Analyzing the Trends and Drivers Influencing Future Leadership in Medical Education in Iran
SAREH MEHNI, REZA DEHNAVIEH TIJANG, MOHAMMAD HASAN KESHAVARZI, SEYED ALIAKBAR FAGHIHI, SOOLMAZ ZARE

TL;DR
This study identifies key drivers shaping future leadership in Iran's medical education to help policymakers make better decisions.
Contribution
The study introduces a comprehensive analysis of 37 drivers of leadership in Iranian medical education using mixed methods and structural modeling.
Findings
The study identified 37 drivers of leadership in medical education, categorized into four types.
Meritocracy in selecting managers and international relations had the most significant impact.
Findings suggest that strategic planning around these drivers can improve decision-making in medical education.
Abstract
A key challenge for policymakers in medical education lies in grasping the future landscape of leadership. Without insights into emerging trends, they may face unforeseen issues, leading to expensive and inefficient decision-making. This study aimed at analyzing the trends and drivers influencing future leadership in medical education in Iran. In this research, we employed a descriptive-exploratory approach This study consists of systematic reviews and interviews that have been analyzed using Structural Equation Modeling with the help of MicMac software (version 6.1.2, 2003/2004: 3IE/EPITA, France). We conducted a systematic review according to PRISMA. A literature search was performed using databases including Medline, Web of Science, ProQuest Dissertation & Theses, Scopus Embase, and Persian studies from SID, and Magiran. The inclusion criteria for the study were the articles which…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
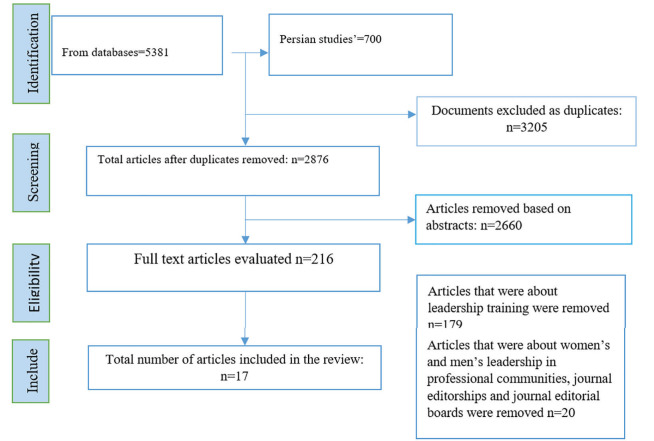 Figure 1
Figure 1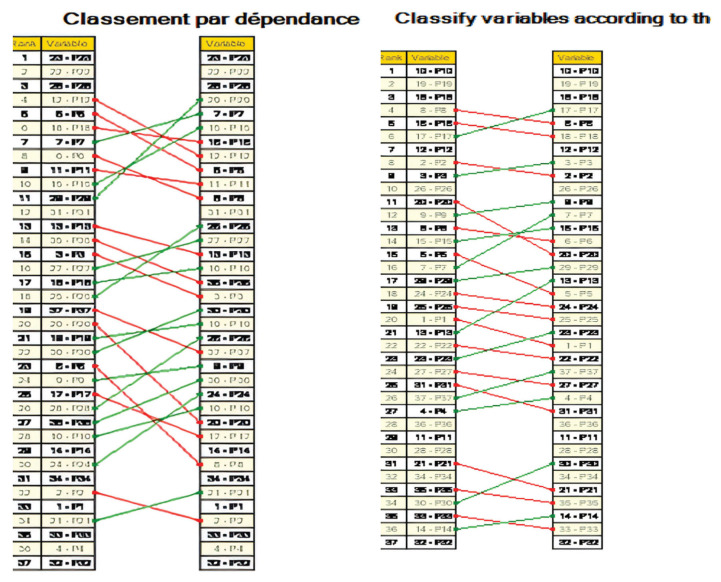 Figure 2
Figure 2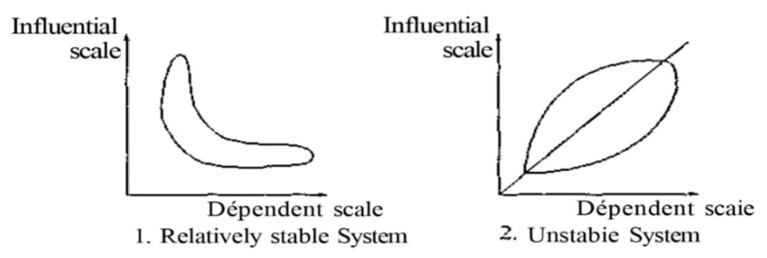 Figure 3
Figure 3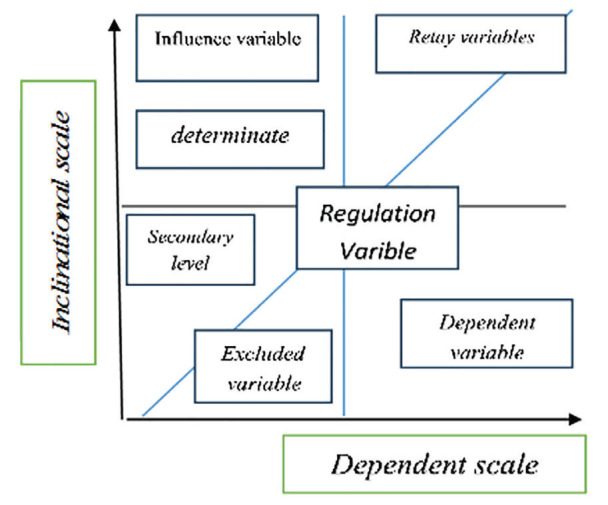 Figure 4
Figure 4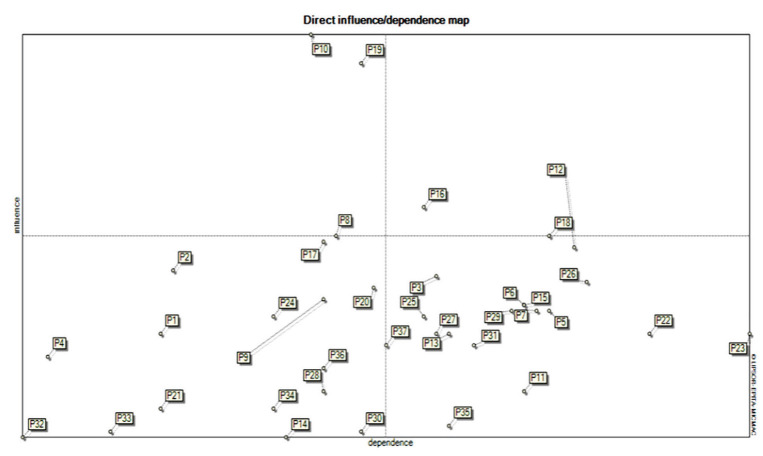 Figure 5
Figure 5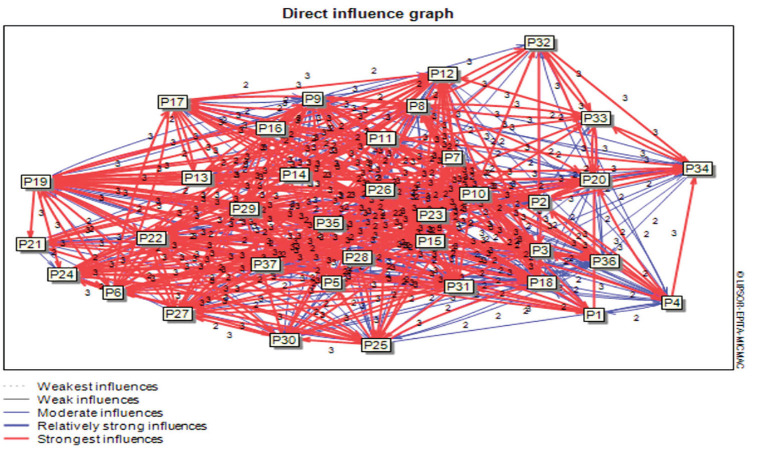 Figure 6
Figure 6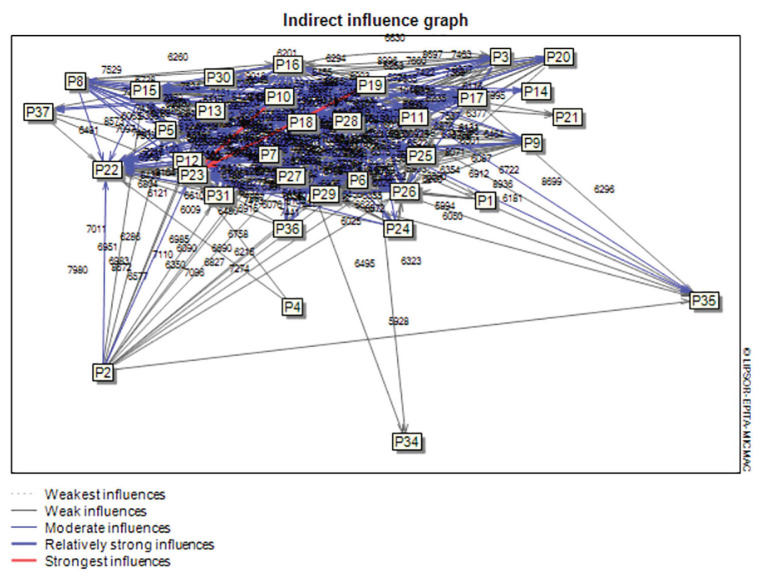 Figure 7
Figure 7| No. | Title | Corresponding Author, Year, and Country | Study type | Results |
|---|---|---|---|---|
| 1 | Healthcare educational leadership in the 21th century | Davinder Sandhu, 2019 ( | Descriptive | We are in the social media, information explosion, and IT ether, which is known as the post-modernity era. Post-modernity viewpoints of leadership must determine how one may free himself/herself from these limitations. If modernity was about order, then, one may consider that post-modernity is about doubts, uncertainties, concerns, and questions. The hierarchy of leadership must be adaptable. In transformation, it is necessary to move people from their classic organizational boxes into flexible fluid management systems functioning as liquid networks. We must cease putting people into little squares on staffing structure charts. It is necessary to look at teams. |
| 2 | Adaptive leadership during challenging times: Strategies for health professions educators: AMEE Guide Issue. 148 | Judy McKimma B. Subha, 2022 ( | AMEE Guide | As one of the most challenging conditions for leaders in health professions education and healthcare, the COVID-19 pandemic made them make decisions ‘on the fly’ and adapt themselves to new challenges while attending to the well-being of themselves, academics, their professional staff, clinical teachers, and learners, and also, maintaining the stability of programs and organizations. |
| 3 | Adopting artificial intelligence in dental education: A model for academic leadership and innovation | Nadim M. Islam, 2022 ( | Descriptive | Artificial intelligence can complement and strengthen human tasks and have a wide scope Impact on academia and healthcare. Adoption and planning by medical education leaders can enhance educational experiences and care delivery, and support current practices and future innovations. |
| 4 | Leadership in health and medical education: lessons from a symposium on health sector development in Ghana | Cephas K. Avoka1, 2023 ( | Symposium | Leadership challenges identified focused on leadership skills for an event organization, effective collaborative speaking and teamwork, and learning from recognizing the contributions of outstanding leaders in the health sector. |
