Seroprevalence of Toxoplasmosis in Sheep and Its Zoonotic Importance in Hargeisa, Somaliland
Abdiqani Mohamed Jama, Taddesse Yayeh Yihun

TL;DR
This study found that toxoplasmosis is common in sheep and pregnant women in Hargeisa, Somaliland, and highlights the need for better hygiene and food safety to prevent infections.
Contribution
The study provides new insights into the seroprevalence and risk factors of toxoplasmosis in a specific region of Somaliland.
Findings
Toxoplasmosis prevalence was 25.5% in sheep and 28% in pregnant women in Hargeisa.
Risk factors for pregnant women include having cats, poor hygiene, and drinking tap water.
Young female sheep were more likely to be seropositive for Toxoplasma gondii.
Abstract
Toxoplasmosis has public health importance, particularly in immunocompromised individuals such as pregnant women leading to congenital abnormalities and fetal losses. In this study, we aimed to determine the seroprevalence of toxoplasmosis in sheep at Mandeeq Slaughter House in Hargeisa and pregnant women attending antenatal care at Hargeisa Group Hospital. Cross‐sectional study design with systematic random sampling method and Questionnaire surveys were used for the collection of data from sheep and pregnant women. Sera were collected and examined for anti‐Toxoplasma gondii antibodies using latex agglutination test. The overall prevalences of toxoplasmosis were 25.5% and 28% in sheep and human, respectively. Multivariable logistic regression analysis indicated that female (AOR = 2.18; 95% CI: 1.38–3.47; p = 0.001) and young age groups of sheep (AOR = 3.04; 95% CI: 1.04–8.86; p =…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
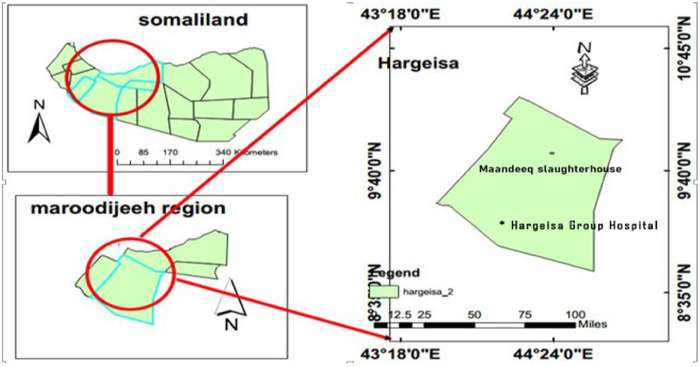 FIGURE 1
FIGURE 1| Variables | Number of examined ( | Number of positive % ( | COR 95% (CI) |
| AOR 95% (CI) |
|
|---|---|---|---|---|---|---|
|
| ||||||
|
Local Non local |
392 8 |
100 (25.5%) 2 (25%) |
0.97 (0.19–4.90) Ref 1.00 | 0.974 |
0.92 (0.17–4.85) Ref 1.00 | 0.927 |
|
| ||||||
|
Female Male |
225 175 |
42 (18.7%) 60 (34.2%) |
2.27 (1.43–3.59) Ref 1.00 | 0.001 |
2.18 (1.38–3.47) Ref 1.00 | 0.001 |
|
| ||||||
|
Young Adult |
41 359 |
4 (9.8%) 98 (27.3%) |
3.36 (1.16–9.70) Ref 1.00 | 0.041 |
3.04 (1.04–8.86) Ref (1.00) | 0.041 |
| Variables | Number of examined ( | Number of positive % ( | COR 95% (CI) |
| AOR 95% (CI) |
|
|---|---|---|---|---|---|---|
|
| ||||||
| 15–24 | 26 | 6 (23%) | 2.41 (0.82–7.04) | 0.107 | 1.35 (0.34–5.32) | 0.534 |
| 25–34 | 124 | 29 (23.3%) | 2.37 (1.17–4.77) | 0.015 | 2.76 (1.07–7.14) | 0.037 |
| 35–44 | 50 | 21 (42%) | Ref 1.00 | |||
|
| ||||||
| First | 36 | 7 (19.4%) | 4.14 (1.41–12.17) | 0.010 | 2.73 (0.67–4.05) | 0.158 |
| Second | 132 | 33 (25%) | 3.03 (1.35–6.65) | 0.007 | 2.87 (0.96–9.11) | 0.074 |
| Third | 32 | 16 (50%) | Ref 1.00 | |||
|
| ||||||
| Yes | 50 | 21 (42%) | 2.37 (1.20–4.69) | 0.012 | 0.67 (0.28–1.73) | 0.415 |
| No | 150 | 35 (23.3%) | Ref 1.00 | |||
|
| ||||||
| Yes | 30 | 18 (60.1%) | 5.21 (2.30–11.70) | 0.000 | 6.45 (2.37–17.52) | 0.000 |
| No | 170 | 38 (22.3%) | Ref 1.00 | |||
|
| ||||||
| Yes | 33 | 25 (75.5%) | 0.15 (0.06–0.33) | 0.000 | 0.12 (0.04–0.35) | 0.000 |
| No | 167 | 31 (18.4%) | Ref 1.00 | |||
|
| ||||||
| Yes | 89 | 25 (28%) | 0.99 (0.53–1.84) | 0.992 | 1.09 (0.45–2.62) | 0.838 |
| No | 111 | 31 (27.9%) | ||||
|
| ||||||
| Yes | 32 | 19 (59.3%) | 5.17 (2.33–11.45) | 0.000 | 6.74 (2.55–17.81) | 0.000 |
| No | 168 | 37 (22%) | Ref 1.00 | |||
|
| ||||||
| Yes | 185 | 44 (23.7%) | 12.81 (3.4–47.48) | 0.000 | 29.5 (5.4–161.11) | 0.000 |
| No | 15 | 12 (80%) | Ref 1.00 | |||
|
| ||||||
