Electronic preoperative fasting abbreviation protocol: creation, application, and training of the patient care team
Rodrigo Costa Gonçalves, José Eduardo de Aguilar Nascimento, Marilia Arantes Rezio, Eula Cristina Machado Ferraz, Rachel de Carvalho

TL;DR
This study shows that using an electronic protocol and training healthcare teams can significantly reduce preoperative fasting times in hospitals.
Contribution
A novel electronic preoperative fasting protocol integrated with electronic medical records and combined with team training effectively reduces fasting duration.
Findings
Preoperative fasting time was reduced from 11.50 to 8.17 hours in one hospital (p:0.000).
Fasting time also decreased from 8.77 to 8.07 hours in the second hospital (p:0.025).
Electronic protocol management and team training were key to achieving these reductions.
Abstract
The preoperative fasting time does not, in practice, meet current recommendations for preoperative care. The implementation of clinical protocols for shortening preoperative fasting has faced numerous barriers. The present study aims to evaluate whether the creation, application and professional training to use a fasting abbreviation protocol, linked to the electronic medical record, is capable of managing and reducing preoperative fasting time. The study was conducted in two public hospitals in Goiânia, Goiás, Brazil. The DMAIC project methodology (Problem Definition - Measurement - Analysis - Implementation and Control) was used. Initially, the preoperative fasting time was measured in both institutions and the possible root causes for its prolongation were analyzed. Based on this assessment, a fasting abbreviation protocol was developed, managed through the electronic medical…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
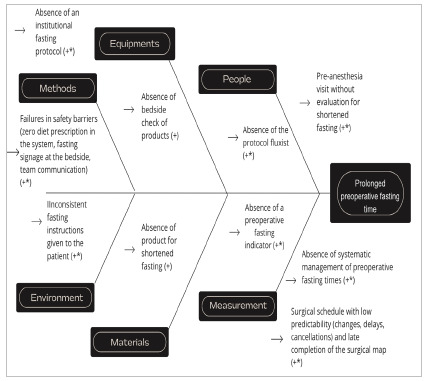 Figure 1
Figure 1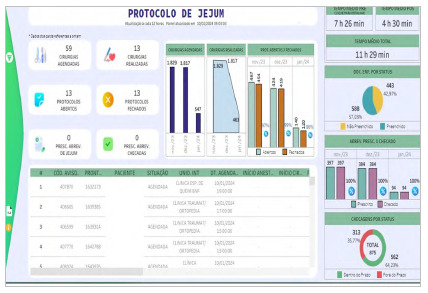 Figure 2
Figure 2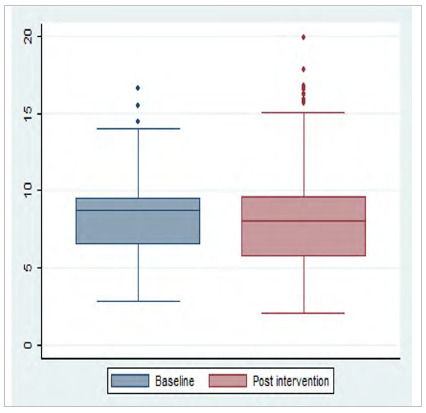 Figure 3
Figure 3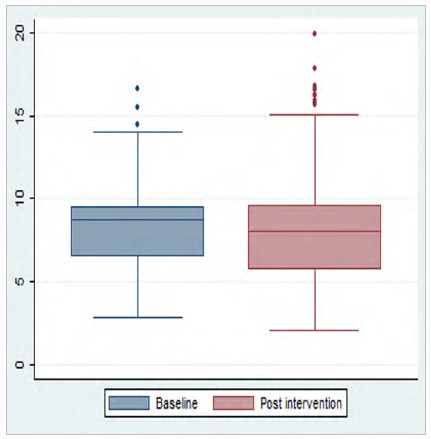 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsEnhanced Recovery After Surgery · Cardiac, Anesthesia and Surgical Outcomes · Nutrition and Health in Aging
INTRODUCTION
Among the preoperative care, preoperative fasting aims to reduce the risk of regurgitation and bronchial aspiration in the anesthetic-surgical procedure1 ^-^ 2. Currently, shorter fasting times have been shown to be safe and improve clinical outcomes, feelings of thirst, hunger, and well-being in patients3 ^-^ 6. However, the reality preoperative fasting time around the world does not meet current recommendations7 ^-^ 9. A study conducted in 16 Brazilian hospitals indicated a median fasting time of 12 hours, which was even longer in hospitals using traditional fasting protocols10.
