Comparative Analysis of Surgical and Conservative Approaches to Recurrent Thyroglossal Duct Cysts: A Literature Review
Barbara Klyslie Kato, Leticia Souza Rego, Pedro Bizarro dos Santos, Flavio Carneiro Hojaij

TL;DR
This review compares surgical and non-surgical treatments for recurring thyroglossal duct cysts, finding that conservative methods may offer benefits but surgery remains the standard due to proven effectiveness.
Contribution
The study provides a comparative analysis of treatment options for recurrent thyroglossal duct cysts, highlighting the potential and limitations of conservative approaches.
Findings
Nine studies involving 278 patients were analyzed, with 143 undergoing surgery and 135 receiving chemical ablation.
Conservative treatments showed potential benefits like lower recurrence rates and faster recovery, but surgery remains the preferred method due to its proven efficacy.
Ethanol and OK-432 were the primary agents used in chemical ablation for this condition.
Abstract
Introduction The management of recurrent thyroglossal duct cysts poses persistent challenges. The present review assesses chemical ablations and surgical re-interventions as strategies for recurrence. However, limited comparative studies exist to determine the optimal approach and follow-up outcome. Objectives The aim of the current study is to conduct a review gathering evidence from the literature to analyze and synthesize the safest and most effective approaches for treating recurrent thyroglossal duct cysts. Methods The present study aims to comprehensively search electronic databases, including the Latin American and Caribbean Literature in Health Sciences (Literatura Latino-Americana e do Caribe em Ciências da Saúde, LILACS, in Portuguese), the database of the Journal of the American Medical Association (JAMA), SciVerse Scopus, Virtual Health Library (Biblioteca Virtual em…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
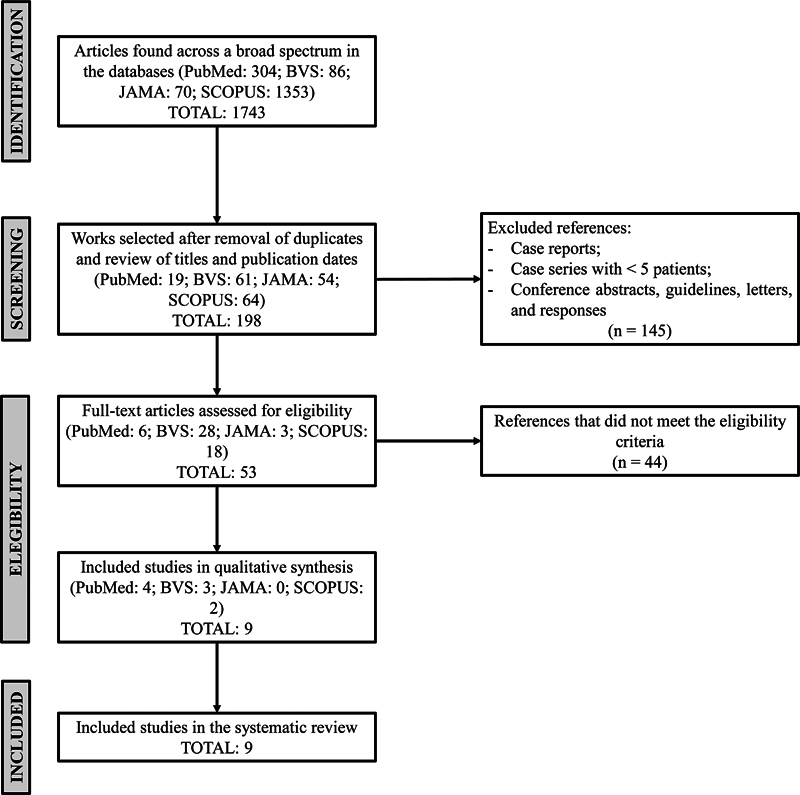 Fig. 1
Fig. 1| Author | Publication | Study design | Country | Number of patients with recurrent thyroglossal duct cyst |
|---|---|---|---|---|
|
Pastore and Bartoli
| 2014 | Retrospective review | Italy | 7 |
|
O'Neil and Cheng
| 2018 | Retrospective review | Australia | 16 |
|
O'Neil et al.
