Laparoscopic appendectomy and cholecystectomy in a 2-year-old with acute suppurative appendicitis and gallbladder torsion: a case report
Jian Sun, You-Cheng Zhang, Chun-Hui Gu

TL;DR
A 2-year-old child with appendicitis was also found to have a rare gallbladder torsion, which was successfully treated with laparoscopic surgery.
Contribution
This case highlights the importance of examining the gallbladder during laparoscopic appendectomy in children.
Findings
A 2-year-old had both acute appendicitis and gallbladder torsion confirmed via laparoscopy.
Laparoscopic cholecystectomy was performed alongside appendectomy without complications.
Postoperative recovery was uneventful despite a brief upper respiratory infection.
Abstract
Pediatric gallbladder torsion is a rare but potentially life-threatening cause of acute abdomen. The first case was reported in the 19th century, yet the precise pathogenesis remains unclear. Due to its nonspecific symptoms, gallbladder torsion in children is frequently misdiagnosed as more common conditions, such as acute appendicitis, cholecystitis, or gastrointestinal infections. A 2-year and 4-month-old boy was admitted to our emergency department with abdominal pain, fever, and vomiting. Initial blood tests revealed a white blood cell count of 13.13 × 109/L, neutrophil percentage at 76.1%, and an absolute neutrophil count of 9.99 × 109/L. Abdominal CT indicated thickened gallbladder walls, a partially blurred appendix margin, an intraluminal dense shadow, and multiple enlarged lymph nodes, along with pelvic effusion. A diagnosis of acute appendicitis was made. Emergency…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
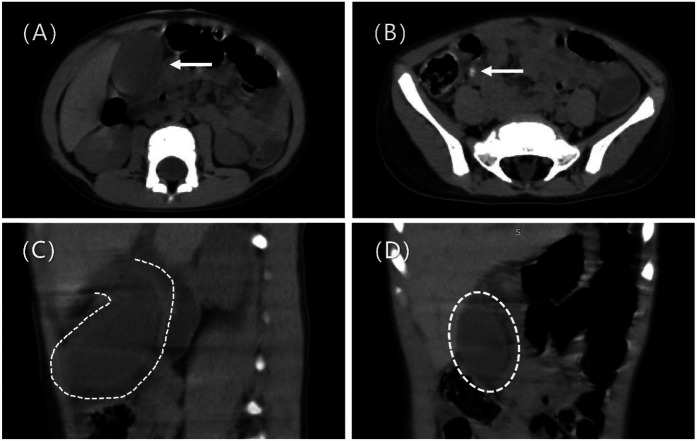 Figure 1
Figure 1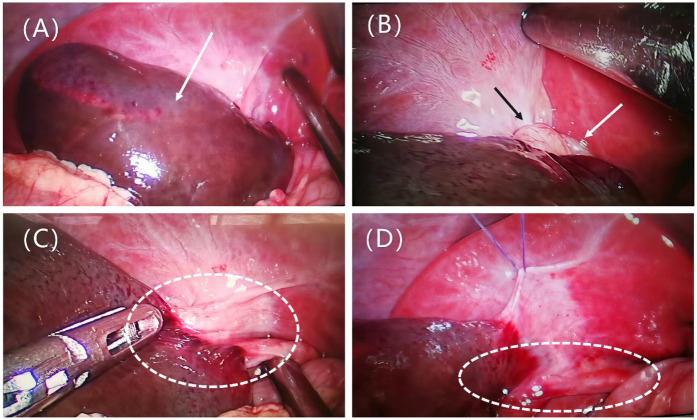 Figure 2
Figure 2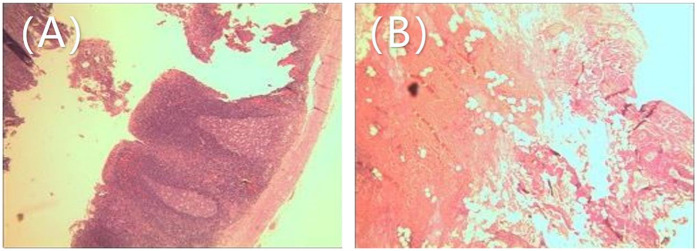 Figure 3
Figure 3| Clinical data | Total | |
|---|---|---|
| Gender | ||
| Male | 22 | 73.33% |
| Female | 8 | 26.67% |
| Mean age, years (range) | ||
| Male | 8.77 | (2, 16) |
| Female | 6.88 | (1, 17) |
| Overall | 8.2 | (1, 17) |
| Clinical manifestations | ||
| Vomiting | 22 | 73.33% |
| Abdominal pain | 30 | 100.00% |
| Fever | 17 | 56.67% |
| Physical examination | ||
| Right upper abdominal tenderness | 28 | 93.33% |
| Muscle rigidity | 15 | 50.00% |
| Poor mental status | 7 | 23.33% |
| Abdominal distension | 4 | 13.33% |
| Diminished bowel sounds | 3 | 10.00% |
| Periumbilical tenderness | 3 | 10.00% |
| Laboratory tests | ||
| Elevated white blood cells | 23 | 76.67% |
| Elevated CRP | 9 | 30.00% |
| Elevated liver enzymes | 6 | 20.00% |
| Imaging features | ||
| Nonspecific | ||
| Asymmetric gallbladder wall thickening | 23 | 76.67% |
| Gallbladder enlargement | 20 | 66.67% |
| Ascites | 14 | 46.67% |
| Gallbladder hydrops | 4 | 13.33% |
| Biliary dilation | 2 | 6.67% |
| Gallstones | 0 | 0.00% |
| Specific | ||
