Are mind-body therapies beneficial for older people with dementia? A Systematic Review and meta-analysis of randomized controlled trials
Zhengyang Mei, Chenyi Cai, Tingfeng Wang, Yuanzhuo Zhang, Wen Zhao, Chifong Lam, Shulai Luo, Yu Shi, Shi Luo

TL;DR
Mind-body therapies may help reduce symptoms like anxiety and depression in older people with dementia, but more high-quality research is needed.
Contribution
This study provides a systematic review and meta-analysis of mind-body therapies for behavioral and psychological symptoms of dementia in older adults.
Findings
MBTs improved behavioral and psychological symptoms of dementia (BPSD) with a standardized mean difference of -0.33.
Anxiety and depression symptoms were significantly reduced, but no significant effect was found for agitation.
The evidence certainty was rated as low to very low, indicating a need for more rigorous research.
Abstract
This systematic review and meta-analysis aimed to evaluate the potential multidomain benefits of mind-body therapies (MBTs) for behavioral and psychological symptoms of dementia (BPSD) in older people with dementia (OPWD). Relevant randomized controlled trials (RCTs) were identified using electronic databases and manual searches. Two independent researchers evaluated the risk of bias in the included trials using the Revised Cochrane Risk-of-Bias tool for randomized trials. A standardized mean difference (SMD) with a 95% confidence interval (CI) was used to combine effect sizes. This review included 35 RCTs comprising 4,043 patients, of whom 24 were included in the meta-analyses. MBTs effectively improved BPSD (SMD = -0.33; 95% CI -0.49 to -0.16; p < 0.01), anxiety (SMD = -0.82; 95% CI -1.53 to -0.10; p = 0.02), and depression (SMD = -0.57; 95% CI -1.06 to -0.08; p = 0.02), with no…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
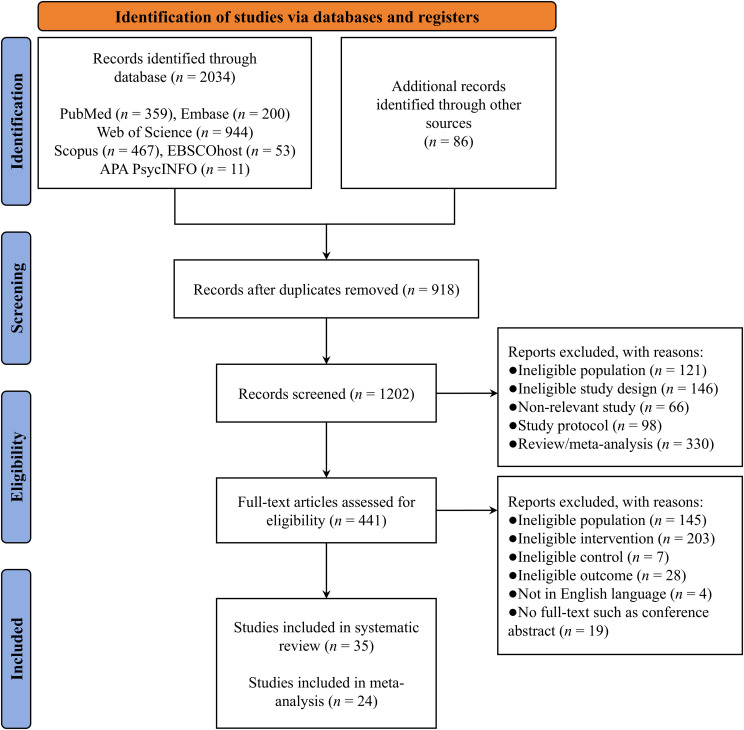 Figure 1
Figure 1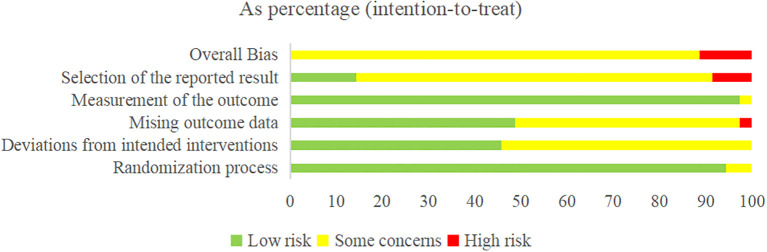 Figure 2
Figure 2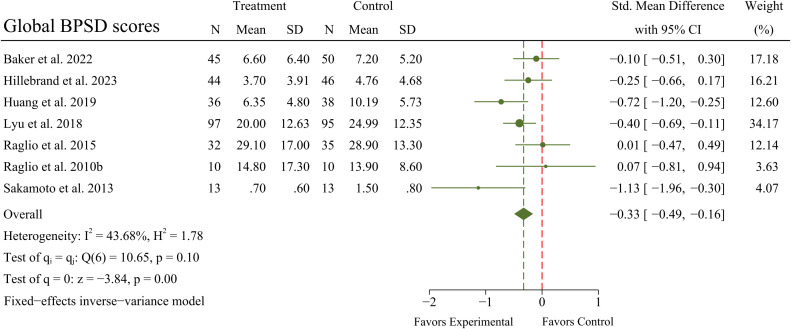 Figure 3
Figure 3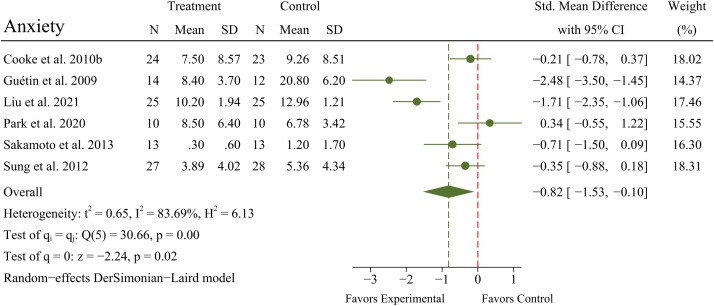 Figure 4
Figure 4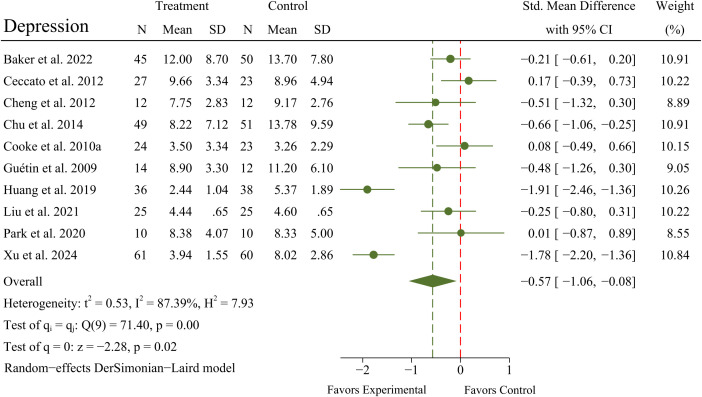 Figure 5
Figure 5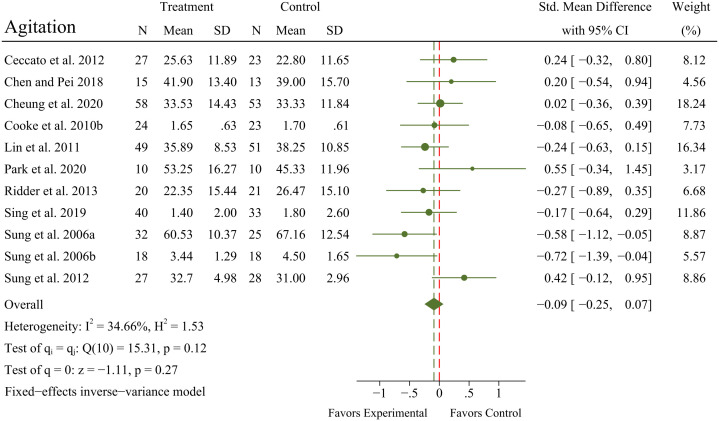 Figure 6
Figure 6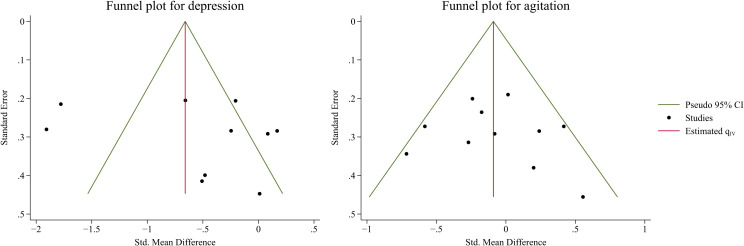 Figure 7
Figure 7| #1 | Dementia* [MeSH Terms] |
| #2 | Dementia* [Title/Abstract] OR Alzheimer* [Title/Abstract] OR Amentia* [Title/Abstract] |
| #3 | #1 OR #2 |
| #4 | Mind body* [Title/Abstract] OR Mind-body* [Title/Abstract] OR Mindfulness [Title/Abstract] OR Meditation [Title/Abstract] OR Shadow boxing [Title/Abstract] OR Tai Ji [Title/Abstract] OR Tai-ji [Title/Abstract] OR Tai Chi [Title/Abstract] OR Chi, Tai [Title/Abstract] OR Tai Ji Quan [Title/Abstract] OR Ji Quan, Tai [Title/Abstract] OR Quan, Tai Ji [Title/Abstract] OR Taiji [Title/Abstract] OR Taijiquan [Title/Abstract] OR T’ai Chi [Title/Abstract] OR Tai Chi Chuan [Title/Abstract] OR Qigong [Title/Abstract] OR Qi Gong [Title/Abstract] OR Ch’i Kung [Title/Abstract] OR Baduanjin [Title/Abstract] OR Yoga [Title/Abstract] OR Pilates [Title/Abstract] OR Exercise Movement Techniques [Title/Abstract] OR Movement Techniques, Exercise [Title/Abstract] OR Exercise Movement Technics [Title/Abstract] OR Pilates-Based Exercises [Title/Abstract] OR Exercises, Pilates-Based [Title/Abstract] OR Pilates Based Exercises [Title/Abstract] OR Pilates Training [Title/Abstract] OR Training, Pilates [Title/Abstract] OR Music* [Title/Abstract] |
| #5 | Older* [Title/Abstract] OR Elder* [Title/Abstract] OR Senior* [Title/Abstract] OR Aged [Title/Abstract] |
| #6 | Randomized controlled trial [Publication Type] OR Randomized [Title/Abstract] OR Placebo [Title/Abstract] |
| #7 | #3 AND #4 AND #5 AND #6 |
| Category | Inclusion criteria | Exclusion criteria |
|---|---|---|
| Population | Older people with dementia (age 60 years or older) | Not older people with dementia |
| Intervention | Mind-body therapies were used as the generic term for interventions including Mindfulness training, Tai Chi, Qigong, Baduanjin, Yoga, Pilates, Music therapy, etc | Interventions that were not mind-body therapies |
| Comparator | Control group receiving only routine treatment or appropriate rehabilitation intervention | No exclusion criteria |
| Outcome | Any assessment for behavioral and psychological symptoms of dementia | No exclusion criteria |
| Study design | All types of randomized controlled trials | Non-randomized controlled trials, such as uncontrolled before-after trials, quasi-experiments, literature review, study protocols, conference proceedings, comments, editorial, letter to editors, etc |
| Study ID | Country | Population | Age (Mean (SD)) | Total/M% | Diagnostic criteria | Intervention | Control | Outcome (measure) |
|---|---|---|---|---|---|---|---|---|
| Baker et al., 2022 ( | Australia | OPWD | T: 86.00 (7.50) | T: 45/NR | CDR/MMSE | Group music | SC | Depression (MADRS) |
| Ceccato et al., 2012 ( | Italy | OPWD | T: 85.50 (5.90) | T: 27/22.2% | DSM-IV | Traditional music | SC | Depression (GDS) |
| Chen and Pei, 2018 ( | China | OPWD | T: 77.30 (9.40) | T: 15/40.0% | Medical diagnosis/MMSE/CDR | Traditional music | TAU | Agitation (CMAI) |
| Cheng et al., 2012 ( | China | OPWD | T: 81.00 (7.70) | T: 12/50.0% | MMSE/CDR | Tai Chi | TAU | Depression (GDS) |
| Cheung et al., 2020 ( | China | OPWD | T: 85.71 (6.68) | T: 58/25.9% | Medical diagnosis/Global Deterioration Scale | Music with movement | TAU | Agitation (CMAI) |
| Chu et al., 2014 ( | China | OPWD | T+C: 82.00 (6.80) | T: 49/NR | DSM-IV | Group music | TAU | Depression (CSDD) |
| Churcher Clarke et al., 2017 ( | UK | OPWD | T: 81.30 (9.29) | T: 20/40.0% | Medical diagnosis/MMSE/DSM-IV | Mindfulness | TAU | Anxiety (RAID) |
| Cooke et al., 2010a ( | Australia | OPWD | T: NR | T: 24/NR | Medical diagnosis/MMSE/DSM-IV | Group music | TAU | Depression (GDS) |
| Cooke et al., 2010b ( | Australia | OPWD | T: NR | T: 24/NR | Medical diagnosis/MMSE/DSM-IV | Group music | TAU | Anxiety (RAID) |
| Giulietti et al., 2023 ( | Italy | OPWD | T: 82.80 (5.60) | T: 22/36.4% | NINCDS-ADRDA | Mindfulness | No-intervention | Depression (BDI) |
| Guétin et al., 2009 ( | France | OPWD | T: 85.20 (6.00) | T: 14/NR | Medical diagnosis | Personalized music | TAU | Anxiety (HAMA) |
| Harrison et al., 2021 ( | USA | OPWD | T: 79.70 (11.20) | T: 103/28.4% | Medical diagnosis | Personalized music | TAU | