Arachnoid Web With Atypical Imaging Findings and Clinical Manifestations: A Case Report
Eijiro Onishi, Yushi Sakamoto, Sadaki Mitsuzawa, Daiki Sako, Tadashi Yasuda

TL;DR
A 63-year-old man with a rare spinal arachnoid web showed unusual symptoms and MRI features, leading to successful surgical treatment.
Contribution
This case highlights atypical imaging and clinical features of spinal arachnoid web, aiding in its diagnosis.
Findings
MRI showed spinal cord atrophy and a dorsal flow void without the scalpel sign, indicating SAW.
Surgical resection improved some symptoms, but numbness and bladder dysfunction remained.
Asymmetric CSF pressure from the septum posticum may cause Brown-Sequard syndrome.
Abstract
Spinal arachnoid web (SAW) is a rare intradural lesion that can result in spinal cord compression and myelopathy. This report describes a case of SAW with atypical imaging findings and clinical manifestations in a 63-year-old male patient who presented with progressive lower limb paresthesia and left-dominant muscle weakness. The patient also exhibited temperature and pain sensory disturbances in the right leg. Magnetic resonance imaging (MRI) revealed spinal cord atrophy, intramedullary hyperintensity, and a dorsal flow void without the scalpel sign at the T7 level. Laminectomy and surgical resection of the SAW were performed. Intraoperative ultrasound revealed a SAW obstructing the flow of cerebrospinal fluid (CSF). The left and right sides of the posterior space were divided by the septum posticum, which moved pulsatile from side to side. Postoperative improvements in muscle…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
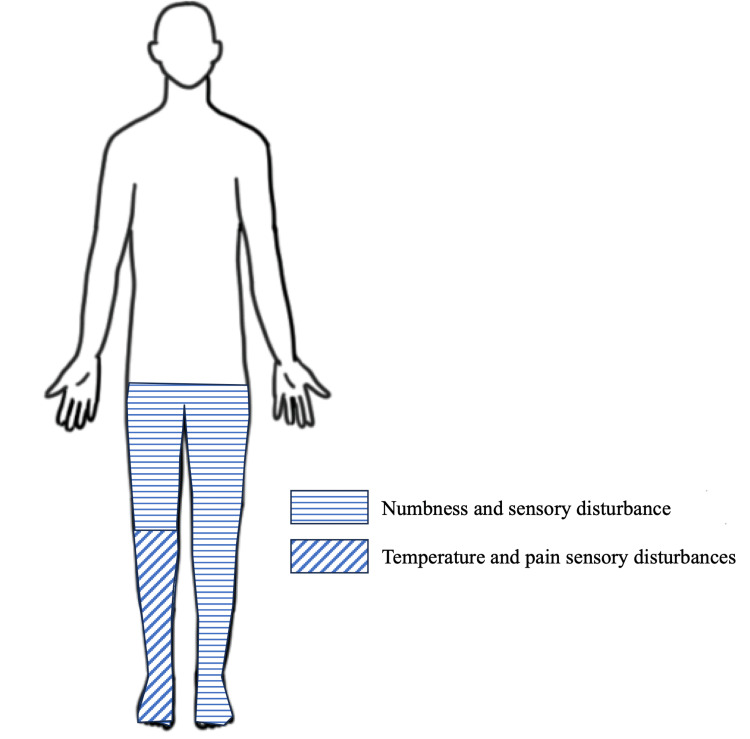 Figure 1
Figure 1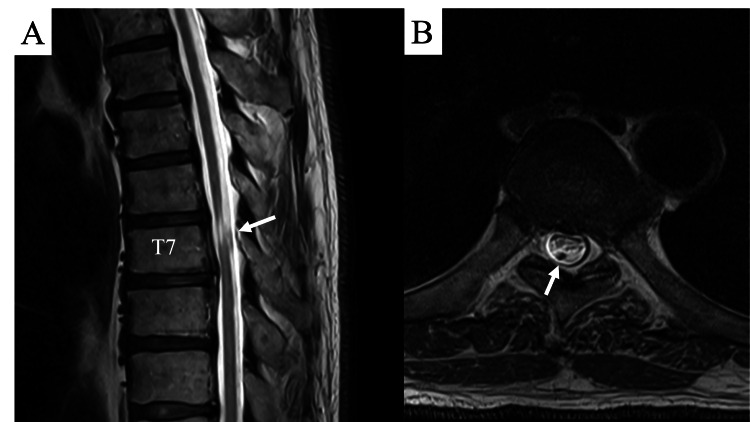 Figure 2
Figure 2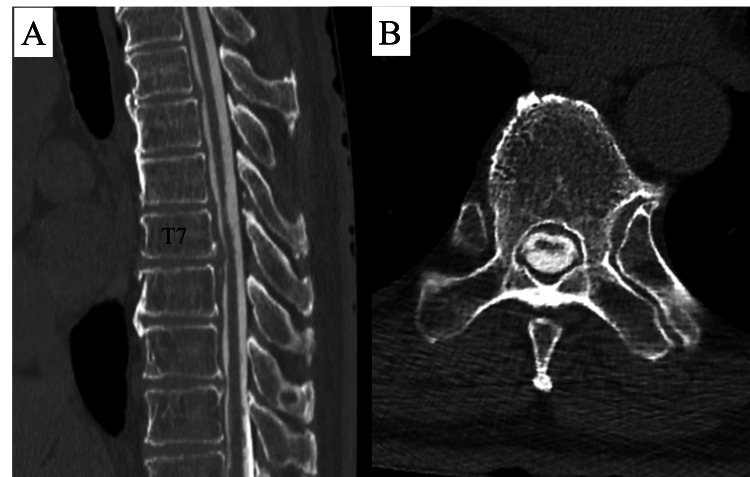 Figure 3
Figure 3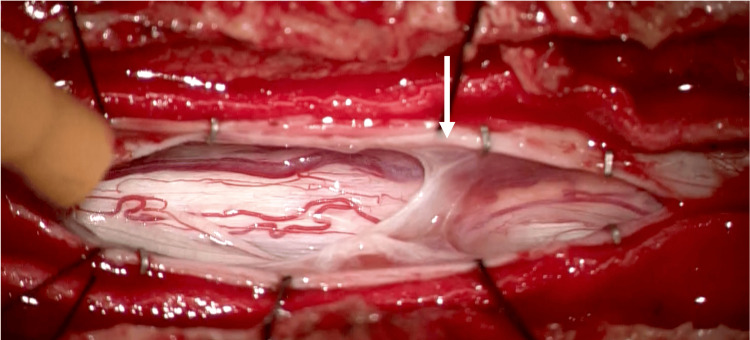 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCerebrospinal fluid and hydrocephalus · Fetal and Pediatric Neurological Disorders · Organ Donation and Transplantation
