A Case of Chronic Expanding Hematoma Following Extraperiosteal Paraffin Plombage After 50 Years
Daiki Hayashi, Naoko Ose, Hideki Nagata, Eiichi Morii, Yasushi Shintani

TL;DR
A man developed a rare chronic expanding hematoma 50 years after a historical paraffin plombage procedure for tuberculosis, requiring surgical removal.
Contribution
Reports a rare long-term complication of extraperiosteal paraffin plombage and advocates for surgical intervention in symptomatic cases.
Findings
Chronic expanding hematoma occurred 50 years after paraffin plombage for pulmonary tuberculosis.
Surgical excision confirmed the diagnosis and resolved the issue.
Late complications from paraffin plombage can be both benign and malignant.
Abstract
Chronic expanding hematoma (CEH) is a late complication of extraperiosteal paraffin plombage. Various late complications have been reported with this historical procedure, including expanding hematoma, paraffinoma, blood specimens complicating chronic empyema, and malignant tumors. A 75-year-old male presented with left-sided lateral chest pain. Fifty years prior, he had undergone a left upper lobectomy with extraperiosteal paraffin plombage for pulmonary tuberculosis. Three years before the current presentation, he had been admitted to another hospital with fever. At that time, a chest computed tomography (CT) scan showed the expanding plombage and a mass in the plombage. Upon referral to our institute, contrast-enhanced CT showed strong enhancement of part of the mass, and a CEH was suspected. The paraffin and hematoma were surgically removed. Pathological diagnosis was a CEH.…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
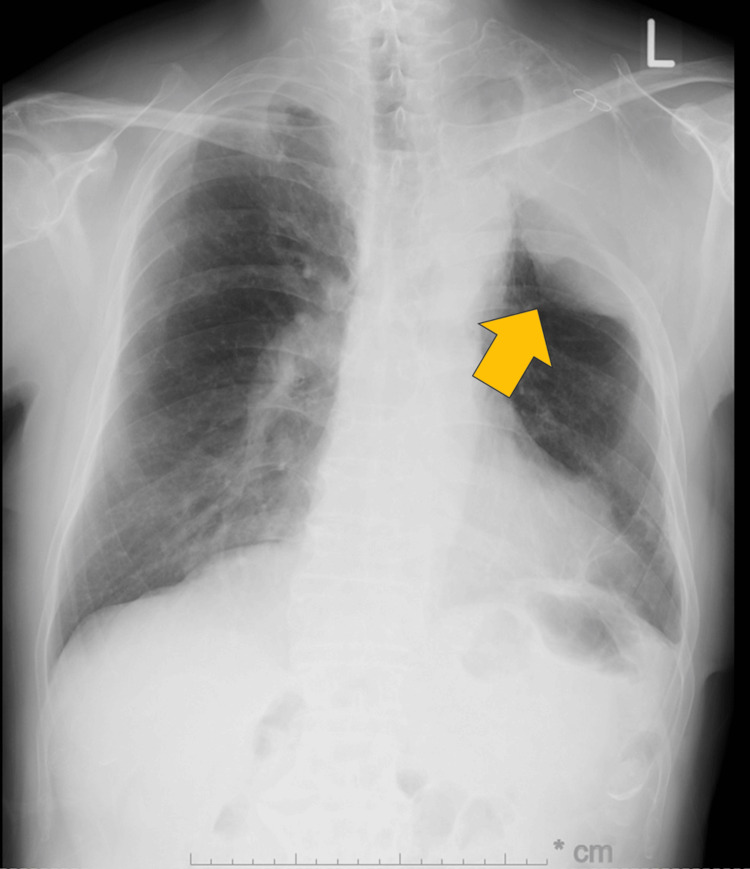 Figure 1
Figure 1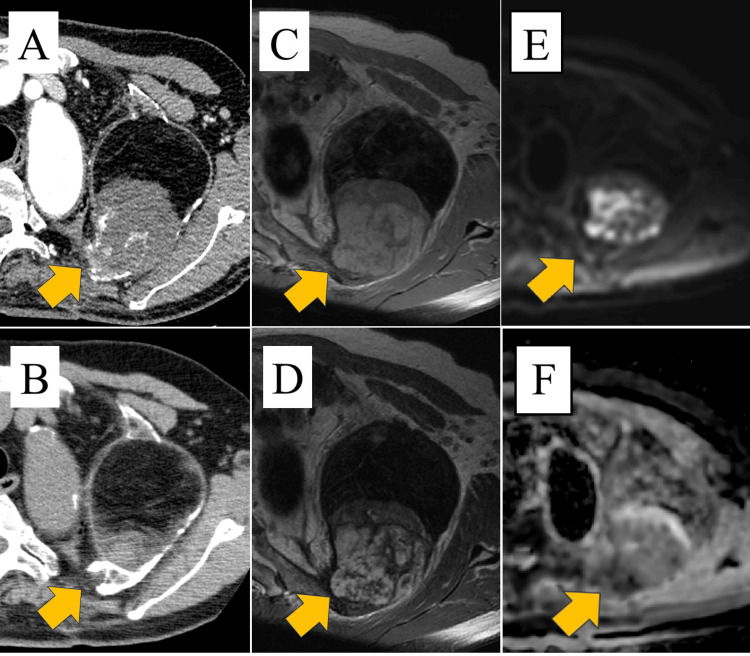 Figure 2
Figure 2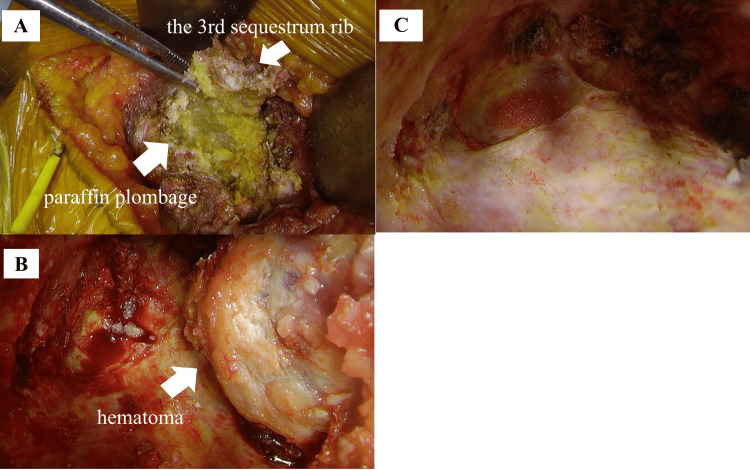 Figure 3
Figure 3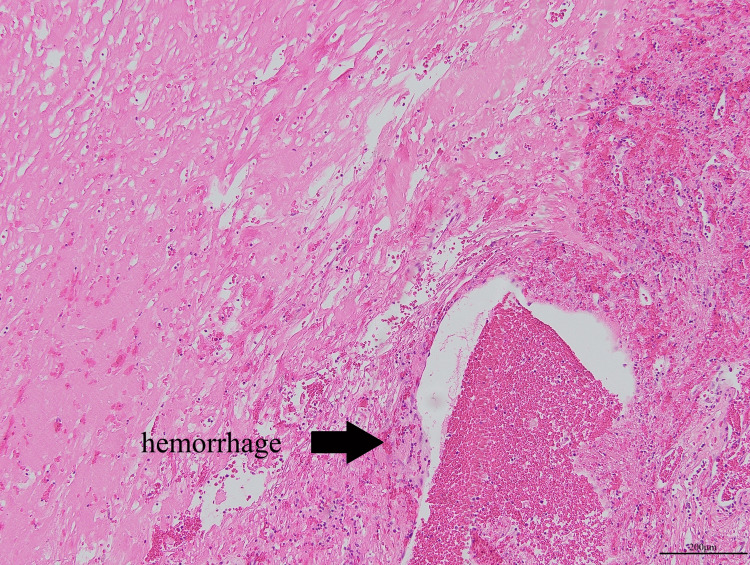 Figure 4
Figure 4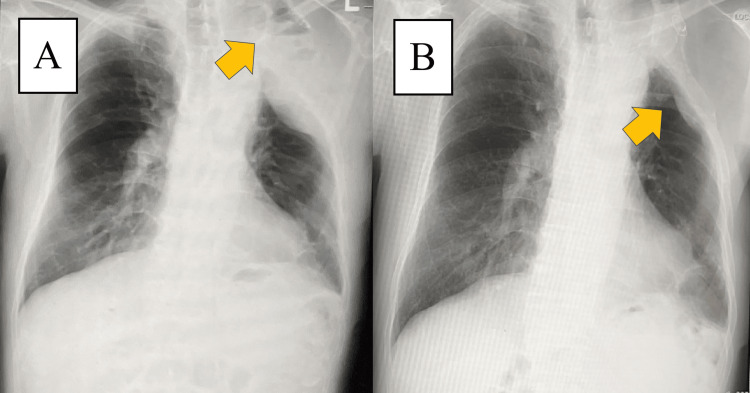 Figure 5
Figure 5| Author | Age (years) | Sex | Complications | Interval from plombage (years) | Treatment |
| Arai et al. [ | 79 | M | Paraffinoma | 47 | Surgery |
| Tanaka et al. [ | 57 | M | CEH* | 22.5 | Surgery |
| 44 | M | CEH* | 21 | Surgery | |
| 43 | M | CEH* | 21 | Surgery | |
| 65 | M | CEH* | 21 | Surgery | |
| 53 | M | CEH* | 17 | Surgery | |
| 50 | F | CEH* | 30.5 | Surgery | |
| 60 | M | CEH* | 27.5 | Surgery | |
| 67 | M | CEH* | 14 | Surgery | |
| Fujiwara-Kuroda et al. [ | 70s | M | CEH* | 48 | Surgery** |
| Horowitz et al. [ | 77 | F | Migration and pyothorax | 35 | Surgery |
| Isoda et al. [ | 75 | M | IgG4-related disease | 54 | Oral prednisolone |
| Our case | 75 | M | CEH* | 50 | Surgery |
| *chronic expanding hematoma **surgery and arterial embolization | |||||
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCase Reports on Hematomas · Spinal Hematomas and Complications · Venous Thromboembolism Diagnosis and Management
Introduction
Extraperiosteal paraffin plombage was used as a collapse therapy for pulmonary tuberculosis before the development of anti-tuberculosis drugs, which were invented by Adams et al. in the 1950s [1]. However, late complications such as expanding plombage, paraffinoma, blood specimens complicating chronic empyema, and chronic expanding hematoma (CEH) have been reported [2-6]. We report a case of CEH developing 50 years after extraperiosteal paraffin plombage.
Case presentation
A 75-year-old male had undergone left upper lobectomy and extraperiosteal paraffin plombage for treatment of tuberculosis 50 years ago. He was referred to our institute with left lateral chest pain when sneezing or coughing for a month. Laboratory investigations revealed a normal soluble interleukin (IL)-2 receptor level of 465 U/mL and an elevated neuron-specific enolase (NSE) level of 14.7 ng/mL, with no other abnormal findings.
Chest X-ray showed an extraperiosteal paraffin plombage space in the left upper lung field (Figure 1).
Chest X-ray findings Extraperiosteal paraffin plombage space was observed in the left upper lung field (arrow).