The implementation of protocols aims to establish the best evidence-based routines in practice. Nonetheless, protocols for abbreviating operative fasting have been difficult to achieve in hospital services due to numerous barriers, including complex and unmanaged processes, decision-making based on hierarchy rather than protocol, absence of a multiprofessional work team, fragile communication channels, and problems in corporate education11 ^-^ 13.
We did not identify studies of implementation of this protocol using project methodology, electronic management, and professional training planning. In view of this, the present study aimed to verify whether the creation, application, and multiprofessional training for the use of a preoperative fasting abbreviation protocol, linked to the electronic medical record, would be able to manage and reduce the preoperative fasting time.
METHODS
This is a study with a mixed design, with the initial stage of the observational/descriptive type and the implementation stage of the interventional protocol.
The methodology used to develop the protocol of this study was based on the DMAIC strategy (Problem Definition - Measurement - Analysis - Implementation and Control), of the Lean Six Sigma project methodology14.
We conducted the study in two public hospitals in the city of Goiânia, capital of the State of Goiás, Brazil.
The target population consisted of patients undergoing elective surgeries in both hospitals, whose sample size was defined by the pre- and post-intervention data collection period.
Study design
To develop the protocol, we set up a multidisciplinary team to evaluate the fasting process, called the “Fasting Team”, involving members from the services of nutrition, nursing, surgery, anesthesiology, internal regulation, and information technology.
Phase 1. Identification of surgical patients’ fasting times and determining factors
For six months, weekly meetings were scheduled with the “Fasting Team”, lasting one to two hours, to develop the project methodology and align the tasks, divided into five stages:
Step 1- Problem Definition
We presented the problem to the “Fasting Team”: difficulty in the abbreviation of preoperative fasting in institutions. We made a dialogical presentation of the existing literature review on the subject. We presented the data collection spreadsheet and conducted training on the attributions and format of data collection by the care teams involved in the surgical patient flow.
Step 2 - Measurement
We collected information on the fasting time of elective surgeries over a period of 30 days in a unit of the general surgical clinic of each of the participating institutions. We did evaluate the type of anesthesia used. The data collection spreadsheet was printed at the nursing station of the studied ward of each hospital. The orderlies responsible for the wards recorded the times referring to the last meal delivered to the patient before surgery, the ingestion of the shortening fasting solution (12.5% maltodextrin), when used, and the meal delivered after surgery. The nursing care team collected the other data from the spreadsheet, including the procedure starting time. In both services, fasting was initiated at the hospital and hospitalizations were performed at least on the day before surgery. The data on fast duration were presented in a meeting with the “Fasting Team”.
Step 3 - Observational analysis
Through conversation circles with the “Fasting Team”, we mapped the flow of patients hospitalized with planned surgery, identifying the potential causes for the increase in fasting times at each stage of the flow, with the Brainstorm tool15. In each meeting, we exposed the stages of the flow and its barriers in the form of sticky notes (post-its) on a wall of the meeting room for better visualization by the team. In sequence, we grouped the causes using the Ishikawa’s Cause-Effect Diagram16. This diagram, also known as “fishbone”, has the purpose of organizing reasoning and hierarchically structuring the potential causes of a given problem or opportunity for improvement. It categorizes these root causes into six distinct groups of failures: method, material, workmanship, machinery, measurement, and environment. After this diagnostic stage, the project’s action plan was defined using the 5W2H methodology17. The 5W2H tool is a set of questions used to compose action plans quickly and efficiently. It consists of seven questions: What, Why, Where, Who, When, How, and How Much.