| 2016 | Retrospective review | Australia | 7 |
|
Perkins et al.
| 2005 | Retrospective review | United States | 34 |
|
Ibrahim et al.
| 2015 | Systematic review | Canada | 66 patients (114 procedures) |
|
Isaacson et al.
| 2019 | Systematic review | United States | 13 |
|
Park et al.
| 2021 | Systematic review and meta-analysis | South Korea | ETHANOL: 82 |
|
Ohta et al.
| 2021 | Case series | Japan | 5 |
|
Simon and Magit
| 2012 | Retrospective case review | United States | 13 |
| Treatment approach | Number of patients treated | Recurrence rate |
|---|---|---|
| Surgical excision | 143 | 56 (39.16%) |
| OK-432 esclerotherapy | 53 | 24 (45.28%) |
| Ethanol esclerotherapy | 82 | 13 (15.85%) |
| Total esclerotherapy | 129 | 37 (27.61%)  |
| Author | Mean age (years) | Number and type of procedure for recurrence | Recurrences |
|---|---|---|---|
|
Pastore and Bartoli
| Undisclosed | Extended Sistrunk | 0 |
| O'Neil LM, Cheng AT | 5.3 ± 3.1 | Sistrunk | 4 |
| O'Neil LM, Gunaratne DA, Cheng AT, Riffat F | 26.4 ± 10.9 | Extensive neck dissection | 0 |
|
Perkins et al.
| 1 ± 21 | - Extensive neck dissection | 22 |
|
Ibrahim et al.
| 2 ± 18 | - En block | - En block: 03 |
|
Isaacson et al.
| 3 ± 19 | Neck dissection | 2 |
| Author | Mean age | Number and type of procedure for recurrence | Recurrences |
|---|---|---|---|
|
Park et al.
| 14 ± 75 | Ethanol: 82; OK-432: 42 | Ethanol: 13; OK-432: 24 |
|
Ohta et al.
| 4 ± 7 | OK-432: 5 | 0 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHead and Neck Anomalies · Salivary Gland Tumors Diagnosis and Treatment · Teratomas and Epidermoid Cysts
Introduction
Thyroglossal cyst is the most common congenital condition among benign cervical masses, occurring in 70 to 75% of cases in the midline of the neck in children under 5 years. 1 2 3 4 5 The formation of the thyroid gland originates from a protrusion in the primitive pharynx, which is the site of the future foramen cecum of the tongue. This phenomenon occurs from the fourth week of gestation. As the embryo elongates, a pathway is formed as the thyroid gland establishes itself in the neck. This structure is known as the thyroglossal tract, occupying the midline of the neck and later the base of the neck by the seventh week. The tract is absorbed by the tenth week of gestation, but the remaining parts can give rise to thyroglossal cysts. 6
Surgical intervention using the Sistrunk technique is the treatment of choice for cysts, with only a 3% relapse rate. 7 8 9 The relapse of the cyst occurs when the thyroglossal duct tract is not completely removed or in cases of lobulated cysts and multiple foci. 10 11 12 13 14 Although the Sistrunk technique has a low recurrence rate, relapses can be challenging due to the potential significant disruptions for both physicians and patients.
The present review aims to present possible therapies based on the evidence found in a structured review of the medical literature.
Methods
The present study was based on a systematic review of the international and national scientific literature, aiming to analyze the best practices and methods for the treatment of recurrent thyroglossal cysts using the databases Latin American and Caribbean Literature in Health Sciences (Literatura Latino-Americana e do Caribe em Ciências da Saúde – LILACS, in Portuguese), Journal of American Medical Association (JAMA), SciVerse Scopus, the Virtual Health Library (Biblioteca Virtual em Saúde, BVS, in Portuguese; http://www.bireme.br ), as well as the United States National Library of Medicine – PubMed ( http://www.ncbi.nlm.nih.gov/pubmed ).
