A heart full of nails: complex management of multiple nail gun cardiac injuries
Shaun Abid, Anton Stolear, Stuart Zarich

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
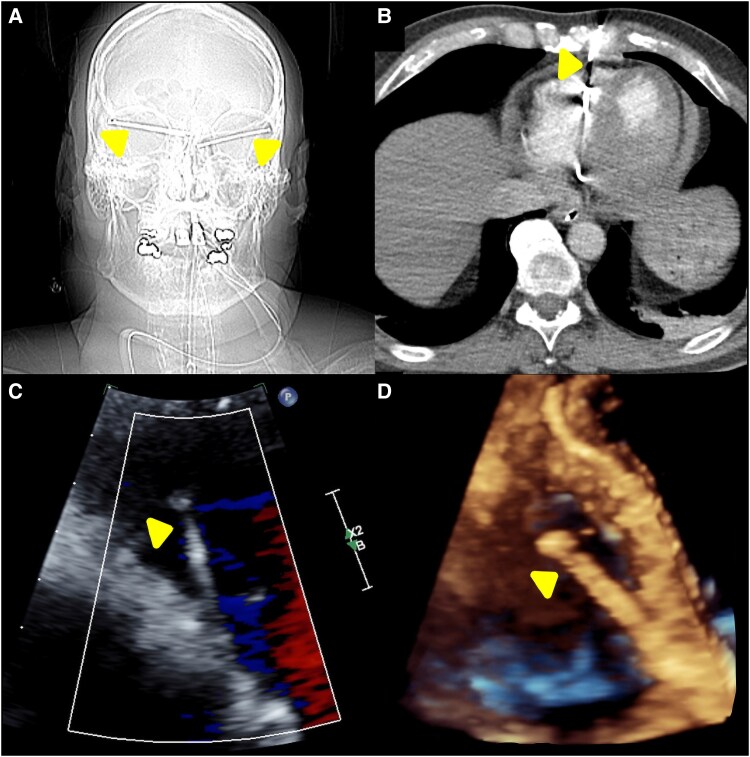 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTraumatic Ocular and Foreign Body Injuries · Trauma Management and Diagnosis · Cardiovascular Effects of Exercise
A 54-year-old male presented after a suicide attempt, suffering severe cardiac and extracardiac injuries from firing a nail gun into both temples (Figure 1A) and his chest. Imaging showed six 5 cm nails embedded in his heart: two in the left ventricle, two in the right ventricle, one traversing the ascending aorta into the left atrium, and one entering the right ventricle from the left parasternal chest wall (Figure 1B–D). These injuries resulted in haemorrhagic pericardial effusion with tamponade, acute aortic regurgitation, mitral valve/pulmonary artery perforations, and a ventricular septal defect.
Neurosurgical intervention was deemed secondary to the cardiac injuries. An emergency sternotomy was performed, evacuating 300 cc of blood from the pericardium and removing five intracardiac nails, while the sixth nail in the right ventricle was deemed too dangerous to remove due to the risk of significant vascular injury. Aortic valve replacement with a 27 mm Edwards bioprosthetic valve was required due to extensive damage to the non-coronary and left coronary cusps. Injuries to the septum, pulmonary artery, left atrium, anterior leaflet of the mitral valve, and left ventricle were repaired. Neurosurgery removed two nails from the right side of the head and one from the left. The patient required subsequent pulmonary valve replacement with a 29 mm Edwards Inspiris Resilia valve and mitral valve repair with a 36 mm annuloplasty band. Due to diffuse chest wall bleeding, re-exploration was required, during which bleeding was successfully controlled. Over the ensuing days, both cardiac and neurological status improved, and a psychiatric evaluation was initiated to address the underlying mental health concerns. At his 3-month follow-up, he was doing well, with a stable repeat echocardiogram.
This case highlights the challenges of managing cardiac trauma involving multi-chamber, large vessel, and valvular injuries, along with haemodynamic compromise. Prompt surgical intervention and multidisciplinary care are essential.
Consent: The patient's consent has been obtained for publication.
Funding: The authors report no specific funding related to this article.