| Horizontal long axis of gallbladder | 6 | 20.00% |
| No blood flow signal in gallbladder wall | 7 | 23.33% |
| Figure of eight sign | 2 | 6.67% |
| Whirl sign | 1 | 3.33% |
| Beak sign at gallbladder neck | 5 | 16.67% |
| Site of torsion | ||
| Duct | 16 | 53.33% |
| Neck | 8 | 26.67% |
| Body | 2 | 6.67% |
| Not mentioned | 4 | 13.33% |
| Angle of torsion | ||
| Less than 180° | 0 | 0% |
| 180° | 6 | 20% |
| More than 180° | 19 | 63% |
| Not mentioned | 5 | 17% |
| Surgical methods | ||
| Open cholecystectomy | 15 | 50.00% |
| Laparoscopic cholecystectomy | 15 | 50.00% |
| Course prolongation | 2 | 6.67% |
| GT caused by abdominal trauma | 2 | 6.67% |
| Author, year | Age (years) | Gender | Preoperative diagnosis | Time from onset to surgery (days) | Operation time (min) | Treatment for cystic duct | Complications | Postoperative hospital stay (days) |
|---|---|---|---|---|---|---|---|---|
| Kimura et al. ( | 11 | M | GT | 1 | 65 | NA | None | 4 |
| Matsuda et al. | 7 | F | GT | 2 | NA | NA | None | 3 |
| Inoue et al. ( | 9 | M | GT | 4 | NA | NA | None | 4 |
| Farnsworth et al. ( | 6 | M | Appendicitis | 1 | NA | NA | None | NA |
| Musthafa et al. ( | 17 | F | biliary colic | 1 | NA | Endoloop | None | 2 |
| Uemura et al. ( | 3 | M | GT | 3 | 104 | Endoloop | None | 6 |
| Hoshi et al. ( | 5 | M | GT | NA | NA | NA | None | NA |
| 13 | M | GT | NA | NA | NA | None | NA | |
| Kruger et al. ( | 16 | M | Appendicitis | 2 | NA | NA | None | 2 |
| Lemons et al. ( | 12 | M | Cholecystitis | 3 | NA | Hem-o-lok® clips | None | 1 |
| Nuyts et al. ( | 1 | F | GT | 2 | 65 | Hem-o-lok® clips | None | 3 |
| Ren et al. ( | 6 | F | GT | 2 | 95 | Non-Absorbable Suture (4–0) | None | 6 |
| Tadesse et al. ( | 7 | M | GT | 3 | NA | NA | None | 4 |
| Tiep et al. ( | 5 | F | GT | 1 month | NA | NA | None | 7 |
| Yi Sun et al. ( | 13 | M | Cholecystitis | 11 | 99 | Endoloop | None | 4 |
| Present case | 2 | M | GT,Appendicitis | 0 | 120 | Hem-o-lok® clips | None | 19 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGallbladder and Bile Duct Disorders · Pediatric Hepatobiliary Diseases and Treatments · Congenital Anomalies and Fetal Surgery
Introduction
Gallbladder torsion is a rare cause of acute abdomen in children, typically occurring in those with anatomical abnormalities of the gallbladder (1). The condition is primarily characterized by acute right upper quadrant pain, nausea, vomiting, and fever, which can easily be mistaken for other acute abdominal conditions such as acute appendicitis (2). If left untreated, it may result in gallbladder ischemia, necrosis, or even biliary peritonitis (1). Therefore, early recognition and prompt surgical intervention are critical for favorable outcomes. Here, we present a successful case of laparoscopic appendectomy and cholecystectomy in a child with acute suppurative appendicitis complicated by gallbladder torsion.