Phase 2. Development of the fasting abbreviation protocol
Step 4 - Implementation
The protocol was computerized in the institutions’ electronic medical record system (MV Soul) with the development of a protocol tab to manage the stages of the fasting protocol. We considered the information obtained in the analysis phase and identified as barriers to implementation, recording of times of meals received before and after surgery, prescription and bedside checking of shortening fasting solutions, and checklists of relevant information to ensure security in the protocol, in addition to the protocol closing document. The system captures the anesthetic induction start time for automated calculation of fasting times.
After this stage, we presented the training project for the care teams involved in the use of the computerized protocol. These teams were trained on how to fill out the protocol tabs and the new tasks to be performed, including those related to the education of patients and family members on preoperative fasting.
The planning of these training sessions involved the “Fasting Team”, through the evaluation of the barriers and facilitators identified in Phase 3. To that effect, we considered the importance of creating multiple training approaches, targeting different professional categories involved in the process, and the objective of transforming learning into performance enhancement, with improved fasting indicators and information to patients and communication among professionals18 ^,^ 19.
Step 5- Monitoring
In the monitoring phase, we collected automated data, provided via software for a new analysis of the preoperative fasting time. We developed indicators to monitor the various stages of the fasting protocol in the two institutions and to generate improvement cycles.
Statistical analysis
The dependent variable of the study was the preoperative fasting time, defined as the time elapsed between the last meal and the time of surgery, for patients without the use of a fasting abbreviation solution. For those using the solution, preoperative fasting time was defined as the time elapsed between the time of solution administration and the time of surgery.
We categorized the data into pre- and post-implementation of the computerized protocol in the two hospitals where the research took place. The pre-intervention quantitative data, collected during 30 days prior to the implementation of the protocol, were structured in double entry in the EpiData 3.1 software, with subsequent validation and export for analysis. We excluded from the statistical analysis data from patients whose times of surgery, times of the last meal, or times of fasting abbreviator ingestion were not recorded. We collected post-intervention data for two months, directly from the fasting time reports issued by the hospitals’ electronic medical records and imported them into the statistical analysis software.
We performed a descriptive analysis of the data, with calculation of the median, interquartile range, and variation of the preoperative fasting time, recorded in hours. Boxplot plots were constructed to evaluate data variability and dispersion. We assessed data distribution by the Kolmogorov-Smirnov test. We evaluated the difference between two medians (pre versus post implementation of the computerized protocol) by the Mann-Whitney test. Statistical analyses were performed using the Stata statistical package, version 12.0, considering statistical significance when p-value < 0.05.
Ethical aspects
The research was approved by the Ethics in Research Committee of the Hospital Israelita Albert Einstein, according to resolution 466/2012 of the National Health Council, under opinion 5.836.799 (CAAE 65135722.5.0000.0071), together with the respective Committees of the co-participating institutions, under opinion 5.874.572 (CAAE 65135722.5.3002.0237).
RESULTS
The median preoperative fasting time before the implementation of the protocol was 11.5 h (4.35 - 20.00) in hospital 1 and 8.77 h (2.83 - 16.65) in hospital 2.
The determining factors for prolonged fasting times were similar in both health units (Figure 1). However, hospital 2 already used a 12.5% maltodextrin solution for shortening fasting in an unmanaged form, which contributed to the shorter pre-intervention fasting time at that center. Action plans were drawn up to correct the determining factors.
Figure 1
Determining factors for prolonging the preoperative fasting time. Hospital 1 factors (+) and hospital 2 factors (*).