There were no significant changes in X-ray over the previous year. Chest contrast-enhanced computed tomography (CT) scan showed a 120 × 90 × 70 mm plombage space with calcification at the margins on the left chest wall and within the space, and a 70 × 65 × 52 mm spherical mass in contact with fat and the chest wall (Figure 2A). The mass was partially strongly contrasted. The mass and plombage space had expanded compared with the plain chest CT scan performed three years earlier (Figure 2B). Magnetic resonance imaging (MRI) showed a mass with low-to-slightly high intensity on T1-weighted images (Figure 2C) and a mosaic-like appearance with low-to-high intensity on T2-weighted images (Figure 2D). Diffusion-weighted imaging showed a mosaic appearance ranging from high to low signal intensity (Figure 2E). The apparent diffusion coefficient (ADC) map also showed a mosaic appearance ranging from high to low signal intensity (Figure 2F).
Chest CT and chest MR findings(A) Chest contrast-enhanced CT scan showing a plombage space with a 120 × 90 × 70 mm plombage space and a mass partly accompanied by a strong contrast effect in the plombage space (arrow). (B) A chest plain CT scan showed an 81 × 81 × 63 mm plombage space, and the size of the mass was 24 × 18 × 18 mm three years ago (arrow). (C) T1-weighted MR image showing a low-to-slightly high-intensity mass in the plombage space (arrow). (D) In the T2-weighted MR image, the mass had a low to high intensity and a mosaic-like appearance (arrow). (E) Diffusion-weighted imaging showed a mosaic appearance ranging from high to low signal intensity (arrow). (F) The apparent diffusion coefficient (ADC) map also showed a mosaic appearance ranging from high to low signal intensity (arrow).
Based on the enlarged plombage cavity, mass characteristics, and elevated NSE on blood tests, we suspected a CEH or pyothorax-associated lymphoma after paraffin plombage.
The surgical approach was through the third intercostal space; however, the third rib was sequestrated, and the paraffin was exposed (Figure 3A). We resected the perineurium and accessed the plombage space. The yellow paraffin was filled in solid form and removed. A hemorrhagic mass surrounded by a smooth, thickened capsule was identified on the mediastinal side (Figure 3B). When the mass with the capsule was removed, it bled from inside the mass easily. The plombage space was irrigated with 15 L of saline solution until no floating paraffin remained (Figure 3C). The operative time was 153 minutes, and the blood loss was 100 mL.
Operative findings(A) Paraffin was removed from the plombage space. (B) Solid hemorrhagic mass is on the mediastinal side in the space. (C) Removed hematomas from the space.
Gross examination revealed old hematomas surrounded by a fibrous capsule.
Histopathological examination confirmed CEH with necrotic tissue and hemorrhage (Figure 4). Bacterial culture tests submitted at the time of surgery were negative for both the empyema wall and paraffin.
Pathological findingsThe pathological findings showed necrotic tissue with some hemorrhage (H-E stain, ×100)
The patient was discharged from the hospital on postoperative day 8 without complications. Gradually, the chest pain improved, and it completely disappeared six months after the surgery. He had no recurrences during the two years of follow-up. On the chest X-ray one month after surgery, a pleural effusion and an air-fluid level were observed in the left upper lung field (Figure 5A). On the chest X-ray two years after surgery, the pleural effusion further decreased (Figure 5B).
Postoperative chest X-ray findings(A) On the chest X-ray one month after surgery, a pleural effusion and an air-fluid level were observed in the left upper lung field (arrow). (B) On the chest X-ray two years after surgery, the pleural effusion decreased (arrow).
Discussion
Extraperiosteal paraffin plombage was developed as a collapse therapy for pulmonary tuberculosis, involving the placement of paraffin between the rib and periosteum. This treatment was considered safe with no serious early complications, and it produced an adequate and permanent collapse, thus resulting in a cure for pulmonary tuberculosis [7]. However, various late complications have been reported following paraffin plombage (Table 1) [2-6]. The onset of late complications varies between 20 and 50 years postoperatively. Cases of paraffinoma with spinal paralysis and IgG4-related disease have been reported after paraffin plombage [3,4]. CEH-associated pyothorax and pyothorax-associated lymphoma have also been reported [8,9]. In our case, while the appearance period of the mass was unknown, the patient became aware of left lateral chest pain 50 years after paraffin plombage. This is the latest-onset case and demonstrates that late complications could occur even after more than 50 years.