Introduction
Spinal arachnoid webs (SAWs) are rare and challenging-to-diagnose intradural lesions of the spinal cord and are often observed in the thoracic spinal cord of men in their fifth and sixth decades of life [1]. Thickening and scarring of the arachnoid tissue lead to localized cerebrospinal flow changes that compress the spinal cord from the posterior, resulting in spinal cord symptoms. Spinal cord compression frequently leads to the formation of a syrinx [1,2]. Symptoms associated with SAW primarily manifest as myelopathy, including sensory impairment, pain, lower limb muscle weakness, and bowel and bladder dysfunction [2-6]. Owing to the potential for a delayed initial diagnosis, treatment for this condition is often initiated after it has already progressed.
Directly visualizing SAWs by magnetic resonance imaging (MRI) and computed tomography (CT) is challenging, and the diagnosis is generally difficult. The scalpel sign, a scalpel-like deformation of the dorsal portion of the spinal cord caused by dorsal compression of the spinal cord due to SAW, is well known in imaging diagnosis and has been identified in many cases [1-3,7]. However, it is important to distinguish SAW from spinal cord herniation, a condition that presents with similar imaging findings [8].
Intraoperative ultrasound has been a reliable method for the definitive diagnosis of SAW and evaluation of the extension of the lesion. Furthermore, ultrasound has been shown to be a valuable tool in excluding other diseases, such as spinal cord herniation, and it may also be effective for evaluating cerebrospinal fluid (CSF) flow following SAW resection [1,2,9].
Herein, we report a case in which SAW was confirmed using intraoperative ultrasound in the absence of a clear scalpel sign on preoperative imaging. This is a rare case in which the patient presented with Brown-Sequard syndrome with left-right differences in the lower extremity symptoms, which may have been caused by differences in cerebrospinal pressure.