| Tap water | 136 | 48 (35.3%) | 3.81 (1.68–8.67) | 0.001 | 8.4 (2.54–28.08) | 0.000 |
| Well | 64 | 8 (12.5%) | Ref 1.00 | |||
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsToxoplasma gondii Research Studies · Parasitic Infections and Diagnostics · Animal Disease Management and Epidemiology
Introduction
1
Toxoplasmosis, caused by Toxoplasma gondii, is a zoonotic disease that commonly infects sheep [1] and the public with economic impacts everywhere [2]. It is an emerging foodborne parasitic disease affecting one‐third of the human population [3]. Toxoplasmosis is transmitted by ingestion of food, water, vegetables, and fruits contaminated with sporulated oocysts sheded from cats or ingesting tissue cysts from raw or undercooked meat; or transplacental transmission of tachyzoites [4]. In the case of immunocompromised pregnant women, toxoplasmosis is associated with severe neurological or ocular diseases such as chorioretinitis, blindness, myocarditis associated with various complications, cerebral anomalies, hydrocephalus, intracranial calcifications, microcephaly, convulsions, schizophrenia, and epilepsy [5, 6, 7, 8, 9].
East Africa is spotted as a high‐risk area for toxoplasmosis due to close linkage between human and livestock, sociocultural practices, poor environmental hygiene, and poverty [10]. In this region, more than one‐half of pregnant women were infected [11]. Despite the few studies on the high prevalence of human toxoplasmosis in Somalia [12], the status of toxoplasmosis both in animals and humans in Somaliland, the secessionist northwestern slice of Somalia that declared independence in 1991 [13], remained unknown. Therefore, this study aimed to estimate the seroprevalence of toxoplasmosis in sheep and pregnant women in Hargeisa, Somaliland.
Materials and Methods
2
Study Area
2.1
Hargeisa is the capital city of Somaliland. It is situated in the western part of Somaliland about 160 km Northeast of Jigjiga. It is considered to be the most populous city in Somaliland. The altitude of this city is around 1334 m above sea level, and it is located between 9.5624° N latitude and 44.0770° E longitude. Hargeisa, semi‐arid type of climate, receives the bulk of its precipitation between the months of April and September with an annual rainfall of 400 mm. The average monthly temperature of Hargeisa ranges from 18°C in December and January to 24°C in June. Data were collected from two locations of Hargeisa: Mandeeq abattoir and Hargeisa Group Hospital (HGH) (Figure 1).
Map of Somaliland showing the location of study sites.
Study Design
2.2
A cross‐sectional study was conducted to estimate the prevalence of toxoplasmosis and identify potential risk factors associated with seropositive pregnant women attending antenatal care (ANC) in HGH (referral public hospital) from June 2021 to December 2021.
Study Population, Inclusion, and Exclusion Criteria
2.3
The source population were sheep slaughtered at Mandeeq slaughter house for human consumption, and all pregnant women visiting HGH for ANC. Pregnant women 18 years old and above were considered during the study period. This study excluded those pregnant women refusing for participation and those who are sick at the time of attending ANC.
Sample Size and Sampling Method
2.4
An estimated number of 400 sheep were sampled. Blood collection was arranged to complete within 2 weeks. Thus, each day for a period of 2 weeks, 28 sheep were selected by systematic random sampling method. We also estimated to sample 200 pregnant women from HGH within a week. Each day, around 50 pregnant women had a visit to the Hospital, of which 28 of them were sampled daily.