CEH was first described by Reid et al. in 1980 [10]. Repeated microvascularization and hemorrhaging caused by chronic aseptic inflammation can lead to hematoma and expansion of the space with organized tissues over decades. If left untreated, CEH can cause respiratory failure due to mediastinal compression, and in some cases, it is difficult to distinguish malignant diseases such as malignant lymphoma. Therefore, surgical treatment is required [7,11]. The optimal treatment for CEH is complete surgical removal of both the hematoma and its capsule, because incomplete removal of the hematoma may result in recurrence of the hematoma. In this case, CEH was suspected based on CT findings showing an enlarged plombage space and mass. The elevated NSE levels prompted consideration of malignant lymphoma in the differential diagnosis. However, pathological examination showed no evidence of malignancy, suggesting that chronic inflammation caused by paraffin led to CEH and plombage space enlargement.
This patient was suspected of malignancy and underwent surgery; the result was benign CEH, but the chest pain disappeared postoperatively. CEH is also a disease that can cause serious symptoms if enlarged, and surgical curettage should be performed if there are symptoms or mass formation after paraffin plombage.
Conclusions
We report a case of CEH occurring 50 years after extraperiosteal paraffin plombage, which was successfully treated by surgical resection. This case highlights that CEH can develop long after extraperiosteal paraffin plombage, particularly when patients present with symptoms or mass enlargement in the plombage cavity. In such cases, differential diagnoses should include malignant tumors, such as malignant lymphoma. Surgical treatment is recommended not only to rule out malignancy but also to eliminate chronic inflammation.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Subscapular paraffin pack as a supplement to thoracoplasty in the treatment of pulmonary tuberculosis J Thorac Surg Adams WE Lees WM Fritz JM 37538522195114881204 · pubmed ↗
- 2Expanding hematoma after extraperiosteal paraffin plombage Surg Today Tanaka H Matsumura A Iuchi K 586589362006 https://doi.org/10.1007/s 00595-006-3216-71679479110.1007/s 00595-006-3216-7 · doi ↗ · pubmed ↗
- 3Paraffinoma with spinal paralysis 40 years after pleural plombage for tuberculosis Kyobu Geka Arai W Ohkawa M Takahashi Y 34434772201931268030 · pubmed ↗
- 4Coexistence of Ig G 4-related disease and reactive granuloma to paraffin plombage Cureus Isoda A Sairenji Y Mihara M Iriuchishima H Saito A 015202310.7759/cureus.40620 PMC 1035482937476122 · doi ↗ · pubmed ↗
- 5Late complications of plombage Ann Thorac Surg Horowitz MD Otero M Thurer RJ Bolooki H 803806531992157097410.1016/0003-4975(92)91440-k · doi ↗ · pubmed ↗
- 6Successful treatment for a large chronic expanding hematoma treated by pneumonectomy after arterial embolization Case Rep Pulmonol Fujiwara-Kuroda A Iwashiro N Ohara M Kaga K 193242020222022 https://doi.org/10.1155/2022/19324203522312210.1155/2022/1932420 PMC 8881156 · doi ↗ · pubmed ↗
- 7Extrapleural pneumonolysis with plombage Am J Surg Walkup HE Murphy JD 2452507819491813564010.1016/0002-9610(49)90338-4 · doi ↗ · pubmed ↗
- 8Non-Hodgkin's lymphoma of the pleural cavity developing from long-standing pyothorax. Summary of clinical and pathological findings in thirty-seven cases Jpn J Clin Oncol Iuchi K Aozasa K Yamamoto S 2492571919892681886 · pubmed ↗