Case presentation
Patient presentation
A 63-year-old male patient had previously undergone endoscopic decompression surgery for lumbar spinal canal stenosis at another medical institution approximately a decade ago. Five years ago, he began to develop numbness and sensory disturbances in both lower limbs. Two years later, the patient developed dysuria necessitating intermittent self-urination. One month prior, the patient presented to our hospital with walking difficulty due to muscle weakness in the lower extremities. The muscle strength grade of the lower extremities was 4 on the right and 2 on the left, with the left lower extremity exhibiting more impairment. He demonstrated a marked reduction in ambulation and bowel and bladder disturbances. Numbness and sensory disturbances were observed in both lower limbs, with more severe numbness in the right lower limb. He also exhibited temperature and pain sensory disturbances in the right lower leg but not in the left leg (Figure 1).
Distribution of sensory disturbance.The patient exhibited numbness and sensory disturbances in both lower limbs. Temperature and pain sensory disturbances were observed in the right lower leg but not in the left leg.
Symptoms progressed with muscle weakness, demonstrating gradual exacerbation. The patient had no history of spinal trauma.
Radiological findings
Magnetic resonance images revealed spinal cord atrophy and flattening at the T6/7 level and intramedullary hyperintensities on T2-weighted MRI, suggesting spinal cord compression from the dorsal side. However, no scalpel sign or syrinx was identified (Figure 2).
Magnetic resonance images.A: Magnetic resonance image showing atrophy of the spinal cord at the T7 level and a flow void (white arrow) dorsal to the atrophic spinal cord. B: Horizontal slice showed a flattened spinal cord and flow void (white arrow).
An intradural flow void on MRI was also identified posterior to the spinal cord, where intramedullary hyperintensities were observed. Additionally, disc protrusions at the T6/7 and 7/8 levels were observed. Consequently, CT myelography results corroborated the MRI findings, indicating spinal cord atrophy, flattening, and mild anterior compression due to disc herniation. A horizontal slice of the CT scan at the T6/7 level revealed a slightly hyperdense contrast accumulation posterior to the atrophied spinal cord (Figure 3). Given the progressive nature of the symptoms, the surgical intervention was considered, with the differential diagnoses of spinal cord herniation, intervertebral disc herniation, intradural spinal cord tumor, and spinal arachnoid web.
CT images of myelogram.A: Computed tomographic myelography demonstrates the atrophy and flattening of the spinal cord at T. B: A horizontal slice showed a hyperdense contrast accumulation posterior to the atrophied spinal cord.
Treatment and outcome
As a definitive diagnosis could not be established preoperatively, the surgical procedure was undertaken by considering the aforementioned differential diagnosis. The surgical procedure involved laminectomy of the sixth to eighth thoracic vertebrae and exposure of the dura mater. Posterior fusion was performed to circumvent the potential consequences of a herniated disc. Subsequent to laminectomy, the dura mater was examined under the microscope, but no evident abnormal findings were identified. Consequently, the decision was made to search for intradural lesions using ultrasound. Regarding the sagittal ultrasonographic findings, the arachnoid membrane was attached to the dorsal surface of the spinal cord at the T7 level, forming an arachnoid web, and CSF was obstructed at this site. The spinal cord was compressed anteriorly and thinned at the same site. A space anterior to the spinal cord for the CSF was observed, thereby ruling out the possibility of spinal cord herniation (Video 1) [8].
Intraoperative ultrasonography image in the sagittal plane.Intraoperative ultrasonography image in the sagittal plane showing an arachnoid web. The spinal cord is compressed ventrally. The cerebrospinal fluid space is located anterior to the spinal cord.
Regarding the horizontal ultrasonographic findings (Video 2), horizontal sectioning at the T6 level, slightly more cranial than the arachnoid web, revealed increased CSF pressure in the dorsal spinal cord, indicating pulsatile anterior compression of the spinal cord. The left and right sides of the posterior space of the spinal cord were divided by the septum posticum, which moved in a pulsatile manner from side to side, suggesting a difference in cerebrospinal pressure between the left and right sides.
Ultrasonography image in the horizontal plane.Intraoperative ultrasound in the horizontal plane (the right side of the screen is on the left side). The septum separates the posterior CSF flow space.