We developed a tab in the electronic medical record for managing patient information in the fasting abbreviation protocol, as well as a panel for online monitoring of data and indicators and automated collection of the duration of the preoperative fasting time after the intervention (Figure 2). The panel uses the Tableau Business Intelligence (BI) tool, accessing the database of the Hospital Management System “MV Sistemas” that operates with an Oracle database.
Figure 2
Panel for automated data collection and online management in the post-intervention period.
The protocol in both centers began with the evaluation of the surgical maps the night before the procedures, by a nutritionist of the protocol team. Each health institution was responsible for defining the time of the last solid meal and the ingestion of the shortening fasting solution, according to its surgical schedule, planning of the patients’ hospitalization time, and the delivery of meals. Therefore, not all surgical schedules were eligible for the shortening fasting solution. Patients with delayed gastric or esophageal emptying signaling at the preanesthetic visit were also not eligible for the use of this solution.
Based on these definitions of the protocol, the nutritionist was responsible for prescribing the patient’s last solid meal and the shortening fasting solution in the electronic medical record, when indicated. The 12.5% maltodextrin solution was supervised by a nursing technician and its time was recorded by an electronic bedside checking system, scanning the barcodes of the patient’s wristband and the fasting abbreviation solution. The time of the last solid meal was recorded in a document with a structured field in the electronic medical record by the nutritionist. Patients included in the operative fasting protocol had prominent signs in the electronic medical record until the protocol was closed at the end of the fast. The nurses were responsible for signaling the fasting beds and emphasizing the time of surgery, the beginning of fasting, and the time of ingestion of the shortening fasting solution to patients and family members.
The care teams were trained in both units to use the managed and computerized protocol. Some training sessions involved exclusively medical, nursing, or call center staff, while others involved the entire multi-professional team. Patients and family members were also contemplated with the development of a surgical booklet with valuable information. Different teaching methodologies were used: publication of a fasting protocol in the internal communication system, printed reminders posted on computers and displays, reminders on computer screens, workshops, gamification, corporate asynchronous distance learning (Distance Learning) classes, conversation circles with small groups at the workstations, and audits with individual feedback (Table 1).
Table 1 Corporate teaching strategies and teams involved. TEACHING STRATEGIESHOSPITAL 1HOSPITAL 2Fasting protocol available on the intranet✔✔Printed reminders ✔#Digital reminders✔✔++Printed educational booklet ✔+Workshop/Seminars✔** E-learning✔# Small groups talks at workstations ✔✔Audits and individual feedbacks✔✔Games✔
✔: Strategy carried out * Multiprofessional team** Nursing team + Patients and family members ++ Call center # Medical team
Data analysis showed a reduction in the median preoperative fasting time at both institutions (Table 2).
Table 2 Preoperative fasting time before and after the intervention, in total hours and by data collection site.
PRE-INTERVENTION POST-INTERVENTION Health UnitMedian (IQR) (h)Amplitude (h)Median (IQR) (h)Amplitude (h)p-value*Hospital 111.5 (9.00-15.58)4.35-20.008.17 (6.27-9.42)2.22-20.920.000Hospital 28.77 (6.50-9.52)2.83-16.658.07 (5.72-9.65)2.05-19.920.025h: hours; IQR: interquartile range (Q1-Q3); *Mann-Whitney test.
There was a significant reduction in data variability in hospital 1, with 75% of the times below 9.42 h after the intervention (Figure 3).
Figure 3
Boxplot of the preoperative (n=68) and post-intervention (n=603) fasting time of patients in hospital 1; p: 0.000.
In hospital 2, despite the reduction in the median, 25% of the fasting times were longer than 9.65 h (Figure 4).
Figure 4
Boxplot of the preoperative (n=104) and post-intervention (n=1149) fasting time of patients in hospital 2; p: 0.025.
DISCUSSION
The implementation of the computerized protocol for abbreviation of preoperative fasting and professional training allowed for a reduction in the duration of preoperative fasting in both health units studied. The construction of a protocol in an interdisciplinary way, adapted to the needs of each institution, its management in electronic format, and the use of multiple training methodologies are innovative techniques for the implementation of a preoperative fasting protocol.
