Effect of chewing gum combined with WeChat-enhanced instruction on bowel preparation in constipated patients: a randomized–controlled trial
Cong Gao, Deli Zou, Weiyi Wang, Yingchao Li, Jie Han, Dongshuai Su, Xingshun Qi

TL;DR
This study tested if chewing gum and WeChat instructions improve bowel prep for colonoscopies in constipated patients but found no improvement and more nausea.
Contribution
A novel combination of chewing gum and WeChat-based instructions was evaluated for improving bowel preparation in constipated patients.
Findings
Chewing gum with WeChat instructions did not improve bowel preparation quality compared to standard care.
The intervention group experienced significantly more nausea than the control group.
No differences were observed in polyp detection rates or procedure times between the groups.
Abstract
Constipated patients have higher risk of poor bowel preparation and suffer from dysfunction of the intestinal motor. Chewing gum can stimulate gut motility and enhanced instructions can improve the quality of bowel preparation. The objective of this study was to investigate whether chewing gum combined with WeChat-enhanced instruction can increase the quality of bowel preparation in constipated patients. This was a single-center, endoscopist-blinded, randomized–controlled trial. Patients were assigned (1:1) to the chewing gum and WeChat-enhanced instruction (CGW) group and the control group. Patients in both groups received 3 L of polyethylene glycol (PEG) before colonoscopy. Patients in the CGW group were asked to chew one piece of gum for 20 min after drinking each 1 L of PEG and received enhanced instruction via WeChat the day before colonoscopy. The quality of the bowel preparation…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
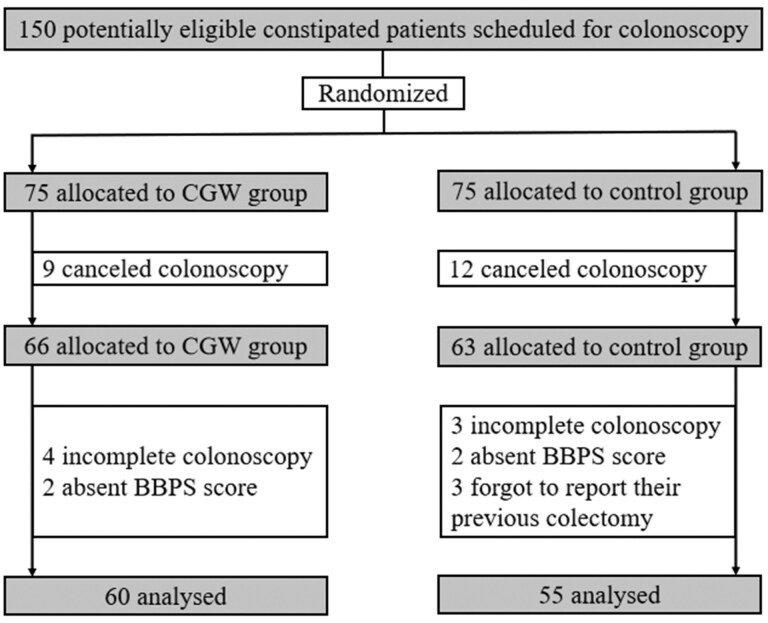 Figure 1
Figure 1| Variables | CGW ( | Control ( |
|
|---|---|---|---|
| Age, years, mean ± SD | 53.28 ± 15.39 | 51.51 ± 16.67 | 0.554 |
| Male | 15 (25.0) | 18 (32.7) | 0.360 |
| BMI, kg/m², mean ± SD | 22.87 ± 3.40 | 22.63 ± 3.45 | 0.715 |
| Colonoscopy time | 0.140 | ||
| Morning | 42 (70.0) | 45 (81.8) | |
| Afternoon | 18 (30.0) | 10 (18.2) | |
| Prior colonoscopy | 21 (35.0) | 21 (38.2) | 0.723 |
| Sedated colonoscopy | 7 (11.7) | 2 (3.6) | 0.166 |
| Prior abdominal surgery | 19 (31.7) | 18 (32.7) | 0.903 |
| Variables | CGW ( | Control ( |
|
|---|---|---|---|
| Primary outcomes | |||
| Adequate bowel preparation, | |||
| Total | 46 (76.7) | 39 (70.9) | 0.312 |
| Right colonic region | 46 (76.7) | 39 (70.9) | 0.312 |
| Transverse colonic region | 58 (96.7) | 49 (89.1) | 0.109 |
| Left colonic region | 58 (96.7) | 48 (87.3) | 0.062 |
| BBPS score, mean ± SD | |||
| Total | 6.80 ± 1.42 | 6.40 ± 1.78 | 0.184 |
| Right colonic region | 1.97 ± 0.66 | 1.75 ± 0.58 | 0.061 |
| Transverse colonic region | 2.42 ± 0.56 | 2.27 ± 0.71 | 0.227 |
| Left colonic region | 2.40 ± 0.56 | 2.35 ± 0.75 | 0.662 |
| Secondary outcomes | |||
| ADR/PDR, | 33 (55.0) | 29 (52.7) | 0.807 |
| Number of polyps and/or adenomas, mean ± SD | 1.3 ± 1.9 | 1.2 ± 1.6 | 0.356 |
| Insertion time, min, mean ± SD | 8.32 ± 4.61 | 7.63 ± 4.15 | 0.421 |
| Withdrawal time, min, mean ± SD | 9.50 ± 4.79 | 8.86 ± 5.56 | 0.520 |
| Variables | CGW ( | Control ( |
|
|---|---|---|---|
| Abdominal pain | 2 (3.3) | 1 (1.8) | 1.000 |
| Bloating | 3 (5.0) | 3 (5.5) | 1.000 |
| Nausea | 20 (33.3) | 9 (16.4) | 0.036 |