The review was conducted following the guidelines of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement of 2020, 15 as illustrated in the attached diagram ( Fig. 1 ).
Adapted schematic representation of the PRISMA flow diagram for the methods of identification, screening, eligibility, and inclusion of studies in the systematic review. Abbreviation: PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Data Source and Search Strategy
The PubMed, BVS, JAMA, and Scopus databases were used as the literary basis for the review. A total of 1,743 studies were found in the aforementioned databases using the descriptors recurrent , thyroglossal , and duct cyst . The search was conducted from December 15, 2022, to January 15, 2023.
Study Selection
Inclusion Criteria
The following criteria were used to select the articles: 1) patients with recurrent thyroglossal duct cyst; 2) publications between 2000 and 2022; 3) clinical and/or surgical intervention for the recurrent cyst; and 4) safety and efficacy of the analyzed approach.
Exclusion Criteria
The exclusion criteria were as follows: 1) case reports or case series with fewer than five patients; 2) articles suspected of containing duplicate data; 3) studies that did not report the success rate of the described treatment modality; and 4) conference abstracts, guidelines, letters, and responses.
The study selection process was independently performed by two authors (reviewer 1 and reviewer 2) through a comprehensive search of the databases. The literature search initially yielded a total of 1,743 articles. Then, articles with eligible titles, abstracts, and publication period were selected, resulting in 198 articles. After independent review, 145 studies were excluded for not meeting the eligibility criteria. The full texts of the remaining 53 articles were reviewed, and 9 studies met the criteria for inclusion in this systematic review. 16 17 18 19 20 21 22 23
Data Extraction
The selected studies were grouped into a spreadsheet for further analysis. For each included study, the total number of patients with recurrent thyroglossal duct cyst, the mean age of the patients, the number and type of procedures adopted to manage the recurrence, treatment outcomes, and the average follow-up period were extracted. This information was obtained from the main text as well as relevant figures ( Table 1 ).
Results
Among the 9 selected studies, 2 20 24 present non-surgical clinical approaches, focusing on chemical ablation (ethanol and OK-432), and 1 23 compares preoperative practices of incision and drainage versus isolated antibiotic therapy for infected thyroglossal cysts and their association with cyst recurrence after the Sistrunk procedure. The remaining six articles 16 17 18 19 21 22 analyze surgical approaches for recurrent cysts: two studies 16 18 demonstrate the Sistrunk technique and its extended variation; two studies 17 19 discuss the extent of neck dissection; and the remaining two studies 21 22 discuss different surgical techniques for cyst resolution.
Overall, 277 patients underwent treatment for recurrent thyroglossal cyst, with 143 undergoing surgical removal and 134 undergoing sclerotherapy ( Tables 2 3 4 ).
Among the surgical cases, 56 (39.16%) experienced subsequent recurrences within at least 12 months of follow-up. The studies by Ibrahim (2015), Isaacson (2019), Pastore et al. (2014), and O’Neill et al. (2018) reported the efficacy of the Sistrunk technique as 64%, 84%, 100%, and 75%, respectively. Other surgical techniques were addressed by Perkins (2006), O'Neill (2016), and Ibrahim (2015), with cure rates ranging from 80 to 100%, and a small number of patients ( Table 1 ).
According to Simon and Magit (2012), a previous history of preoperative infection resulted in a significantly higher recurrence rate ( p = 0.007), as determined by the Fisher exact test. An analysis of 120 patients who underwent the surgical procedure revealed that 49% of them had a history of previous infection. The relative risk of recurrence in patients with a history of preoperative infection was 4.83 (95% confidence interval [CI], 1.40–16.65), while the odds ratio was 5.81 (95% CI, 1.51–22.30). The study reports that 12% of patients underwent drainage and incision, and this group had a cyst recurrence rate of 10.8%.
