11).0151.47 (1.02-2.15).041OR, Odds ratio; ECMO, extracorporeal membrane oxygenation.∗Adjusted for age at admission, gestational age, coronary anomaly, patent ductus arteriosus, insurance, and household income.
Variation in Age at Arterial Switch Operation + Ventricular Septal Defect Closure by Center
ASO + VSD closure was performed in a majority (24/38) of centers in patients with a median age of 7 days or younger. Patients in 8 centers had a median age at surgery of 8 days, and patients in 6 centers had a median age of more than 8 days. Because 6 centers reported less than 5 total cases throughout the study period, they were excluded for this evaluation (Figure 1).Figure 1. Box-plot showing in median age and IQR of ASO + VSD closure for individual study centers. IQR, Interquartile range; ASO, arterial switch operation; VSD, ventricular septal defect.
Comparisons of Outcomes by Age Cutoff Identified by Cut-point Analysis
The identified cutoff for age at ASO + VSD closure with the maximum sum of sensitivity + specificity was 8 days (Figure 2). Individually, the odds of in-hospital mortality, postoperative ECMO, in-hospital mortality or postoperative ECMO, delayed sternum closure, reoperation for control of bleeding, or nonhome discharge were not statistically significant when ASO + VSD closure was performed after more than 8 days (all P > .05). However, the odds of composite outcome comparing ASO + VSD closure age more than 8 days versus 0-8 days was 1.51 (95% CI, 1.08-2.11, P = .015). This remained significant in the multivariable regression analysis after adjusting for age at admission, gestational age, coronary anomaly, patent ductus arteriosus, insurance, and household income (OR, 1.47, 95% CI, 1.02-2.15, P = .041) (Table 4).Figure 2. Cut-point analysis revealing 8 days as the cutoff for predicting ASO + VSD outcome (red line at 8 days). ASO, Arterial switch operation; VSD, ventricular septal defect.Table 4. Subanalysis of arterial switch operation + ventricular septal defect closure outcomes by age in premature, low-birthweight, and delayed presentation patientsVery early(0-7 d)Early(8-14 d)Late(15-21 d)Very late(>21 d)P valuePremature birth (<37 wk) n (%)39 (40.2)33 (34.0)16 (16.5)9 (9.3)- Gestational age, wk- 33-3638 (97.4)29 (87.9)13 (81.3)8 (88.9) 29-321 (2.6)3 (9.1)2 (12.5)1 (11.1) ≤280 (0)1 (3.0)1 (6.3)0 (0.0) Mortality4 (10.3)6 (18.2)0 (0)0 (0).23 Postoperative ECMO2 (5.1)2 (6.1)0 (0)0 (0)1.0 Death or ECMO5 (12.8)6 (18.2)0 (0)0 (0).24 Delayed sternum closure5 (12.8)4 (12.1)2 (12.5)4 (44.4).09 Reoperation for bleeding3 (7.7)3 (9.1)1 (6.3)1 (11.1)1.0 Composite outcome14 (35.9)12 (36.4)5 (31.3)5 (55.6).67 Postoperative LOS, median, IQR17, 13-35 d19, 12-37 d18, 9-31 d22, 15-43 d.80Low birth weight (<2.5 kg) n (%)35 (46.1)21 (27.6)14 (18.4)6 (7.9)- Birth weight, g- 2000-249930 (85.7)18 (85.7)11 (78.6)4 (66.7) <20005 (14.3)3 (14.3)3 (21.4)2 (33.3) Mortality4 (11.4)5 (23.8)0 (0)0 (0).19 Postoperative ECMO4 (11.4)1 (4.8)0 (0)0 (0).67 Death or ECMO6 (17.1)5 (23.8)0 (0)0 (0).19 Delayed sternum closure3 (8.6)4 (19.1)2 (14.3)2 (33.3).38 Reoperation for bleeding3 (8.6)2 (9.5)0 (0)0 (0).80 Composite outcome12 (34.3)11 (52.4)3 (21.4)2 (33.3).32 Postoperative LOS, median, IQR17, 12-37 d16, 11-35 d16, 12-18 d34, 22-86 d.15Delayed presentation (age at admission >3 d) n (%)26 (26.8)31 (31.9)24 (24.7)16 (16.5)- Admission age in d4, 4-5 d7, 5-8 d14, 12-17 d20, 14-23 d- Mortality1 (3.9)0 (0)1 (4.2)1 (6.3).48 Postoperative ECMO2 (7.7)0 (0.0)2 (8.3)1 (6.3).36 Death or ECMO2 (7.7)0 (0)3 (12.5)1 (6.3).19 Delayed sternum closure2 (7.7)1 (3.3)0 (0)1 (6.3).55 Reoperation for bleeding1 (3.9)2 (6.5)2 (8.3)1 (6.3).94 Composite outcome5 (19.2)6 (19.4)7 (29.2)3 (18.8).83 Postoperative LOS, median, IQR10, 9-15 d9, 7-12 d12, 7-18 d11, 8, 14 d.39Term (≥37 wk), normal birth weight (≥2.5 kg) with admission age ≤3 d n (%)509 (71.6)165 (23.2)26 (3.7)11 (1.6)- Mortality9 (1.8)3 (1.8)1 (3.9)0 (0).67 Postoperative ECMO14 (2.8)7 (4.2)2 (7.7)1 (9.1).14 Death or ECMO17 (3.3)7 (4.2)2 (7.7)1 (9.1).25 Delayed sternum closure34 (6.7)16 (9.7)4 (15.4)3 (27.3).025 Reoperation for bleeding21 (4.1)16 (9.7)1 (3.9)1 (9.1).041 Composite outcome74 (14.5)36 (21.8)6 (23.1)3 (27.3).07 Postoperative LOS, median, IQR13, 9-18 d12, 9-18 d19, 9-25 d13, 9-38 d.17ECMO, Extracorporeal membrane oxygenation; LOS, length of stay; IQR, interquartile range.