| Vomiting | 6 (10.0) | 2 (3.6) | 0.275 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsColorectal Cancer Screening and Detection · Gastrointestinal motility and disorders · Gastric Cancer Management and Outcomes
Introduction
Colorectal cancer (CRC) is the third-most common cancer worldwide [1]. The incidence rate of CRC has been increasing in China [2]. Colonoscopy is the most common approach for CRC screening [3]. Up to one-fifth of participants undergoing colonoscopy have constipation [4]. The quality of the bowel preparation has an effect on colonoscopy performance. Notably, patients with constipation have a lower quality of bowel preparation than those without [5]. Thus, it is of great importance to improve the bowel-preparation quality in such patients.
Constipated patients suffer from dysfunction of the intestinal motor and secretory activity [6]. It seems that sham feeding can activate the cephalic–vagal axis and stimulate the colonic motility and secretory activity [7]. Chewing gum is a convenient approach of sham feeding. However, whether chewing gum can improve bowel-preparation quality remains controversial. A previous randomized trial suggested that chewing gum added to high-dose senna before colonoscopy improved the quality of the bowel preparation [8]. In contrast, another randomized–controlled trial (RCT) failed to show any benefit of chewing gum in bowel cleaning, but it can improve patients’ satisfaction with the process of bowel preparation [9]. Additionally, few studies have investigated its effectiveness in constipated patients.
Poor compliance is another reason for inadequate bowel preparation [10]. In our previous study, short-message-service-enhanced instructions have improved the quality of bowel preparation probably via increasing the patients’ compliance [11]. Recently, WeChat has been the most widely used social software in China. Accordingly, it has been considered to be a more convenient approach for enhanced instructions instead of a short-message service.
In the current study, we aimed to evaluate whether chewing gum combined with WeChat-enhanced instruction can improve the quality of bowel cleansing as an adjunct to bowel preparation in constipated patients undergoing colonoscopy.
Methods
Study design and participants
A single-center, endoscopist-blinded RCT was conducted between February 2022 and August 2023 at the Department of Gastroenterology of the General Hospital of Northern Theater Command (Shenyang, P. R. China). The study protocol conformed to the ethical guidelines of the 1975 Declaration of Helsinki. This trial was approved by the Medical Ethical Committee of the General Hospital of Northern Theater Command (approval number Y [2023] 177) and registered at ClinicalTrials.gov (identifier NCT05447403). All patients provided written informed consent at the time of the colonoscopy appointment.
Inclusion criteria were as follows: (i) age ≥18 years; (ii) patients undergoing colonoscopy; (iii) diagnosis of constipation (according to the Rome IV criteria [12]); and (iv) written informed consent.
Exclusion criteria were as follows: (i) history of colorectal surgery; (ii) major psychiatric disorders; (iii) pregnancy or breastfeeding; (iv) contraindications for colonoscopy (e.g. heart failure, renal insufficiency); (v) suspicion of intestinal obstruction, stenosis, or perforation; (vi) allergy to gum ingredients and polyethylene glycol (PEG); or (vii) WeChat not available or could not be used by the patients themselves or their family members.