As expected, the preoperative fasting times before the implementation of the protocol were prolonged in relation to current scientific recommendations and similar to those found in Brazilian and international studies7 ^-^ 10. The multicenter study of the Brazilian Group for the Study of Preoperative Fasting Time (BIGFAST) evaluated preoperative fasting in 3,715 patients in 16 Brazilian hospitals. The median fasting time was 12 hours, and fasting was significantly longer in hospitals using traditional fasting protocols (13 hours) than in hospitals adopting new guidelines (8 hours)10. We also observed this fact in hospital 2, which had a shorter initial fasting time because it already used a 12.5% maltodextrin solution, as recommended by guidelines3 ^,^ 20.
In the present study, the mapping of the process by the “Fasting Team” was fundamental for the identification of the main barriers to the protocol. The creation of a multidisciplinary team, including surgeons and anesthesiologists, for the development and implementation of the project has already been suggested by other studies, in which a collaborative approach adapted to local realities was a predictor of success in surgical care programs11 ^-^ 13. The use of project methodology techniques allows the involvement of the care team in the creation and development of the new workflow, ensuring greater learning and effectiveness of the processes21.
In contrast to what other studies have found13 ^,^ 22, anesthesiologists were not resistant to the protocol. We did not identify fear of bronchial aspiration or legal risks as barriers to the with the prescription of shortened fasting. In Brazil, the Federal Council of Medicine and the Brazilian Society of Anesthesiology validate this recommendation for anesthetic acts. The concern of anesthesiologists was that the lack of coordination between teams would lead to surgical cancellations. This complexity of processes, involving low predictability of appointments and surgical times, was observed in another study11 and was one of the main challenges of this project. The predictability of the surgical schedule in the two health units remained in need of improvement at the end of the study. We observed fasting times of more than 12 hours in situations such as postponement of the procedure, changes in the order of the surgical schedule, and cancellations made after the completion of the surgical map and planning of the fast.
The registration of contraindications to the use of shortening fasting solution during pre-anesthetic visits in wards (hospital 1) or outpatient clinics (hospital 2) ensured better communication with the nutrition service and greater safety in the process. Another study had already pointed out the benefits of the pre-anesthetic visit to the greater knowledge of patients about fasting recommendations23.
The “Fasting Teams” developed and published in both units a document supporting the protocol. However, other studies11 ^,^ 24 have identified that the existence of a protocol is not enough to improve results, minimize hierarchical decisions, and empower decision-making. The support of the hospitals’ clinical boards was crucial for the protocols to be treated as institutional. Improved communication channels, adequate monitoring, and feedback processes contribute to sustainability11.
Automated protocols can also promote greater adherence to the process and contribute to data management, directing actions towards numerous improvements25 ^,^ 26. Computerized data collection in the post-intervention allowed the management of the preoperative fasting duration of a larger number of patients when compared with paper-based management. Thus, the development of a computerized fasting protocol linked to the electronic medical record and a panel for managing fasting times and other protocol indicators, with filters by hospital areas, was innovative. This management was fundamental for the development of action plans and the construction of the project’s training.
The education of employees, patients, and family members facilitates the implementation of programs to accelerate surgical recovery11 ^,^ 13. In this way, we built a broad training matrix, involving all the teams involved in the process, using diversified methodologies, as planned by the “Fasting Team”. The combination of learning strategies is more effective for the success of improvement implementation27, and continuing education should involve the different professional categories that are part of the process. The creation of teams to build and monitor this implementation, as well as the use of electronic support systems for clinical decision-making, are recommended18 ^,^ 28. A systematic review produced by Cochrane evaluated implementation tools focused on health professionals, patients, and health organizations. It was not possible to identify the individual impact of each tool. However, printed educational materials, educational meetings, educational blitz, local opinion leaders, auditing and feedback, computerized reminders, and personalized interventions present evidence28. In addition, the outcome indicators are the most advanced level of evaluation of the effectiveness of training and show the real educational impact on health outcomes29.