Discussion
To our knowledge, the present multi-institutional study is the largest report of d-TGA + VSD as an isolated cohort, including more than 1000 ASO + VSD closures. Most patients underwent ASO + VSD closure early within the first week of life. Patients who underwent delayed repair were more likely to be premature, to have low birth weight, or to have delayed presentation. Overall, in-hospital mortality and primary outcomes were similar in all 4 groups. However, earlier repair may have advantages with regard to secondary outcomes and healthcare use burden.
Most centers in the present study performed ASO + VSD closure within the first week. This represents a departure from the traditional approach of delayed repair for d-TGA + VSD and may be a result of contemporary literature that has generally encouraged performance of ASO as early as possible. Anderson and colleagues4 reported a 40% increase in risk each day ASO is delayed (>3 days) from a cohort of 140 ASOs, of which 35 (25%) had VSD closure.4 Pletzer and colleagues8 reported adverse outcomes with increasing surgical age of ASO + VSD closure in infants. Ahlström and colleagues9 did not find significant differences in outcomes of delayed ASO (>7 days) from a cohort of 241 ASOs, of which 83 had d-TGA + VSD. It is important to consider that most of these aforementioned studies included d-TGA + IVS, which is more sensitive to timing. Our results suggest that surgical timing (within the first month) does not play a major role in mortality in patients with d-TGA + VSD; however, earlier repair could be beneficial for improving secondary outcomes, such as the need for delayed sternal closure and hospitalization costs.
In patients undergoing ASO, the requirement of postoperative ECMO, delayed sternal closure, and reoperation for bleeding is likely multifactorial.12^,^13 In the present study, however, mortality and ECMO were similar by surgical timing, despite a greater proportion of preterm and low-birthweight patients in the late groups. The major drivers of delayed repair were patient factors such as prematurity, low birth weight, and delayed presentation. In addition, transfer from an outside hospital and lower household income are likely surrogates for lack of prenatal diagnosis. Prior studies reporting outcomes by the timing of ASO + VSD closure have often excluded patients born prematurely or with low birth weight.1^,^4 One report suggested that delays in ASO in low-birthweight patients may be unnecessary.14 In the present study, the mortality, length of stay, and total hospitalization costs were similar by surgical timing in preterm and low-birthweight patients.
Complications, including stroke, heart failure, necrotizing enterocolitis, and renal failure, were all significantly higher in the late ASO + VSD closure group. Lim and colleagues2 highlighted a significant association between the presence of d-TGA + VSD and older age at surgical repair with postoperative neurodevelopmental dysfunction from a cohort of 45 patients with d-TGA, of whom 11 underwent ASO + VSD closure. Moreover, the general presentation of a hemodynamically significant VSD with d-TGA has demonstrated elevated risks for congestive heart failure compounded by increased durations between birth and ASO.7^,^15 However, we were unable to discern from this study when these were diagnosed during their admission because of limitations of the database.