Randomization and blinding
Study group assignment was based on a computer-generated table of random numbers that was created by C.G. with random-numbers-generator software (Qi He Inc., Wu Han, P. R. China). Allocation concealment was achieved by using opaque sealed envelopes that contained the random numbers. During the process of the colonoscopy appointment, patients were assigned (1:1) to the chewing gum and WeChat-enhanced instruction (CGW) group and the control group by a nurse who was not involved in the acquisition and analysis of the data.
Patients were asked to refrain from discussing the bowel preparation with endoscopists and assistant nurses. Blinding of the patients was not possible due to the differences between the two bowel-preparation regimens.
Bowel-preparation regimens
Patients were informed to eat a semi-liquid and low-slag diet (which refers to very little dietary fiber or hard muscle fiber contained in the food) for breakfast and lunch, and a full-liquid diet for dinner on the day before the colonoscopy, and to fast on the day of the colonoscopy. A split-dose regimen of 3 L of PEG was used for all colonoscopies: patients were asked to take 1 bag of PEG with 1 L of water at 21:00 on the day before the colonoscopy, and the remaining two bags of PEG with 2 L of water at 4:00 and 30 mL of simethicone at 6:00 on the day of the colonoscopy as previously described [11, 13]. If a patient underwent colonoscopy in the afternoon, the remaining 2 L of PEG and simethicone were permitted to be taken at noon. If a patient felt that the bowel-preparation quality was inadequate after traditional bowel preparation, an additional bag of PEG could be taken. Even if a patient did not strictly obey the bowel-preparation regimen, we would discuss with him or her about whether the colonoscopy could be performed. Patients in the CGW group were asked to chew one piece of xylitol sugarless gum (Extra, Mars Inc., Guangzhou, P. R. China) for ∼20 min after drinking each 1 L of PEG.
Instructions
At our department, standard written instructions were provided for all patients, including: (i) colonoscopy appointment time; (ii) dietary guidance; and (iii) time and method for consuming the laxative. Patients in the CGW group received enhanced instruction via WeChat the day before the colonoscopy, including dietary guidance, instructions for laxative intake and chewing gum, and the importance of adequate bowel preparation. Patients in the control group would not receive any further enhanced instruction via WeChat.
Outcomes
The primary outcome was the quality of the bowel preparation, which was assessed by using the Boston Bowel Preparation Scale (BBPS) [14]. A total BBPS score of ≥6 with a BBPS score of ≥2 for each colon segment was considered to show adequate bowel preparation.
Secondary outcomes were as follows: (i) adenoma and/or polyp detection rate (ADR/PDR): proportion of patients with at least one adenoma and/or polyp detected during colonoscopy; (ii) number of polyps and/or adenomas; (iii) cecal intubation rate; (iv) insertion time: the time required to intubate the colonoscope to the cecum; and (v) withdrawal time.
Adverse events
Adverse events during or after bowel preparation were assessed before the colonoscopy procedure, including abdominal pain, bloating, nausea, and vomiting.
Sample-size calculation
A previous study reported that an adequate bowel-cleansing rate in the WeChat-enhanced instruction and the conventional instruction group was 89.8% and 66.4%, respectively [15]. Considering a type I (α) error of 5%, a type II (1-β) error of 10%, and a dropout rate of 20%, it was determined that 75 patients would be required in each group.
Statistical analysis
Continuous variables were expressed as means ± standard deviations and compared by using the Student’s t-test. Categorical variables were summarized as absolute frequencies and percentages, and analysed by using the chi-squared test or Fisher’s exact test for expected frequencies of <5. P-values of <0.05 were considered statistically significant. All analyses were performed by using SPSS software (Ver. 27.0; SPSS Inc., Chicago, Illinois, USA).
Results
Baseline characteristics
Among the 150 patients who were enrolled in this study, 21 canceled the colonoscopy. Besides, three patients forgot to report their previous colectomy, which were found during the colonoscopy, four patients lacked a BBPS score, and cecal intubation failed in seven patients due to colonic obstruction or intolerable pain. Finally, 115 eligible individuals were included in the final analysis. A flow diagram that describes the patient enrollment is shown in Figure 1.
Flowchart of patients’ enrollment. CGW = chewing gum and WeChat-enhanced instruction, BBPS = Boston Bowel Preparation Scale.
No significant differences were found between the CGW and control groups in terms of baseline characteristics (Table 1). Except for constipation, reasons for colonoscopy were abdominal pain (*n = *15) and bloating (*n = *5).
Primary outcome
The percentages of adequate bowel preparation between the CGW and control groups were not significantly different (76.7% vs 70.9%, *P = *0.312). There was no significant difference in the percentages of adequate bowel preparation for right, transverse, and left colon segments between the CGW and control groups (76.7% vs 70.9%, *P = *0.312; 96.7% vs 89.1%, *P = *0.109; 96.7% vs 87.3%, *P = *0.062).
No significant differences were found between the CGW and control groups in terms of BBPS scores (6.80 ± 1.42 vs 6.40 ± 1.78, *P = *0.184) (Table 2). The differences in the mean scores for right, transverse, and left colonic regions between the CGW and control groups were also insignificant (1.97 ± 0.66 vs 1.75 ± 0.58, *P = *0.061; 2.42 ± 0.56 vs 2.27 ± 0.71, *P = *0.227; 2.40 ± 0.56 vs 2.35 ± 0.75, *P = *0.662).
Secondary outcomes
The ADR/PDR was 55.0% in the CGW group and 52.7% in the control group (*P = *0.807). There was no significant difference in the number of polyps and/or adenomas between the CGW and control groups (1.3 ± 1.9 vs 1.2 ± 1.6, *P = *0.356). Only a few patients had diverticulosis (3 of 115, 2.6%) and protuberant or inflammatory lesions (7 of 115, 6.1%) (Table 2).
The rates of successful cecal intubation were comparable between the two groups (CGW group vs control group, 93.8% vs 94.8%, *P = *0.965). The reasons for incomplete colonoscopy included colorectal space-occupying lesions (CGW group vs control group, 5% vs 0%, *P = *0.245) and intolerable discomfort (CGW group vs control group, 3.3% vs 5.5%, *P = *0.459). There was no significant difference in the insertion and withdrawal times between the CGW and control groups (8.32 ± 4.61 vs 7.63 ± 4.15 min, *P = *0.421; 9.50 ± 4.79 vs 8.86 ± 5.56 min, *P = *0.520).
Adverse events
Regarding adverse events, the proportions of abdominal pain, bloating, or vomiting were comparable between the two groups (*P = *1.000, *P = *1.000, *P = *0.275, respectively). However, the incidence of nausea was higher in the CGW group than in the control group (33.3% vs 16.4%, *P = *0.036) (Table 3).
Discussion
The findings of this trial show that chewing gum combined with WeChat-enhanced instruction does not achieve a statistically significant improvement in the quality of bowel preparation before colonoscopy but does increase the incidence of nausea in constipated patients.
Patient factors are important determinants of suboptimal bowel preparation. Especially, one of the most common factors associated with bowel-preparation quality is constipation [16] and constipated patients have a higher risk of inadequate bowel preparation [5]. Several RCTs have evaluated the efficacy of stronger bowel-preparation regimens in constipated patients. The published RCTs usually choose the regimen of laxatives plus prokinetic drugs [17] or additional laxatives [18–20] and the control groups usually choose laxatives such as PEG [17–19] or sodium phosphate [20]. But the results of these RCTs are conflicting. Overall, insufficient evidence exists to provide an appropriate protocol for bowel preparation in these patients. In this setting, we attempted to explore the efficacy of chewing gum combined with WeChat-enhanced instruction for bowel preparation in this randomized–controlled endoscopist-blinded trial. Notably, whether chewing gum or WeChat-enhanced instruction can improve the quality of bowel preparation is still controversial among studies. One trial evaluated the efficacy and safety of high-dose senna plus chewing gum for bowel preparation before colonoscopy and found that chewing gum enhanced bowel cleansing [8]. But it should be noted that the regimen used for bowel cleansing was high-dose senna, which is uncommon in clinical practice. Another previous study showed that chewing gum could not improve the quality of bowel preparation, which was consistent with the findings of our study [9]. But it should be noted that the chewing-gum protocol was not common, in which patients in the gum group were asked to chew one piece of gum every 2 h until their colonoscopy examination, and the mean number of pieces of gum consumed was 2.8 ± 0.8. By comparison, our study employed split-dose bowel preparation and designed a more widely used protocol of chewing gum, in which patients chewed three pieces of gum in total to more accurately demonstrate the effect of chewing gum on bowel cleansing before colonoscopy. Besides, this previous study showed an improvement in patient satisfaction with the process of bowel preparation [9], which was contradictory to our findings that chewing gum increased the risk of nausea, probably due to the fact that patients were in an empty state during bowel preparation. Chewing gum may increase the secretion of gastric acid and gastrointestinal symptoms, such as nausea, especially in patients with gastritis, gastric ulcers, and chronic pharyngitis.
In the present study, the total BBPS score, the BBPS score of each colonic segment, and the percentage of adequate bowel preparation of all and each colonic segment were higher in the CGW group than in the control group, although the difference was not of statistical significance. However, we found that patients in the CGW group had a higher incidence of nausea than patients in the control group, which was in contrast to the results of earlier studies [8, 9, 21]. This indicates that chewing gum as an adjunctive treatment to a split dose of 3 L of PEG may not be suitable for constipated patients, primarily because they have already had dysfunction of intestinal motility. There is currently no effective choice for the radical treatment of constipation and most patients with constipation can only use laxatives to temporarily relieve symptoms in clinical practice. Therefore, a higher stimulus to activate gut motility would aggravate gastrointestinal symptoms, such as nausea.
This is the first RCT to assess the effect of chewing gum combined WeChat-enhanced instruction for bowel preparation in constipated patients. Our study has several limitations. There was a high cancelation rate for colonoscopy (14%), probably due to the prevention and control measures during the COVID-19 epidemic. As we used xylitol gum in the current trial and the effect of a sweet taste could not be completely excluded, this may be a variable that could have affected our current results. Lastly, it is hard for us to completely monitor whether each patient strictly chewed the gum for 20 min or no more than one piece of gum following each 1 L of PEG.
Conclusions
Chewing gum combined with WeChat-enhanced instruction in this single-center, endoscopist-blinded RCT of constipated patients did not improve the quality of bowel preparation before colonoscopy, but did increase the incidence of nausea. Although chewing gum is simple and inexpensive, whether it could be used in addition to a split-dose PEG preparation before colonoscopy needs further discussion. Modified regimens should be investigated with the aim to improve the quality of bowel preparation before colonoscopy in patients with constipation.
Authors’ contributions
X.Q. was responsible for conceptualization; C.G. and X.Q. were responsible for data analysis; C.G., Y.L., J.H., D.S. and X.Q. were responsible for data curation; C.G., W.W. and X.Q. were responsible for drafting; C.G., W.W., Y.L., J.H., D.S., D.Z. and X.Q. were responsible for revising the manuscript. D.Z. and X.Q. were responsible for the study supervision. All authors have read and approved the final version of the manuscript.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Sung H , Ferlay J, Siegel RL et al Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 2021;71:209–49.33538338 10.3322/caac.21660 · doi ↗ · pubmed ↗
- 2Li N , Lu B, Luo C et al Incidence, mortality, survival, risk factor and screening of colorectal cancer: a comparison among China, Europe, and northern America. Cancer Lett 2021;522:255–68.34563640 10.1016/j.canlet.2021.09.034 · doi ↗ · pubmed ↗
- 3Davidson KW , Barry MJ, Mangione CM et al; US Preventive Services Task Force. Screening for colorectal cancer: US Preventive Services Task Force recommendation statement. JAMA 2021;325:1965–77.34003218 10.1001/jama.2021.6238 · doi ↗ · pubmed ↗
- 4Gimeno-GARCíA AZ , Baute JL, Hernandez G et al Risk factors for inadequate bowel preparation: a validated predictive score. Endoscopy 2017;49:536–43.28282690 10.1055/s-0043-101683 · doi ↗ · pubmed ↗
- 5Gandhi K , Tofani C, Sokach C et al Patient characteristics associated with quality of colonoscopy preparation: a systematic review and meta-analysis. Clin Gastroenterol Hepatol 2018;16:357–69.e 10.28826680 10.1016/j.cgh.2017.08.016 · doi ↗ · pubmed ↗
- 6Camilleri M , Ford AC, Mawe GM et al Chronic constipation. Nat Rev Dis Primers 2017;3:17095.29239347 10.1038/nrdp.2017.95 · doi ↗ · pubmed ↗
- 7Roslan F , Kushairi A, Cappuyns L et al The impact of sham feeding with chewing gum on postoperative ileus following colorectal surgery: a meta-analysis of randomised controlled trials. J Gastrointest Surg 2020;24:2643–53.32103455 10.1007/s 11605-019-04507-3PMC 7595968 · doi ↗ · pubmed ↗
- 8ERGüL B , Filik L, KOçAKE et al Efficacy and safety of gum chewing in adjunct to high-dose senna for bowel cleansing before colonoscopy: a single-blind randomized controlled trial. Saudi J Gastroenterol 2014;20:356–9.25434316 10.4103/1319-3767.145325 PMC 4271010 · doi ↗ · pubmed ↗