Following the incision of the dura mater, the arachnoid membrane was scarred at the T7 level and adhered to the dorsal spinal cord, consequently obstructing the flow of CSF in the corresponding area (Figure 4). The arachnoid web adhering to the dorsal spinal cord was resected as far as possible laterally with micro scissors, and uncompromised arachnoid and dura mater were sutured in layers. Postoperatively, the patient demonstrated early improvement in lower extremity muscle strength, was able to ambulate with a cane, and exhibited resolution of right lower leg temperature and pain sensory disturbances. However, numbness in the lower extremities and bowel and bladder dysfunction persisted one year postoperatively.
Intraoperative microscopic photo.On the left is the cephalad side. Incision through the dura and arachnoid revealed a scarred arachnoid tissue at the T6/7 level adhering to the posterior surface of the spinal cord and obstructing CSF perfusion (white arrow: arachnoid web).
Discussion
SAW is an uncommon condition that often manifests as progressive myelopathy. Therefore, it is imperative to diagnose it promptly and offer suitable treatments. Here, two atypical findings of SAW were observed. First, the patient did not show the scalpel sign seen on MRI due to preoperative dorsal compression of the SAW, and he showed only spinal cord atrophy and intramedullary hyperintensities at the same site. Second, there were left-right differences in lower extremity neurological symptoms, with significant muscle weakness in the left and temperature and pain sensory disturbances in the right lower extremity.
Regarding the diagnosis of SAW, Reardon et al. have primarily described characteristic MRI findings, with a well-known sign being the so-called "scalpel sign" [7]. This sign, observed in all cases of SAW as reported by Voglis et al., involves spinal cord deformation due to dorsal compression by the SAW, which results in the appearance of a scalpel blade [3]. Additionally, a syrinx was present in 83% of patients. Consistent with these observations, systematic reviews have corroborated the scalpel sign as a hallmark feature of SAW. A comprehensive review by Vattipally et al. further substantiated the prevalence of the scalpel sign and noted its presence in 98% of cases [10]. Carr et al.'s systematic investigation of 127 SAW cases further refined the classification system by dividing the cases into three distinct groups based on MRI findings: type 1, spinal cord deformity only; type 2, cord deformity with myelomalacia; type 3, cord deformity with myelomalacia and syringomyelia. The findings showed that 54% of cases were classified as type 1, indicating that all cases of SAW resulted in some degree of spinal cord deformation [2].
In the present case, although spinal cord atrophy was observed, the characteristic scalpel sign was absent, rendering the MRI findings atypical and consequently challenging the definitive diagnosis of SAW before surgery. However, in the present case, a flow void was identified on MRI on the dorsal aspect of the spinal cord. Flow void represents a form of MRI artifact that refers to signal loss in moving fluids (usually blood, but also commonly observed in CSF or urine). Consequently, the presence of a flow void within a blood vessel is indicative of vascular patency. In the present case, the flow void was identified on the dorsal side of the flattened spinal cord on MRI. When considered in conjunction with the intraoperative ultrasound findings, it is hypothesized that the CSF colliding with the SAW at the same site caused a rapid change in CSF flow, which manifested as a flow void. Given the fact that SAW invariably causes CSF flow obstruction, a dorsal flow void may serve as a finding suggestive of SAW.
The patient presented with significant left-sided muscle weakness and temperature and pain sensory disturbance in the right lower extremity, which manifested as the Brown-Sequard syndrome. To the best of our knowledge, there have been no previous reports of similar symptoms. The most common symptoms of SAW are those associated with thoracic myelopathy, such as lower-extremity muscle weakness, gait disturbance, and numbness and pain in the lower extremities. Intraoperative ultrasonography is effective in the diagnosis of SAW and the evaluation of resection [9,10]. In this case, the septum posticum was seen to swing from side to side in the horizontal section, suggesting a left-right difference in the CSF perfusion in the posterior spinal cord. The left spinal fluid pressure was likely elevated relative to that of the right, resulting in a greater impact on the left side of the spinal cord. Postoperatively, there were signs of improvement in muscle strength, and the patient's right lower extremity temperature and pain sensory disturbances improved. Thus, SAWs can cause spinal cord pressure elevation due to impaired CSF flow from the posterior spinal cord, and the left-right difference in symptoms may be caused by the left-right difference in CSF pressure divided by the septum posticum during spinal cord compression. Brown-Sequard syndrome often occurs in cases of spinal cord herniation, and a differential diagnosis is necessary.