Limitations
This study has some limitations. These are related to its retrospective nature and analysis of administrative database. Operative variables such as bypass or crossclamp times, VSD size, or location were not available. We were unable to distinguish or adjust for the timing of certain key factors such as failure of organ systems. Although we used a regression model and performed a stratified analysis, the exact factors and decision-making that may have led to delay were unavailable to be determined from this database. It is challenging to completely uncouple surgical timing from individual patient characteristics that may have led to delays. We were unable to assess the role of surgical timing by corrected gestational age. We do not report outcomes beyond the in-hospital period and may have missed a few early deaths within the perioperative period. The strengths of this study are its large sample size drawn from multiple centers across the United States, availability of financial data that offer a broad picture of contemporary ASO + VSD outcomes, and insight into potential etiologies of early versus late surgical timing of repair.
Conclusions
This analysis of more than 1000 neonates born with d-TGA with a VSD without outflow tract obstruction revealed similar post–ASO + VSD closure in-hospital mortality within the first 30 days of life. In the contemporary era, surgery was performed at most study centers within the first week of the patient's life. Reasons for delay beyond this period included prematurity, low birth weight (<2.5 kg), and delayed presentation (>3 days of birth). Earlier repair may be advantageous with respect to secondary outcomes and healthcare use burden.
Webcast
You can watch a Webcast of this AATS meeting presentation by going to: https://www.aats.org/resources/early-versus-late-arterial-swi-7314.
Conflict of Interest Statement
A.A.: Principal Investigator for Pyrames. D.L.S.M.: Abbott Vascular, Aziyo, Xeltis BV, Berlin Heart, SynCardia Systems (consulting/advisory). All other authors reported no conflicts of interest.
The Journal policy requires editors and reviewers to disclose conflicts of interest and to decline handling or reviewing manuscripts for which they may have a conflict of interest. The editors and reviewers of this article have no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Smith A.H.Shin A.Y.Tabbutt S.Age at surgery and outcomes following neonatal cardiac surgery: an analysis from the Pediatric Cardiac Critical Care Consortium J Thorac Cardiovasc Surg 1654202315281538.e 710.1016/j.jtcvs.2022.05.02935760618 · doi ↗ · pubmed ↗
- 2Lim J.M.Porayette P.Marini D.Associations between age at arterial switch operation, brain growth, and development in infants with transposition of the great arteries Circulation 1392420192728273810.1161/circulationaha.118.03749531132861 · doi ↗ · pubmed ↗
- 3Duncan B.W.Poirier N.C.Mee R.B.Selective timing for the arterial switch operation Ann Thorac Surg 77520041691169610.1016/j.athoracsur.2003.10.04215111168 · doi ↗ · pubmed ↗
- 4Anderson B.R.Ciarleglio A.J.Hayes D.A.Quaegebeur J.M.Vincent J.A.Bacha E.A.Earlier arterial switch operation improves outcomes and reduces costs for neonates with transposition of the great arteries J Am Coll Cardiol 635201448148710.1016/j.jacc.2013.08.164524184243 · doi ↗ · pubmed ↗
- 5Cain M.T.Cao Y.Ghanayem N.S.Transposition of the great arteries--outcomes and time interval of early neonatal repair World J Pediatr Congenit Heart Surg 52201424124710.1177/215013511352055924668972 · doi ↗ · pubmed ↗
- 6Fraser C.D.Jr.Chacon-Portillo M.A.Well A.Twenty-three-year experience with the arterial switch operation: expectations and long-term outcomes Semin Thorac Cardiovasc Surg 322202029229910.1053/j.semtcvs.2020.01.00431958553 · doi ↗ · pubmed ↗
- 7Daoud Z.Nuri H.A.Miette A.PomèG.Transposition of the great vessels and intact ventricular septum: is there an age limit for the arterial switch? Personal experience and review of the literature Cardiol Young 30720201012101710.1017/s 104795112000145632594960 · doi ↗ · pubmed ↗
- 8Pletzer S.A.Atz A.M.Chowdhury S.M.The relationship between pre-operative left ventricular longitudinal strain and post-operative length of stay in patients undergoing arterial switch operation is age dependent Pediatr Cardiol 402201936637310.1007/s 00246-018-2018-130413855 PMC 6415533 · doi ↗ · pubmed ↗