The studies analyzed investigated chemical ablation using Ethanol or OK-432 20 24 as an alternative to Sistrunk surgery for the treatment of thyroglossal cysts. According to the meta-analysis proposed by Park et al. (2021), 7 articles with a total of 129 patients were included, ranging in age from 14 to 75 years. The success rate of ethanol use was 84%, while for OK-432 it was 51%. However, the statistical significance difference between these success rates is ambiguous ( p = 0.055).
The primary treatment resulted in complete resolution of the cysts, and secondary outcomes included rates of complications and recurrence, such as pain and inspiratory stridor, both of which were subsequently resolved. The selected articles followed up with patients for a period ranging from 1 to 94 months, identifying 13 recurrences in the ethanol group and 24 in the OK-432 group.
The case series conducted by Ohta et al. (2021) proposed the application of OK-432 and a follow-up period of 14.2 months after the last application. As a result, 4 out of 5 patients (80%) showed complete resolution or significant shrinkage of the cyst with just one cycle of therapy, without recurrences or major complications. The only reported complication was moderate fever (37.5–38.5°C). Thus, out of the 134 patients who underwent conservative treatment, 53 received OK-432 ablation and 82 received ethanol ablation ( Table 2 ). Ohta et al. 20 and Park et al. 24 observed a recurrence rate of 24 (45.28%) out of the 53 patients treated with OK-432, while ethanol ablation resulted in 13 recurrences (15.85%).
Discussion
The recurrence of cysts in the thyroglossal duct poses a persistent and challenging issue in its treatment. The primary cause of recurrence is often attributed to incomplete removal during the initial surgery, which is closely associated with three factors: patient age, cyst histopathology, and infection. 7 8 9 14 25 Additionally, the presence of multiple diverticula connected to the duct, along with branching and proliferation within the surrounding tissue, particularly around the hyoid bone, as well as the presence of residual duct remnants, can contribute significantly to the recurrence phenomenon. Although surgical intervention is commonly employed as the first-line approach for thyroglossal duct cysts, the need to explore and enhance conservative therapeutic options becomes crucial when recurrence occurs. 26 These conservative approaches have shown promise in minimizing the risk of further recurrences, but their efficacy requires validation through additional rigorous and comprehensive studies.
The Sistrunk technique remains the gold standard of treatment, 3 as the recurrence rate does not exceed 10% when compared with simple cyst excision, which has a recurrence rate between 45 and 55%. O'Neill et al. 18 (2018) conducted a review discussing the efficacy of the Sistrunk technique in recurrent cysts. The sample consisted of 16 patients over a 15-year period in a single hospital. Eleven of the patients had undergone primary Sistrunk surgery, two were conservatively treated during recurrence, and the remaining nine underwent Sistrunk procedure again. Seven (78%) of these patients who experienced recurrence after the Sistrunk technique had no further recurrences during a mean follow-up of 21.8 ± 29.2 months, while 2 patients (22%) remained unhealed even after 2 subsequent excisions. This demonstrates the challenge of the problem at hand.
In a systematic review conducted by Ibrahim et al. 21 (2015), various surgical techniques for treating thyroglossal duct cysts were analyzed, encompassing 9 studies with a collective patient pool of over 66 individuals and a total of 114 secondary surgeries. Among the examined techniques, transhyoid pharyngotomy and the Koempel technique yielded successful outcomes, demonstrating no complications or instances of recurrence. However, it is important to acknowledge the limited number of patients in the Koempel groups, which may impact the generalizability of the results. These findings align with other studies that also emphasize the efficacy of these surgical approaches in managing thyroglossal duct cysts.