| 5 | Educational Leadership and the Pandemic | David Gurr, 2020 ( | Descriptive | In terms of implications for leadership, the special issues of ISEA have reflected the fact that to help transition to remote education provision, in all education sectors, it has been necessary for teachers to remain more collaborative and for leadership to come from many. In addition, to upskill teachers quickly, rapid professional learning support has been necessary. In addition, it has been necessary to make leaders ready to be able to lead through crises. |
| 6 | Identifying challenges for academic leadership in medical universities in Iran | Bikmoradi Ali, 2010 ( | Qualitative | The main challenges to academic leadership could be categorized under three themes, : organizational issues (a very broad set of responsibilities and missions; inefficacy of academic governance; concerns with regard to the selection of managers); managerial issues (disagreement between responsibilities and authority; management styles; leadership capabilities), and organizational culture (low motivation; a boss-centered culture; inclination to governmental management). |
| 7 | ‘Important… but of low status’: male education leaders’ views on gender in medicine | Gunilla Risberg E. Eva, 2011 ( | Cross sectional | The results indicate that male faculty leaders embrace the importance of gender-related issues, gender as a determinant of health and, as bystanders, they had witnessed inequalities and the wasting of women’s competence. |
| 8 | Leadership aspirations among residents in obstetrics and gynecology in the United States: a cross-sectional analysis | Brindha Bavan, 2019 ( | Cross-sectional | Gender inequality in determining the goals of medical education leadership. The impact of targeted coaching, the presence of female role models in leadership, and the implementation of unconscious bias education in curricula should be explored as ways to overcome barriers for women and men alike. |
| 9 | Leadership, governance and management in dental education – new societal challenges | Townsend G. 2007 ( | Descriptive | The financial challenge, the balance between the responsibilities of medical education leaders to lead and manage employees in the school and their responsibilities to the senior managers who report to them, increasing student numbers and public budget pressures for greater accountability and universities are moving from a traditional academic approach to More corporate management styles are distanced. |
| 10 | Leading by Design: Lessons for the Future From 25 Years of the Executive Leadership in Academic Medicine (ELAM) Program for Women | Reshma Jagsi, 2020 ( | Descriptive | Regrettably, based on some convincing evidence, the failure to realize gender equity at the leadership level in academic medicine does not merely result from a slow pipeline, but, instead, is indicative of multiple complex reasons. |
| 11 | Requirements for effective academic leadership in Iran: A Nominal Group Technique exercise | Bikmoradi Ali, 2008 ( | Qualitative | Medical universities may have not enough statutory powers to prove the need to managerial system reform. In contrast, to these selection measures, the complexity of academic leadership does not enhance its stature in Iran due to the merging of medical education and health services, where great responsibilities exist. Academic leadership is further, exacerbated by problems such as lack of appropriate budget, supervision, and expansion of health issues. Arguably, selected academic leaders sometimes lack the required merits or appropriate qualifications, so they tend to be conservative. Perhaps these factors pose limitations among academic leaders and create unpleasant experiences about utilizing their authority. Criteria supporting academic leadership have been delegated to politicization, informal groups, and external forces. |
| 12 | Shifting norms and expectations for medical school leaders: a textual analysis of career advertisements 2000–2004 cf. 2010–2014 | Diane Gorskya and Anna MacLeodb, 2016 ( | Descriptive | In medical education and other higher education settings, contemporary drivers include funding constraints, regulatory and accreditation changes, increased organizational complexity, new governance models, performance management curriculum renewal, and enhanced expectations regarding accountability and transparent. |
| 13 | EDUCATIONAL LEADERSHIP IN HEALTH PROFESSIONS EDUCATION | Kristina Sundberg, 2019 ( | Thesis | The educational leaders expressed ambiguity toward their identity as educational leaders due to both the difficulties perceived in leading colleagues towards educational development and change and also unclear educational roles. The educational leaders rarely received feedback on their work from higher institutional levels, which caused them to feel that their role had a symbolic character. |
| 14 | Academic Medicine in the Military Health System: Problems and Solutions for Academic Leadership Development | Jessica T. 2018 ( | Descriptive | The high frequency of turnover of faculty members and the ranking structure of faculty members, the lack of experience of new faculty members, the subsequent lack of self-confidence and the desire to leave their positions, and the burnout of old faculty members are among the challenges of medical education leadership. |
| 15 | Women’s leadership in academic medicine | Lulu Alwazzan, Samiah S. Al-Angari, 2019 ( | Reviewed | Our review revealed that in medical schools, women had less access to leadership positions, the evidence showed <50% of leadership positions— programme directors, unit heads, or chairs, programme directors, or unit heads—were dedicated to female faculty members. |
| 16 | Develop tomorrow’s leaders in health and social care education. Case studies in leadership in medical and health care education. Special report 5. Newcastle-upon-Tyne: Higher Education Academy, Medicine Dentistry and Veterinary Medicine | McKimm J. 2004 ( | Case studies | maintain an appropriate work-life balance Managing both clinical and academic careers culture of their own organization Balancing competing agendas healthcare systems, with rapid change accountability the wider agenda. |
| 17 | Leadership development for clinicians: what are we trying to achieve? | McKimm, S. 2011 ( | Cross-sectional | Leaders work in complex systems, which are comprised of healthcare organizations university environments, and other professional and regulatory bodies. Navigation through such complexity necessitates knowledge of policy agendas, systems, strategy and organizations and understanding operational managerial procedures and processes. |
| Participants | Work Experience | Gender | Position | Situation | Managerial Experience in Medical University | Relevant Education in Health Higher Education/Health Policy | Managerial Experience in Ministry of Health and Medical Education |
|---|---|---|---|---|---|---|---|
| A | 20 | Male | Associate Professor | Tehran University of Medical Sciences | ✔ | ✔ | |
| B | 15 | female | Associate Professor | Kerman University of Medical Sciences | ✔ | ✔ | |
| C | 17 | Male | Assistant Professor | Shiraz University of Medical Sciences | ✔ | ✔ | |
| D | 23 | female | Associate Professor | Yazd University of Medical Sciences | ✔ | ✔ | |
| E | 31 | Male | Professor | Kerman University of Medical Sciences | ✔ | ✔ | |
| F | 22 | Male | Professor | Iran University of Medical Sciences | ✔ | ✔ | |
| G | 23 | Male | Professor | Tehran University of Medical Sciences | ✔ | ✔ | |
| H | 21 | Male | Professor | Mashhad University of Medical Sciences | ✔ | ✔ | ✔ |
| I | 15 | female | Assistant Professor | Shiraz University of Medical Sciences | ✔ | ✔ | |
| J | 30 | Male | Professor | Esfahan University of Medical Sciences | ✔ | ✔ | |
| K | 27 | Male | Professor | Tabriz University of Medical Sciences | ✔ | ✔ | |
| L | 23 | Male | Associate Professor | Gonabad University of Medical Sciences | ✔ | ||
| M | 25 | Male | Professor | Hormozgan University of Medical Sciences | ✔ | ✔ | |
| N | 24 | female | Associate Professor | Kerman University of Medical Sciences | ✔ | ✔ |
| Inclusion Criteria | Exclusion Criteria |
|---|---|
| Truly uncertain | Overlapping drivers |
| The greatest influence on shaping the future | Predictable and obvious |
| Non-intervention and Imitable |