Blood Sample Collection and Serum Preparation
2.5
Aseptically, around 5 mL of blood was drawn from the jugular vein of sheep and allowed to clot for serum separation. After consenting pregnant women, 5 mL of venous blood was collected by laboratory nurses into a plain vacutainer tube by using sterile disposable syringe. The tubes were appropriately labeled with the identity number of participants and the blood was allowed to coagulate at room temperature. All samples were sent to Somaliland National Veterinary Laboratory (SNVL), and serums were separated from the whole blood by centrifugation at 2800 × g for 5 min. Serum samples were aliquoted into two portions by using a sterile Pasteur pipette and stored at −20°C before performing serological tests for T. gondii.
Questionnaire Survey
2.6
Questionnaire survey was conducted to identify potential risk factors associated with the existence of toxoplasmosis in pregnant women. Factors such as location, age, pregnancy status, stage of pregnancy, presence of cats at home, physical contact with cats, and consumption of raw/undercooked meat, consumption of raw vegetables and fruits, and source of drinking water were considered.
Principle and Performance of the Test
2.7
Toxo‐latex test is a rapid slide agglutination procedure, developed to detect more than 10 IU/mL anti‐toxoplasma antibodies. The assay was performed by testing a suspension of latex particles coated with antigenic extract of T. gondii against unknown samples. As described by manufacturer, 50 µL sera samples and 25 µL of Toxo‐latex reagent were placed on the Toxo‐latex agglutination slide and one drop of each positive and negative control separate circles on the slide text and mixed thoroughly. The presence or absence of a visible agglutination indicates the presence or absence of anti‐toxoplasma antibodies in the sample.
Quality Control
2.8
Every day, the collected data were reviewed and checked for completeness. For laboratory investigations, standardized operating procedures and manufacturer's instructions were strictly followed. The quality of latex agglutination kits for anti‐T. gondii was checked by both positive and negative controls.
Data Management and Analysis
2.9
Data from questionnaire and laboratory findings were coded and entered into SPSS version 26.0 for descriptive statistics and multiple logistic regression analysis. A p value less than 0.05 were considered to be statistically significant.
Result
3
Prevalence of Toxoplasmosis and Its Associated Risk Factors in Sheep
3.1
A total of 400 serum samples were tested for T. gondii–specific antibodies. One hundred two sera were seropositive for T. gondii with an overall seroprevalence of 25.5% of all tested samples. In both univariable and multivariable logistic regression analyses, sex and age of sheep were risk factors associated with T. gondii seropositivity.
Multivariable logistic regression analysis showed that female sheep were two times more likely becoming T. gondii seropositive when compared to males ((AOR = 2.18; 95% CI: 1.38–3.47; p = 0.001)). Likewise, the young age group of sheep were three times more likely becoming T. gondii seropositive when compared to adult age groups (AOR = 3.04; 95% CI: 1.04–8.86; p = 0.041) as shown in Table 1.
Prevalence of Toxoplasmosis and Its Associated Risk Factors in Pregnant Women
3.2
Among 200 pregnant women tested for T. gondii antibodies, 56 were found to be seropositive with an overall prevalence of 28%. In multivariable logistic regression analysis, potential risk factors significantly associated with T. gondii seropositivity were age groups between 25 and 34, cat availability at home, close contact of pregnant women with cats, contact with garden soil, poor hand washing habit before eating, and drinking tap water were significantly associated with T. gondii seropositivity (Table 2).
After adjustment for possible confounder, adult age groups (25–34) of pregnant women were three times more likely to develop toxoplasmosis than younger age groups (AOR = 2.76; 95% CI: 1.07–7.14; p = 0.037). Pregnant women having cats in their home were six times more likely of becoming T. gondii seropositive than those who were not keeping cats in their home (AOR = 6.45; 95% CI: 2.37–17.52; p = 0.000). Pregnant women who had contact with garden soil were almost seven times more likely to become toxoplasmosis seropositive than those who did not have contact with garden soil (AOR = 6.74; 95% CI: 2.33–11.45; p = 0.000). Likewise, pregnant women who were unable to wash their hands frequently were 29 times more likely to acquire toxoplasmosis than those individuals washing their hands before eating (AOR = 29.5; 95% CI: 5.41–160.11; p = 0.000). We also found that pregnant women drinking tap water were eight times more likely to acquire T. gondii infection than those who use well water (AOR = 8.4; 95% CI: 2.54–28.08; p = 0.000) (Table 2).
Discussion
4
Toxoplasmosis is a widespread disease with high prevalence and public health importance. East Africa region is a high‐risk area of toxoplasmosis owing to a close association between humans and livestock, sociocultural practices, poor environmental hygiene, and poverty [14]. This study showed a seroprevalence 25.5% in sheep waiting for slaughter at Mandeeq slaughter house. This finding is consistent with the high prevalence of ovine toxoplasmosis in the nearby country, Somalia [15]. In this study, female and young sheep were significantly associated with seropositivity of toxoplasmosis. This could probably be related to reduced immunity owing to hormonal influences in females and reduced the exposure of lambs for oocysts [16].