Case report
A 2-year and 4-month-old boy presented to the emergency department with abdominal pain, fever, and vomiting persisting for one day. On physical examination, the abdomen was soft with generalized tenderness, pronounced pain at McBurney's point, rebound tenderness, and muscle guarding in the right lower quadrant, without palpable masses. Laboratory findings included elevated white blood cells at 13,130/µl, a neutrophil percentage of 76.1%, and an absolute neutrophil count of 9,990/µl, while C-reactive protein levels were within normal limits. An abdominal CT scan showed no significant intra- or extrahepatic bile duct dilation, but it indeed shows thickening of the gallbladder wall, gallbladder fluid accumulation (Figure 1A), and suspected gallbladder torsion (Figures 1C,D), a partially indistinct appendix margin, an intraluminal dense shadow (Figure 1B), multiple enlarged lymph nodes, and pelvic effusion. The patient was admitted to the pediatric surgery department for suspected acute appendicitis.
Shows preoperative imaging findings. (A) Preoperative CT axial scan shows thickening of the gallbladder wall and accumulation of fluid in the gallbladder (arrow). (B) Preoperative CT axial scan shows the local margin of the appendix is blurred, and a linear dense shadow is seen within the appendix lumen, suggestive of appendicolith (arrow). (C) Preoperative CT sagittal scan shows a floating gallbladder, with only the gallbladder neck connected to the liver (dashed line). (D) Preoperative CT coronal scan shows a distended, floating gallbladder (dashed line).
Emergency laparoscopic surgery was performed through a 5 mm umbilical incision with a 5 mm trocar and camera. Two additional 5 mm incisions were made along the left rectus abdominis muscle and the midpoint between the umbilicus and the pubic symphysis. Standard laparoscopic appendectomy procedures for pediatric acute appendicitis were followed. The appendix was found to be congested, swollen, and covered with purulent exudate. Following the appendectomy, the entire small intestine was examined, revealing no significant abnormalities. The gallbladder, located in the subhepatic region, appeared blackened with severe edema and was twisted 360° counterclockwise at the cystic duct and mesentery level (Figures 2A,B). The gallbladder was restored to its natural position through clockwise torsion, and the mesentery was suspended and unfolded. After 20 min, no color change was observed in the gallbladder, and significant edema was noted in the cystic duct, indicating possible gallbladder necrosis (Figures 2C,D). The free mesentery was isolated, and the cystic artery and cystic duct were doubly ligated using Hem-o-Locks, followed by cholecystectomy. The procedure lasted 120 min, with minimal intraoperative blood loss. Postoperative histopathology revealed gallbladder wall congestion, edema, and vascular dilatation (Figure 3).
Presents intraoperative findings. (A) Distended gallbladder with blackened color (arrow). (B) Exposure of the gallbladder neck, showing the gallbladder twisted counterclockwise by 360° at the cystic duct and mesenteric level, with the mesentery (black arrow) and cystic duct (white arrow) twisted together. (C) The gallbladder is restored to its natural position by clockwise torsion, with a slight mesentery connection to the liver, classified as Type II according to Gross. The cystic duct is visible (dashed line). (D) The mesentery is suspended and unfolded; after 20 min, there is no color change in the gallbladder, and significant edema is observed in the cystic duct (dashed line).
Postoperative pathological findings: (A) appendix: congestion and fibrinous purulent exudate on the serosal surface. (B) Gallbladder: Congestion, edema, and vascular dilation of the gallbladder wall, with infiltration of inflammatory cells.