| Session | Number of Drivers |
|---|---|
| Obtained from Scoping Review and Expert Interviews | 122 |
| Reviewed and Summarized in the First Session | 119 |
| Second Session | 101 |
| Third Session | 69 |
| Final Session | 37 |
| Indicator | Number of interationsMatrix size | Number of zeros | Number of ones | Number of twos | Number of threes | Number of P | Total | Fill rate | |
|---|---|---|---|---|---|---|---|---|---|
| Value | 2 | 37 | 324 | 351 | 360 | 334 | 0 | 1045 | 76.3 |
| Area of Influence | Drivers | Influence Score | Dependence Score | Code |
|---|---|---|---|---|
|
| The role and influence of networks and social media | 53 | 38 | P1 |
| Cultures and beliefs | 64 | 39 | P2 | |
| Demanding society | 63 | 60 | P3 | |
| Racial and ethnic issues | 49 | 29 | P4 | |
|
| Growth and development of technologies | 57 | 69 | P5 |
| Access to emerging technologies | 58 | 67 | P6 | |
|
| The motivation of human resources in the field of education | 57 | 68 | P7 |
| Poverty and inflation | 70 | 52 | P8 | |
| The state of financial resources | 59 | 51 | P9 | |
|
| Meritocracy in the appointment of the leaders | 105 | 50 | P10 |
| Interdepartmental cooperation | 43 | 67 | P11 | |
| Long-term planning based on vision and program | 68 | 71 | P12 | |
| Independence of the university and decentralization of education | 53 | 61 | P13 | |
| The attractiveness of the role of leadership in education | 35 | 48 | P14 | |
| System performance evaluation status | 58 | 67 | P15 | |
| Systemic view | 75 | 59 | P16 | |
| Political and managerial stability | 69 | 51 | P17 | |
| Evidence-based decision making | 70 | 69 | P18 | |
| International relations | 100 | 54 | P19 | |
|
| Lifestyle | 61 | 55 | P20 |
| Integration of education in healthcare | 40 | 38 | P21 | |
| Educational Impact Factors | Type of curriculum policy | 53 | 77 | P22 |
| System agility, new educational models and styles | 53 | 85 | P23 | |
| Awarding a joint degree from several universities | 56 | 47 | P24 | |
| The role of the university in acquiring skills and capabilities | 56 | 59 | P25 | |
| Social accountability of education | 62 | 72 | P26 | |
| Balance in performing the duties of academic staff members | 53 | 60 | P27 | |
| Convergence of sciences | 43 | 51 | P28 | |
| The importance of international accreditation | 57 | 66 | P29 | |
| The number of entries in specialized fields | 36 | 54 | P30 | |
| Competence of faculty members | 51 | 63 | P31 | |
|
| The course of demographic changes (population aging) | 40 | 47 | P34 |
|
| Climate change | 35 | 27 | P32 |
| Environmental crises | 36 | 34 | P33 | |
| Expatriation | 37 | 61 | P35 | |
| The status of access to human resources | 47 | 51 | P36 | |
| Population concentration in big cities | 51 | 56 | P37 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsInnovations in Medical Education · Health and Well-being Studies · Dental Education, Practice, Research
Introduction
In the contemporary world, universities are pivotal in the development of societies and the advancement of economic and social frameworks. As societies evolve from traditional to industrial and informational paradigms, the role of universities has significantly transformed. No longer merely centers for knowledge transfer, these institutions have emerged as major forces in the production of knowledge and technology. Economies driven by research and development regard universities as key organizations that can stimulate creativity and innovation. This shift is particularly in line with the growing societal demand for innovation and entrepreneurship. Consequently, it is anticipated that by 2050, universities will adopt structures and models specifically designed to enhance creativity, innovation, and entrepreneurship ( 1 ). Accordingly, there is growing uncertainty about whether universities will have the sustained ability to generate new and pertinent knowledge needed to meet today's demands. Such knowledge is crucial for promoting economic and social development, individual success, and social integration ( 2 ). In recent decades, universities have undergone significant changes and are continuing to evolve at a rapid pace ( 3 ). To thrive in this dynamic environment, modern universities must go beyond simply reacting to future developments ( 4 ). They need to anticipate future transformations and proactively steer these changes to achieve optimal outcomes ( 5 ). Effective leadership is essential for universities to navigate and meet these challenges successfully ( 6 ).