Study limitations
The methodology used allowed the identification of the existing barriers in both hospitals and individualized strategies to overcome them. However, other institutions can use the methodology, but build an implementation adapted to local needs.
Filling in data in the electronic medical record is the responsibility of the care teams and any failures cannot be eliminated.
The lack of an assertive surgical schedule did not allow the use of an abbreviating fasting solution at all surgical times, which could lead to better results.
It is not possible to separate the contribution of the project methodology from the computerization of the protocol and from the professional training in relation to the results of the present study.
The computerization of the protocol in MV Sistemas does not guarantee its implementation in other electronic medical records.
Perspectives
It is desirable that future studies evaluate work overload and employee turnover as limiting factors for implementation and training and ways to overcome them in this protocol. Research involving strategies to optimize the surgical schedule, such as monitoring surgical times by related diagnosis groups and by surgical team and their impact on the predictability of fasting are also warranted.
CONCLUSION
The elaboration and application of the protocol for abbreviation of preoperative fasting, contemplating the needs of each institution studied, its management in electronic format, and the use of multiple training methodologies for the multiprofessional team made it possible to reduce the preoperative fasting time in both health units.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1de Aguilar-Nascimento JE Dock-Nascimento DB Reducing preoperative fasting time: A trend based on evidence World J Gastrointest Surg 2010273576010.4240/wjgs.v 2.i 3.57.PMC 299921621160851 · doi ↗ · pubmed ↗
- 2Brady M Kinn S Stuart P Preoperative fasting for adults to prevent perioperative complications Cochrane Database Syst Rev 20034 CD 004423 CD 00442310.1002/14651858.CD 00442314584013 · doi ↗ · pubmed ↗
- 3Aguilar-Nascimento JE Ribeiro U Junior Portari-Filho PE Salomão AB Caporossi C Colleoni R Neto Perioperative care in digestive surgery: the ERAS and ACERTO protocols. Brazilian College of Digestive Surgery Position Paper ABCD Arq Bras Cir Dig 202437 e 179410.1590/0102-672020240001 e 1794.38716919 PMC 11072254 · doi ↗ · pubmed ↗
- 4Yip A Hogan S Carey S Interventions Aimed at Reducing Fasting Times in Acute Hospital Patients A Systematic Literature Review Nutr Clin Pract 202136113315210.1002/ncp.1057932970377 · doi ↗ · pubmed ↗
- 5Dock-Nascimento DB de Aguilar-Nascimento JE Magalhaes Faria MS Caporossi C Slhessarenko N Waitzberg DL Evaluation of the effects of a preoperative 2-hour fast with maltodextrine and glutamine on insulin resistance, acute-phase response, nitrogen balance, and serum glutathione after laparoscopic cholecystectomy a controlled randomized trial JPEN J Parenter Enteral Nutr 2012361435210.1177/014860711142271922235107 · doi ↗ · pubmed ↗
- 6Morrison CE Ritchie-Mc Lean S Jha A Mythen M Two hours too long time to review fasting guidelines for clear fluids Br J Anaesth 2020124436336610.1016/j.bja.2019.11.03631959387 · doi ↗ · pubmed ↗
- 7Lim HJ Lee H Ti LK An audit of preoperative fasting compliance at a major tertiary referral hospital in Singapore Singapore Med J 2014551182310.11622/smedj.201400524452973 PMC 4291906 · doi ↗ · pubmed ↗
- 8Njoroge G Kivuti-Bitok L Kimani S Preoperative Fasting among Adult Patients for Elective Surgery in a Kenyan Referral Hospital Int Sch Res Notices 201720172159606215960610.1155/2017/215960628487877 PMC 5405382 · doi ↗ · pubmed ↗