On the 5th day post-surgery, the child developed fever and cough, prompting a consultation with the pediatric respiratory department. A chest x-ray revealed right-sided pneumonia. The child was treated with antibiotics, nebulization, and antiviral therapy as symptomatic treatment. After three consecutive negative nucleic acid tests for the novel coronavirus, the child was transferred to the pediatric respiratory department on the 9th postoperative day. The child was discharged on the 19th postoperative day without any complications. Follow-up visits were conducted at one and three months post-surgery. Physical examinations and laboratory tests (including complete blood count and biochemical tests) showed no abnormalities.
Discussion
Gallbladder Torsion is more commonly seen in the elderly and adult females. The earliest reported case of adult gallbladder torsion dates back to 1898, reported by the surgeon Wendel AV (3).Gallbladder torsion is an infrequent diagnosis in pediatric patients, typically occurring in those aged 1–17 years (4, 5), with the youngest reported patient being 1 years old (2, 6–11). The male-to-female ratio is approximately 11:4. Levard et al. (1) documented that out of 11 pediatric patients diagnosed with gallbladder torsion, 2 succumbed to misdiagnoses. The rarity and non-specific clinical manifestations contribute to the challenges in diagnosis. Common factors associated with gallbladder torsion include: (1) Congenital anatomical abnormalities: A floating gallbladder refers to a condition where the gallbladder is completely within the peritoneum, suspended in a floating state. The only mesentery attachment is at the gallbladder neck and cystic duct. The gallbladder duct is suspended below the liver, in a floating position (12, 13). Due to the high mobility of the gallbladder, it is prone to torsion along the axis of the cystic duct and the cystic artery (14). This case is of this type. (2) Acquired anatomical abnormalities: The incidence of gallbladder torsion is higher in the elderly, as the tissue structures around the gallbladder and the supporting fatty tissue gradually shrink with age. Tissue degeneration and reduced elasticity cause the gallbladder to droop, lengthening the mesentery (15, 16). Additionally, the motility of the stomach, duodenum, and transverse colon, as well as external factors such as physical labor and sudden changes in posture, can also induce gallbladder torsion (17). The acute onset of right upper quadrant pain is a common presenting symptom, often accompanied by tenderness or muscle guarding. Nausea and vomiting are frequently observed, while low-grade fever is possible but high-grade fever is uncommon. Laboratory tests typically show non-specific inflammatory markers, such as elevated white blood cell counts.
Conventional imaging techniques like ultrasonography and CT scans can assist in preoperative diagnosis, but most cases are diagnosed intraoperatively. CT and ultrasonography may show signs such as cystic duct torsion, abnormal gallbladder positioning, gallbladder wall thickening, and acalculous distension (7). If a floating gallbladder is detected on contrast-enhanced CT, with reduced blood flow towards the gallbladder wall, or the presence of the beak or spiral sign at the gallbladder neck, gallbladder torsion should be considered. MRI is considered the most valuable tool for preoperative confirmation, as it can clearly depict the anatomical relationship between the gallbladder and bile ducts, as well as the torsion axis (7). In cases where imaging results are inconclusive, laparoscopy can both diagnose and treat gallbladder torsion. The optimal timing for surgical intervention in gallbladder torsion is within two days of symptom onset; beyond this period, the mortality rate increases (18). Surgery is the definitive treatment (2, 10, 11), involving the detorsion of the gallbladder; if necrosis is present, cholecystectomy is required. For cases without evident necrosis, long-term follow-up data are needed to determine whether prophylactic cholecystectomy is warranted to prevent recurrence and complications.
Laparoscopic cholecystectomy has become the standard treatment in recent years due to its minimally invasive nature and rapid recovery. Reports indicate that laparoscopic procedures are both safe and effective in pediatric patients. Considering the risks of recurrence and mechanical stress injury, we do not advocate for the preservation of the gallbladder. In cases diagnosed with gallbladder torsion, we recommend cholecystectomy to prevent recurrence and to avert severe complications resulting from exacerbated cholangitis. We conducted a systematic search of English-language databases, including PubMed and Web of Science, to summarize pediatric gallbladder torsion cases, including our own, totaling 30 cases. Among these, 16 cases (including ours) were treated laparoscopically. Clinical data from these cases were also summarized, with detailed information provided in Tables 1, 2.
The three pediatric cases of gallbladder torsion complicated by acute appendicitis reported in this study share several notable clinical features. All patients presented with abdominal pain and vomiting, common symptoms of gastrointestinal distress. The first and third cases primarily involved right-sided abdominal pain, while the second case also featured nausea, vomiting, and worsened abdominal pain. Additionally, the second patient showed signs of lethargy and abdominal distension, likely due to progressing infection. None of the patients were initially diagnosed with gallbladder torsion, and the primary diagnosis in all cases was acute appendicitis. However, laparoscopic exploration revealed gallbladder torsion in each instance. The first patient did not undergo imaging prior to surgery, but intraoperative findings revealed a distended and twisted gallbladder, while the second case's preoperative CT scans suggested possible appendiceal perforation along with gallbladder distension. All patients underwent laparoscopic surgery, including appendectomy and cholecystectomy, with no significant postoperative complications, although one patient developed respiratory symptoms, which were successfully treated. These cases underscore the importance of considering gallbladder torsion in the differential diagnosis when managing pediatric patients with acute right-sided abdominal pain, particularly when conventional diagnoses like appendicitis do not fully explain the clinical presentation. Routine exploration of the gallbladder should be included in the surgical management of suspected appendicitis to avoid missed diagnoses and improve patient outcomes.
Conclusion
This report describes a successful laparoscopic appendectomy and cholecystectomy in a 2-year-old boy with acute suppurative appendicitis and gallbladder torsion. Routine inspection of the gallbladder should be considered in cases of pediatric acute appendicitis. Although the clinical presentation of gallbladder torsion is non-specific, clinicians and radiologists should enhance their ability to recognize pediatric patients with right-sided abdominal pain to avoid misdiagnosis, especially when traditional diagnoses (such as appendicitis) do not fully explain the clinical manifestations.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Levard G Weil D Barret D Barbier J. Torsion of the gallbladder in children. J Pediatr Surg. (1994) 29(4):569–70. 10.1016/0022-3468(94)90095-78014819 · doi ↗ · pubmed ↗
- 2Kimura T Yonekura T Yamauchi K Kosumi T Sasaki T Kamiyama M. Laparoscopic treatment of gallbladder volvulus: a pediatric case report and literature review. J Laparoendosc Adv Surg Tech A. (2008) 18(2):330–4. 10.1089/lap.2007.005718373471 · doi ↗ · pubmed ↗
- 3Mohamed Ali H Wahab ERA Damaj A Moussawi B Audi W Haidar M Intraoperative diagnosis of gallbladder volvulus. Case Rep Surg. (2023) 2023:1194077. 10.1155/2023/119407737941826 PMC 10630001 · doi ↗ · pubmed ↗
- 4Sun Y Fang Z Cao X Zhang T Liu X Zhang J Pediatric gallbladder torsion managed by laparoscopic cholecystectomy: a case report and scoping review. Front Pediatr. (2024) 12:1506506. 10.3389/fped.2024.150650639877339 PMC 11772262 · doi ↗ · pubmed ↗
- 5Ren H Liu H Liu X Wei H Tian P. Case report: rare floating gallbladder torsion in a child. Front Med (Lausanne). (2024) 11:1407716. 10.3389/fmed.2024.140771638873202 PMC 11169684 · doi ↗ · pubmed ↗
- 6Hamada T Tajima Y Yamaguchi J Ueda T Izawa K Ohtani H Torsion of the gallbladder in a 3-year-old infant. J Hepatobiliary Pancreat Surg. (2009) 16(2):234–7. 10.1007/s 00534-008-0027-919165413 · doi ↗ · pubmed ↗
- 7Hoshi R Uehara S Hosokawa T Kaneda H Koshinaga T. Gallbladder volvulus in two children: the importance of radiological features. Pediatr Int. (2022) 64(1):e 15260. 10.1111/ped.1526035938602 · doi ↗ · pubmed ↗
- 8Inoue S Odaka A Hashimoto D Tamura M Osada H: Gallbladder volvulus in a child with mild clinical presentation. Pediatr Radiol. (2011) 41(1):113–6. 10.1007/s 00247-010-1753-020593170 · doi ↗ · pubmed ↗