Leadership is about influencing individuals over the long term to reach specific group or organizational objectives ( 7 ). This process includes setting goals and strategies, boosting commitment, enhancing productivity, and fostering a dynamic, team-oriented culture ( 8 ). It also involves continuously structuring or restructuring conditions, perceptions, and expectations ( 9 ). Universities will require additional resources due to constrained government funding, and academics will be under increased pressure to adapt to new learning methods, updated teaching technologies, and educational competition ( 10 ). Furthermore, another study examining the future of higher education emphasized that revising the educational system should be a priority for future-oriented university programs ( 11 ). On the other hand, medical education, a critical component of higher education, has a direct impact on human life. Medical universities are responsible for training qualified personnel to meet the healthcare needs of the community effectively. Therefore, ensuring the quality and future of medical education is vital ( 12 ). Medical leaders must navigate evolving contexts, including medical advances, economic pressures, chronic and epidemic diseases, aging populations, and shifting doctor-patient relationships, all of which will shape future healthcare delivery methods ( 13 ).
The results of Hassanpor et al.'s study has revealed that futures studies in the field of medical education, based on competitive dynamics, are crucial. Consequently, researchers and specialists in medical education and future studies can utilize these components for their analyses ( 14 ). In a rapidly changing and uncertain environment, mapping the future becomes essential. Future studies help policymakers and managers to be adaptable and resilient ( 15 ). Identifying the forces shaping the future is a key aspect of this process ( 16 ). Therefore, examining the principles of foresight in medical education should not only address new issues and topics within the field but also emphasize monitoring the variables and actors that will play pivotal roles in the future of medical education ( 17 ). One of the most important steps in any foresight project is identifying the trends that affect the subject under study. Trends are essentially the forces or drivers that lead to changes in various fields. When conducting foresight on a specific topic, it is crucial to understand how this topic is shaped by the balance of social, technological, economic, political, and value-driven forces. These forces are primarily global in nature and are often referred to as global trends. By examining and monitoring the aforementioned variables, one can evaluate the issues and trends, gain a comprehensive understanding of the environment, identify emerging models and patterns, and infer potential driving forces and capacities for the future ( 14 ). However, future studies in the field of medical education remain a relatively unexplored and evolving domain with limited research ( 17 ).
Trend analysis, due to its accuracy and comprehensiveness, provides valuable insights for managers and leaders. Understanding trends facilitates appropriate planning to advance programs and anticipate the future. Given the crucial role of organizational leadership in the success of an organization, identifying and understanding trends amidst rapid changes in technology, society, politics, and economics are essential. This is particularly important for medical education leaders, enabling them to cope with crises and enhance their resilience, ultimately leading to success in a competitive world. Recognizing the trends allows leaders to formulate and outline various scenarios, focusing on the future while being responsive to the medical education system and society. Therefore, this study aimed to identify, categorize, and analyze the trends affecting the future of leadership and management in medical education in Iran.
Methods
This applied research utilizes a Sequential-Exploratory Mixed Method design, incorporating new methodologies from future studies ( 18 ). It combines both quantitative and qualitative models to achieve its goals. The primary aim of this research method is to identify and extract the drivers of change ( 19 ). This study was conducted in three main steps. The first step involved extracting key drivers from major databases and consulting with experts. In the second step, the research team identified these drivers. Finally, the third step assessed the impact of these identified drivers on the future of management and leadership in medical education.
The first step, which entails identifying and extracting key drivers, comprises two stages. In the first stage, this review follows the guidelines from the "Reviewers’ Manual of the Joanna Briggs Institute (JBI)" and the "Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) checklist"( 20 ).
Eligibility Criteria (Inclusion and Exclusion)
The PCC strategy guided our inclusion criteria: "P" for participants/population, "C" for the concept to be analyzed, and another "C" for the context. The inclusion criteria for the study specified that articles needed to contain one or more listed keywords, be published in a scientific journal, be written in English or Persian, be published between 2004 and 2024, have the full text available, and focus on educational leadership in medical schools.
Data Sources and Search Strategy
Articles were sourced from databases like Embase, Medline, APA PsycINFO, Scopus, CINAHLProQuest, Web of Science, and Persian studies from SID, Magiran, Civilica, and others. We used 35 keywords plus the main keyword and Boolean operators 'AND' and 'OR' to enhance relevance. For example, we surveyed the Web of Science using this strategy covering January 1, 2004, to August 12, 2024, including the Science Citation Index Expanded (SCI-EXPANDED), Emerging Sources Citation Index (ESCI), and Social Science Citation Index (SSCI).
Keywords used included: (search strategies)
• TS = ((educational OR training or academic or transformation* OR distributed or adaptive or change or school or college or university or institute) NEAR/1 (management or leadership*))
• TS = (Medicine OR Clinical OR Nursing or Dentistry or Pharmacy or 'Allied Health' or Paramedical OR Health Care OR 'Health Care' OR 'Health Professions?' or 'Health Professions?') NEAR/0 (Education OR Training 0R Teaching or teaching to a teacher or a teacher?))
Study Selection and Data Extraction
Data from various databases were entered into EndNote 20 (Clarivate Analytics, USA) to remove duplicates. Two reviewers (S. M. and M. K.) screened studies by abstracts and titles. Full texts of papers with unclear or no abstracts were reviewed. Differences were resolved through consensus with a third member (A, F) or group discussions. Data were collected using Excel, including publication year, authors, results, locations, and other details ( 21 ).
Study Characteristics
A total of 6081 records were identified. After removing duplicates and irrelevant records, 17 articles were selected for data extraction. Figure 1 shows the selection process. The selected papers, conducted in nine countries (seven from America, three from Australia, three from Sweden, two from Iran, one from Canada, and one from England), are summarized in Table 1.
PRISMA flowchart
The second stage aimed to finalize the first stage by sharing the identified drivers with experts. Experts were initially selected based on predefined criteria. They were initially selected according to predefined criteria. To be included, experts had to possess relevant education in medical education, health policy, or higher education management; occupy an executive or managerial position in higher health education or health policy; have more than 15 years of work experience; and be willing to participate in the study. Purposive sampling was used to select key informants, drawing on experts with significant experience in executive roles or education in higher health education, particularly those with over 15 years of experience in educational management and policymaking within the Ministry of Health and Medical Education and medical universities across Iran. Sampling continued until data saturation was reached, ultimately including 14 participants (Table 2). A snowball sampling method was employed to identify subsequent participants based on entry criteria until saturation was achieved. Experts consented to participate and completed a matrix of mutual effects questionnaires for subsequent studies. The process included scheduling face-to-face meetings to explain the study objectives and obtain informed consent. When face-to-face meetings were not possible, email or phone contact was arranged with the experts' permission. During this phase, the nature and objectives of the research and the need to complete two phases of the questionnaire were explained to the participants. Participants also guided the identification of additional experts for the study. Questionnaires were provided to participants at each stage, and arrangements were made for their timely return until data saturation was confirmed. Open-ended questions in the questionnaires allowed the participants to provide insights based on their experiences and perspectives, helping to identify effective drivers for the future leadership of medical education. Efforts were made to select participants with comprehensive experience in higher education in health and educational planning and policy-making to ensure their opinions contributed to identifying important drivers and influential factors.
All of the participants (100%) had managerial experience in medical universities. Additionally, 35% of them were managers and policymakers from the Ministry of Health and Medical Education. The inclusion and exclusion criteria for selecting drivers are shown in Table 3 ( 24 ).
In the second step, which focuses on identifying drivers, the research team carefully reviewed the results over four sessions (Table 4) and organized them using a horizontal approach ( 23 ).
In the final step, which involves assessing the impact, the goal was to evaluate the impact of the identified drivers on the future of leadership in medical education. Experts scored the results using a cross-impact matrix form. This matrix, which consisted of 37 rows and columns, was derived from the previously identified drivers. The degree of influence and responsiveness was determined using the following scale, with a grade (from 1 to 3) in the corresponding square: (0) no impact, (1) weak impact, (2) moderate impact, and (3) strong impact. The rows of the matrix represent the influence of key factors, while the columns represent their responsiveness. The data was analyzed using MicMac software ( 39 ).