Due to the scarcity of scientific literature addressing non-invasive techniques, this review was limited to only two studies that met the inclusion criteria. These studies investigated the use of ethanol or OK-432 sclerotherapy for the treatment of thyroglossal duct cysts. A total of 134 patients underwent chemical ablation and, of these, 36 (27%) experienced cyst recurrence. Compared with surgery, chemical ablation is a minimally invasive method that leaves no scars or pigmentation at the injection site, does not require special equipment or hospitalization, has a short procedure duration, is minimally painful, and reduces the risks of complications such as secondary infections and hemorrhage. 27 28
The mechanism responsible for the efficacy of OK-432 therapy involves the intense production of cytokines, including interleukin 6 (IL-6), interleukin 8 (IL-8), interferon-gamma (IFN-γ), interferon-alpha (IFN-α), vascular endothelial growth factor (VEGF), and periostin, through the activation of monocytes and neutrophils. 29 This mechanism leads to a reduction in cyst volume and the generation of fibrotic adhesion within the cystic cavity. On the other hand, ethanol chemical ablation induces cell membrane lysis, protein denaturation, and vascular occlusion, resulting in cell death. The success of sclerotherapy for the treatment of recurrent thyroglossal duct cysts was determined based on the reduction of cyst volume by 50 to 70% or complete absence of the cyst after the procedure, with no recurrence. The combined success rates were 84% in the ethanol group.
Conclusion
This review highlights conservative treatments for recurrent thyroglossal duct cysts, although further clarification is still needed. This approach demonstrates potential benefits, such as effectiveness in terms of invasiveness and recovery time. However, surgery remains the preferred therapeutic option as it is already widely known, safe, and established. As the benefits of conservative treatment are further refined and supported by additional studies, a shift in the therapeutic approach for thyroglossal duct cysts can be expected.
Limitations
The literature review's limitation in this study arises from the small number of eligible studies available on the topic, which restricts the breadth and depth of analysis. The limited availability of relevant studies may have led to a narrower perspective on the research question, potentially overlooking important findings or variations in the data. This constraint highlights the need for more comprehensive research in the area to provide a more robust evidence base. Future studies with a broader scope and a larger sample of eligible studies could enhance the reliability and generalizability of the findings.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Chou J Walters A Hage R Thyroglossal duct cysts: anatomy, embryology and treatment Surg Radiol Anat 2013351087588123689821 10.1007/s 00276-013-1115-3 · doi ↗ · pubmed ↗
- 2Randolph G W Kamani D V Thyroglossal duct cyst, thyroglossal duct cyst cancer, and ectopic thyroid Up To Date,2023[updated Jan 17, 2023]. Available from:https://www.uptodate.com/contents/thyroglossal-duct-cyst-thyroglossal-duct-cyst-cancer-and-ectopic-thyroid?search
- 3Brousseau V J Solares C A Xu M Krakovitz P Koltai P J Thyroglossal duct cysts: presentation and management in children versus adults Int J Pediatr Otorhinolaryngol 200367121285129014643470 10.1016/j.ijporl.2003.07.006 · doi ↗ · pubmed ↗
- 4Bhama A R Smith R J Robinson R A Preoperative evaluation of thyroglossal duct cysts: children versus adults–is there a difference?Am J Surg 20142070690290624246260 10.1016/j.amjsurg.2013.06.018 · doi ↗ · pubmed ↗
- 5Ahuja A T Wong K T King A D Yuen E H Imaging for thyroglossal duct cyst: the bare essentials Clin Radiol 2005600214114815664568 10.1016/j.crad.2004.08.009 · doi ↗ · pubmed ↗
- 6Amos J Shermetaro C Thyroglossal Duct Cyst Treasure Island (FL)Stat Pearls Publishing 2023 Jan-. Available from:https://www.ncbi.nlm.nih.gov/books/NBK 519057/30085599 · pubmed ↗
- 7Babu S Roman-Nielsen M Lechner M The Sistrunk procedure for thyroglossal duct cysts: a systematic review and meta-analysis Eur Arch Otorhinolaryngol 20212780111032506145
- 8Ren W Zhi K Zhao L Gao L Presentations and management of thyroglossal duct cyst in children versus adults: a review of 106 cases Oral Surg Oral Med Oral Pathol Oral Radiol Endod 201111102 e 1e 610.1016/j.tripleo.2010.10.02921237423 · doi ↗ · pubmed ↗