The etiology of SAW remains to be fully elucidated, but a previous multicenter study reported that 16% of patients with SAW had a history of previous spinal surgery. Conversely, most patients who underwent spinal surgery did not develop SAW, rendering the association uncertain [1]. In this case, the patient underwent lumbar endoscopic decompression surgery at another hospital, but details such as whether there was intraoperative dural injury were unknown, and it had been more than 10 years since the surgery, making an association unlikely.
The primary treatments for SAW are laminectomy and resection of the SAW [1,2,6,11]. A systematic review by Nisson et al. reported improvements in neurological symptoms in 91% of cases [1]. However, there are reports that surgery is unnecessary [10], and Carr et al. found that many cases of spinal deformity alone, i.e., without myelomalacia or a syrinx, do not require surgical intervention [2]. In the present case, the presence of myelomalacia in the spinal cord, as well as the patient's exhibited gait disturbance, necessitated surgical intervention. However, owing to the prolonged duration of the disease, some neurological symptoms persisted postoperatively. These findings emphasize the importance of an early and accurate diagnosis in the management of SAW.
Conclusions
The diagnosis of SAW is challenging, and the characteristic MRI findings include the scalpel sign and spinal deformities. The scalpel sign is observed in most patients; however, even in cases where it is not evident, if there are findings indicative of spinal cord compression and a flow void behind the spinal cord, SAW should be suspected, and surgical intervention may be considered. Notably, SAW has the potential to manifest as Brown-Sequard syndrome, as evidenced in the present case. The underlying pathophysiology is presumed to be attributable to the septum posticum, which generates a disparity in CSF pressure between the left and right sides of the dorsal spinal cord.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Arachnoid web of the spine: a systematic literature review J Neurosurg Spine Nisson PL Hussain I Härtl R Kim S Baaj AA 1751843120193100322010.3171/2019.1.SPINE 181371 · doi ↗ · pubmed ↗
- 2Surgical management of thoracic dorsal arachnoid webs: a 10-year single-institution experience World Neurosurg Carr MT Bhimani AD Schupper AJ 78179019320253943324910.1016/j.wneu.2024.10.055 · doi ↗ · pubmed ↗
- 3Spinal arachnoid web—a distinct entity of focal arachnopathy with favorable long-term outcome after surgical resection: analysis of a multicenter patient population Spine J Voglis S Romagna A Germans MR 1261352220223417546810.1016/j.spinee.2021.06.018 · doi ↗ · pubmed ↗
- 4Spinal arachnoid webs: presentation, natural history, and outcomes in 38 patients Neurosurgery Laxpati N Malcolm JG Tsemo GB 9179278920213443287810.1093/neuros/nyab 321 · doi ↗ · pubmed ↗
- 5Surgical treatment of spinal arachnoid web: report of two cases and literature review Surg Neurol Int Rodrigues AB Rodrigues DB Queiroz JW 316122021 https://pubmed.ncbi.nlm.nih.gov/34345457/3434545710.25259/SNI_493_2021 PMC 8326061 · doi ↗ · pubmed ↗
- 6Clinical characteristics, outcomes, and pathology analysis in patients with dorsal arachnoid web Neurosurgery Delgardo M Higgins D Mc Cormick KL Reid P Canoll P Mc Cormick PC 5815879020223529025510.1227/neu.0000000000001884 · doi ↗ · pubmed ↗
- 7Dorsal thoracic arachnoid web and the "scalpel sign": a distinct clinical-radiologic entity AJNR Am J Neuroradiol Reardon MA Raghavan P Carpenter-Bailey K 110411103420132334875910.3174/ajnr.A 3432 PMC 7964642 · doi ↗ · pubmed ↗
- 8Scalpel sign: dorsal thoracic arachnoid web, thoracic arachnoid cyst and ventral cord herniation Radiol Case Rep Buntting CS Ham Y Teng KX Dimou J Gauden AJ Nair G 356435691720223592334610.1016/j.radcr.2022.06.100PMC 9340144 · doi ↗ · pubmed ↗