Ethical Consideration
This study was approved by the Vice-Chancellor for Research as PhD dissertation and by the ethics committee of Shiraz University of Medical Sciences with the number IR.SUMS.REC.1403.015.
Results
The initial phase of structural analysis identified 122 drivers influencing the future management and leadership of medical education. After four regular sessions with the research team (Table 4), 37 of these drivers were ultimately selected and categorized into eight groups: technological, political, economic, social, health, education, environmental, and demographic. In the subsequent phase, a panel of experts completed the cross-impact matrix, which was then prepared for data analysis using the MicMac software. Table 4 illustrates the process the research team used to identify the final drivers from the extracted drivers, based on criteria for their inclusion and exclusion. From the 122 identified drivers, 37 were chosen and entered into the MicMac software for analysis.
Table 5 presents the results of the cross-impact analysis of 37 factors or variables influencing the future of leadership in medical education in Iran. This analysis is based on a 37×37 matrix, spanning 8 main dimensions: Technological, Political, Economic, Social, Health, Educational, Environmental, and Demographic.
The initial analysis of the matrix data and the cross-impact of the variables (Table 5) shows that the fill rate of the matrix is 76.3%. This suggests that the selected factors have strongly influenced each other, indicating that the system has been in a stable state. Out of 1045 assessable relationships in this matrix, 324 had a value of zero. This means that the factors either did not influence or were not influenced by each other.
In the structural analysis matrix, the sum of the numbers in the rows for each variable represents its degree of influence, while the sum of the numbers in the columns for each variable represents its degree of susceptibility. The analytical results of this matrix indicate that the variables "meritocracy in the appointment of the leaders" and "international relations" have the highest degree of influence. On the other hand, the variables "climate change" and "the attractiveness of leadership roles in education" have shown the lowest degree of influence (Table 6).
Based on the questionnaire data, which has been completed as a matrix, the MicMac software calculates relationships and assigns a numerical score to each driver. These drivers are then ranked based on their direct and indirect influence and their susceptibility to influence (Figure 2).
Ranking of Variables based on Influence and Dependence
The scatter plot in Figure 3 illustrates the distribution and dispersion of the variables, indicating the level of stability or instability of the system. This initial analysis provides a foundational understanding of the status of the system, which influences the subsequent analysis of the variables.
System Stability or Instability
In this study, the distribution pattern of the variables forms an L-shape (Figure 3), indicating that some variables have high influence while others have low influence ( 40 ). The role of each factor in the system can be identified using the scatter plot of factors on the influence and impact coordinates (Figure 4) ( 41 ). Results from the MicMac software show that the important influencing factors (Northwest quadrant) include three components that act as significant drivers of the system. These drivers have the potential to affect other drivers within the system. Influencing variables are the most critical components, as system changes depend on them, and control over them is crucial. The reinforcing factors (Northeast quadrant) include three highly influential and highly influenced components. These bidirectional components have the potential to both influence and be influenced. Attention to these components, also known as trust factors, is essential as they can potentially disrupt the stability of the system.
Spatial Position of Different Variables in the Perceptual Diagram Using the MicMac Method (Goude & Associates, 1999)
The independent components (Southwest quadrant) include 15 components with low influence and low impact. It is suggested that the evolution of these variables does not relate to the current system dynamics, and they can be removed from the system. Finally, the dependent components (Southeast quadrant) include 16 components with low influence but high impact. Changes in the drivers lead to direct observable effects on these components, also referred to as output variables (Figure 5).
Scatter Plot of Variables
The graphical representation shows the variables affecting the future of medical education leadership in Iran. These figures illustrate the drivers' direct and indirect impacts on other drivers within the system. The influence of drivers is categorized as strongest, strong, moderate, and weak (Figure 6).
Scatter plot of Direct Impact of Factors
The impact graph serves as a visual tool to display the relationships between variables and how they influence each other. In this graph, red and blue lines are used to differentiate the type and intensity of the influence.
Red lines represent a strong influence between the variables. In other words, they indicate when one variable significantly affects another, while blue lines, with varying thicknesses, indicate moderate to weak relationships between the variables. The thickness of the blue line signifies the strength of the influence; the thicker the line, the stronger the influence.
This type of graph helps researchers and analysts easily observe complex relationships between variables and gain a better understanding of how they interact with one another. It provides a clear and intuitive visualization of how different factors affects the system, highlighting both strong and subtle connections (Figure 7).
Scatter plot of indirect effects of factors
From all the assessed relationships in the matrices created by the software, relationships with low, medium, and high values were distinguished. The analysis revealed that the components of meritocracy in managerial selection and international relations had the greatest influence. Meanwhile, the components of the system agility and curriculum policy exhibited the highest level of impact on the future of educational management and leadership (Table 6).
Discussion
This study aims to identify the driving forces shaping the future of management and leadership in medical science education over the next 20 years. A scoping review and expert opinions helped identify and categorize 37 drivers into eight categories. Using MicMac software, we analyzed the impact of each driver on the others. Our findings show that the most influential drivers for the future of medical science education management and leadership are meritocracy in selecting educational leaders and the international communication within the education sector. Competencies are measurable patterns of abilities, skills, and behaviors that distinguish between strong and weak organizational performance ( 42 ). According to Brown et al., competency is a capability that includes personal characteristics, skills, and knowledge necessary to achieve an organization’s macro and strategic goals ( 43 ). The success of an organization, particularly regarding human resources, significantly depends on the competencies of its senior managers. Often, weaknesses or deficiencies in organizational performance are attributed to mismanagement. Therefore, having effective managers selected based on merit, who possess unique behaviors, skills, knowledge, attitudes, and personality traits, is crucial for organizational success ( 44 , 45 ). Dalvi et al. proposed a specialized competency model for leaders of medical sciences universities, which categorizes 43 subscales into 18 general categories within a paradigm model. This model encompasses causal factors, contextual conditions, intervening conditions, strategies, and consequences ( 46 ). Our study has also highlighted that international interactions are another significant driving force impacting the future of management and leadership in medical education. The internationalization of higher education involves incorporating international, intercultural, and global dimensions into university goals and functions, including teaching, learning, research, and services ( 47 ). Today's universities, influenced by global events and conditions, play a pivotal role in enhancing scientific and educational exchanges between nations and cultures. This role is shaped by two parallel phenomena: globalization, which emphasizes unification, and internationalization, which focuses on cooperation and partnership ( 48 ). As to achieving a desirable level of internationalization in higher education, a study by Hamidifar et al. (2023) identifies four crucial areas to be managed and led: conducting an analytical study of the environment, developing a coherent and targeted strategic program, implementing and organizing infrastructures, and monitoring and evaluation. According to the researchers, with effective leadership and management, strategic planning, and the continuous execution of related activities, the future of higher education internationalization in Iran is potentially promising ( 49 ). Furthermore, a study conducted by Wittenberg ( 50 ) emphasized that challenges such as shaping community knowledge, creating employment, integration, internationalization, quality focus, competitiveness, and the development and use of new forms of education and learning are likely to become defining trends in the future of higher education, supporting the findings of the current study. Knight (2013) ( 48 ) argues that while internationalization transforms higher education, globalization reshapes the global landscape. However, other studies suggest that internationalization also brings challenges, particularly if colleges and universities rely heavily on international students. Internationalization impacts not only those who participate in it but also affects what is learned, how it is learned, and where it is learned ( 51 ).
Limitation
The research faced limitations in identifying trends due to restricted access to certain credible sources. Only sources with full texts available through targeted searches were included in the scoping review. This may have led to the omission of some important and influential texts, potentially affecting the comprehensiveness of the findings. Therefore, future research should employ a broader range of data collection methods. Additionally, given the busy schedules of experts and their responsibilities within the Ministry of Health and medical universities, the timing, location, and type of interviews were designed to facilitate their participation.
Conclusion
This study identified 37 components across 8 dimensions as the key factors influencing the future of medical education management and leadership. The research findings suggest that the overall pattern of variable dispersion, based on interaction effects analysis, indicates a stable environmental system. Within this system, the trends affecting medical education leadership demonstrate consistent influence and susceptibility. The components of meritocracy in managerial selection and international relations are identified as having the greatest impact on the future of medical education management and leadership. By understanding and planning around these influential and susceptible components, managers and policymakers can gain foresight. This foresight enables them to make current decisions and actions more effective in pursuing a desirable future by systematically improving decision-making processes, revising procedures, and determining appropriate strategies in medical education leadership.
Recommendation
The findings of this research suggest that managers, policymakers, and decision-makers in the field of medical education should focus their strategies on two main factors: meritocracy in the selection of educational leaders and enhancing international communications. Concentrating on these areas allows them to play a critical role both in Iran and globally. Emphasizing meritocracy ensures that educational leaders possess the necessary qualifications, while fostering international communications promotes collaboration and knowledge exchange with other countries. This approach not only improves the quality of education but also elevates the status of medical education on an international scale.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Moscardini AO Strachan R Vlasova T The role of universities in modern society Studies in Higher Education 202247481230
- 2Duerrenberger N Warning S Corruption and education in developing countries: The role of public vs. private funding of higher education International Journal of Educational Development 20186221725
- 3Vincent-Lancrin S Building future scenarios for universities and higher education: an international approach Policy Futures in Education 200422245
- 4Munck R Mc Connell G University strategic planning and the foresight/futures approach Planning for Higher education 2009383140
- 5Khoadyar E Mazari E Khabazeh K Maleki M Explanation Role of Employeesʼshuman Capital of higher Education Centersontheir Tendency Toorganizational innovation (Case: University of Birjand) Journal of New Approaches in Educational Administration 20156216384
- 6De Wit H Hunter F Howard L Egron-Polak E Internationalisation of higher education Brussels: European Parliament 201510444393
- 7Tingvoll WASæterstrand T Mc Clusky LM The challenges of primary health care nurse leaders in the wake of New Health Care Reform in Norway BMC nursing 201615182790443510.1186/s 12912-016-0187-x PMC 5121988 · doi ↗ · pubmed ↗
- 8Arroliga AC Huber C Myers JD Dieckert JP Wesson D Leadership in health care for the 21st century: challenges and opportunities The American Journal of Medicine 2014127324692428017710.1016/j.amjmed.2013.11.004 · doi ↗ · pubmed ↗