Pseudoaneurysmal rupture with massive bleeding following endoscopic ultrasound-guided gallbladder drainage using an electrocautery-enhanced lumen-apposing metal stent
Kyong Joo Lee, Se Woo Park, Dong Hee Koh

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
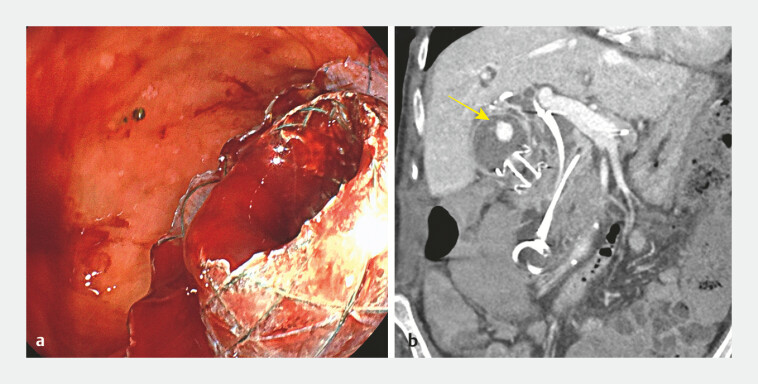 Fig. 1
Fig. 1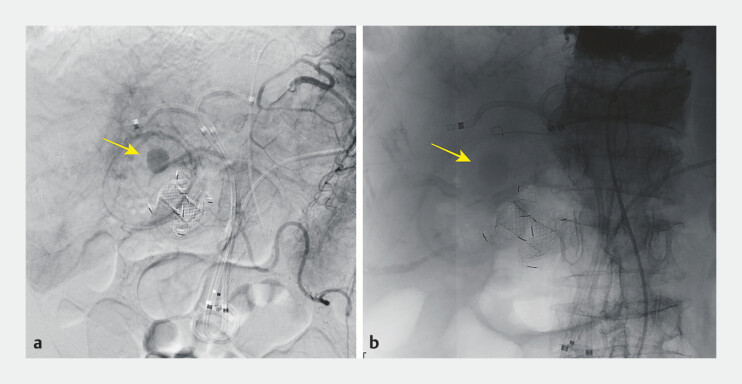 Fig. 2
Fig. 2- —Hallym University Medical Center Research Fund
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGallbladder and Bile Duct Disorders · Abdominal vascular conditions and treatments · Esophageal and GI Pathology
Endoscopic ultrasound-guided gallbladder drainage (EUS-GBD) is a minimally invasive and effective treatment for patients at high risk of acute cholecystitis who are unsuitable for surgical intervention due to underlying comorbidities 1 . Although EUS-GBD is generally considered safe, with reported bleeding events in 2.1–4.3% of cases 2 , the occurrence of pseudoaneurysms is rare 3 . We report a case of pseudoaneurysmal rupture following EUS-GBD using a novel electrocautery-enhanced lumen-apposing metal stent (LAMS).
A 74-year-old woman with multiple myeloma, chronic kidney disease, and recurrent dyspnea presented with abdominal pain and developed acute cholecystitis 3 days after undergoing endoscopic retrograde cholangiopancreatography (ERCP) for bile duct stones. She exhibited a positive Murphyʼs sign. Abdominal computed tomography (CT) revealed gallbladder dilation with pericholecystic fluid collection. Given her poor surgical candidacy, EUS-GBD was performed ( Video 1 ).
Inadvertent injury to the opposite gallbladder wall caused by puncture during endoscopic ultrasound-guided gallbladder drainage (EUS-GBD) in a 74-year-old woman. Bleeding occurred after the deployment of the electrocautery-enhanced lumen-apposing metal stent but resolved spontaneously.Video 1
Using a linear echoendoscope (EG-580UT; Fujifilm Medical Systems, Tokyo, Japan), the gallbladder neck was punctured with a 19-gauge needle (EZ Shot3; Olympus Medical, Japan); however, the opposite gallbladder wall was inadvertently punctured. Following guidewire placement and contrast administration, the electrocautery-enhanced-LAMS (Niti-S HOT SPAXUS; Taewoong Medical, Goyang, Korea) was successfully deployed, resulting in substantial bleeding into the duodenum. The hemorrhage resolved spontaneously, and the patient was discharged on post-procedural day 3.
After 6 days, the patient was readmitted with jaundice and fever. Urgent ERCP revealed blood clots draining from both the bile duct and through the LAMS. Continuous drainage of fresh blood from the LAMS ( Fig. 1 a ) prompted an immediate CT scan, which showed high-density material within the gallbladder consistent with blood, along with a pseudoaneurysm on the gallbladder wall ( Fig. 1 b ). Angiography confirmed involvement of the cystic artery ( Fig. 2 a ), and embolization was successfully performed using gelfoam particles ( Fig. 2 b ). The patient’s symptoms resolved without further complications.
Endoscopic and radiologic findings of pseudoaneurysm following endoscopic ultrasound-guided gallbladder drainage. a Endoscopic view showing continuous fresh blood draining through the lumen-apposing metal stent into the duodenum. b Computed tomography scan revealing high-density material in the gallbladder (yellow arrow), indicating the presence of a pseudoaneurysm.
Angiographic findings and embolization of the cystic artery. a Angiographic image showing the presence of a pseudoaneurysm involving the cystic artery (arrow). b Angiographic image after gelfoam particle embolization showing successful resolution of the pseudoaneurysm (arrow).
The pseudoaneurysm was likely caused by mechanical trauma during the initial needle puncture. To reduce the risk of such vascular injuries, careful puncture of the gallbladder wall adjacent to the duodenum is essential.
Endoscopy_UCTN_Code_CPL_1AL_2AD
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Sagami R Mizukami K Sato T Strategy comparison of endoscopic ultrasound-guided gallbladder drainage to percutaneous transhepatic gallbladder drainage, following failed emergent endoscopic transpapillary gallbladder drainage J Clin Med 202312703410.3390/jcm 1222703438002649 PMC 10671954 · doi ↗ · pubmed ↗
- 2Giri S Mohan BP Jearth V Adverse events with EUS-guided biliary drainage: a systematic review and meta-analysis Gastrointest Endosc 2023985155.23E 2037392952 10.1016/j.gie.2023.06.055 · doi ↗ · pubmed ↗
- 3Sagami R Hayasaka K Nishikiori H Current status in the treatment of acute cholecystitis patients receiving antithrombotic therapy: is endoscopic drainage feasible? a systematic review Clin Endosc 20205317618810.5946/ce.2019.17731914723 PMC 7137572 · doi ↗ · pubmed ↗