Studies in Somalia also indicated that toxoplasmosis has been highly prevalent in human patients and pregnant women [12]. Our study in Hargeisa also indicated a high prevalence of toxoplasmosis (28%) in pregnant women who were attending ANC in Hargeisa Group Hospital, indicating that this disease could be endemic in the study area. We also observed a significant association of toxoplasmosis seropositivity with age category. Pregnant women who were in the age group 25–34 were more likely to develop toxoplasmosis than other age groups (AOR = 2.76; 95% CI: 1.07–7.14; p = 0.037). This age group (25–34) can be considered as the most childbearing age that needs proper public health policies [10]. Pregnant women who had cats in their home, close contact with cats, lack of hand washing before meal, contact with garden soil, and drinking of tap water had significant association with seropositive pregnant women. These findings are in line with the routes of toxoplasma transmission such as drinking oocyst contaminated water, and contact with the soil. It is also indicated that domestic cats were the major sources of ecosystem contamination [17]. Furthermore, poor hygiene regarding to meat handling practices and lack of compliance with minimum meat hygiene and food safety standards may explain the increased level of toxoplasmosis in pregnant women in Somaliland [18].
In conclusion, toxoplasmosis in sheep and pregnant women is highly prevalent in Hargeisa, Somaliland. Environmental contamination by infected cats, contaminated tap water, and poor personal hygiene might have contributed to the widespread nature of toxoplasmosis in the area. The role of cats in the epidemiology of toxoplasmosis and the overall hygienic practices related to food handling should not be overlooked in Hargeisa, Somaliland.
Author Contributions
Abdiqani Mohamed Jama: investigation, funding acquisition, formal analysis, resources, data curation, validation, methodology, writing – original draft, software, conceptualization. Taddesse Yayeh: supervision, writing – review and editing.
Ethics Statement
The authors confirm that the ethical policies of the journal, as noted on the journal's author guidelines page, have been adhered to, and the appropriate ethical review committee approval (protocol number 01/IRB/2022) has been received. The College of Agriculture and Environmental Sciences guideline in Bahir Dar University for the Care and Use of Animals were followed.
Conflicts of Interest
The authors declare no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1J. P. Dubey , “Toxoplasmosis in Sheep—The Last 20 Years,” Veterinary Parasitology 163, no. 1–2 (2009): 1–14.19395175 10.1016/j.vetpar.2009.02.026 · doi ↗ · pubmed ↗
- 2P. R. Torgerson , B. Devleesschauwer , N. Praet , et al., “World Health Organization Estimates of the Global and Regional Disease Burden of 11 Foodborne Parasitic Diseases, 2010: A Data Synthesis,” P Lo S Medicine 12, no. 12 (2015): e 1001920.26633705 10.1371/journal.pmed.1001920 PMC 4668834 · doi ↗ · pubmed ↗
- 3G. Saadatnia and M. Golkar , “A Review on Human Toxoplasmosis,” Scandinavian Journal of Infectious Diseases 44, no. 11 (2012): 805–814.22831461 10.3109/00365548.2012.693197 · doi ↗ · pubmed ↗
- 4J. G. Montoya and O. Liesenfeld , “Toxoplasmosis,” Lancet 363, no. 9425 (2004): 1965–1976.15194258 10.1016/S 0140-6736(04)16412-X · doi ↗ · pubmed ↗
- 5B. Edvinsson , M. Lappalainen , V. J. Anttila , A. Paetau , and B. Evengard , “Toxoplasmosis in Immunocompromised Patients,” Scandinavian Journal of Infectious Diseases 41, no. 5 (2009): 368–371.19229764 10.1080/00365540902783319 · doi ↗ · pubmed ↗
- 6C. Paquet and M. H. Yudin , “Toxoplasmosis in Pregnancy: Prevention, Screening, and Treatment,” Journal of Obstetrics and Gynaecology Canada 35, no. 1 (2013): 78–81.23343802 10.1016/s 1701-2163(15)31053-7 · doi ↗ · pubmed ↗
- 7G. Milne , J. P. Webster , and M. Walker , “ Toxoplasma gondii: An Underestimated Threat?,” Trends in Parasitology 36, no. 12 (2020): 959–969.33012669 10.1016/j.pt.2020.08.005 · doi ↗ · pubmed ↗
- 8Z. Zhou , H. I. A. Ortiz Lopez , G. E. Pérez , et al., “Toxoplasmosis and the Heart,” Current Problems in Cardiology 46, no. 3 (2021): 100741.33183832 10.1016/j.cpcardiol.2020.100741 · doi ↗ · pubmed ↗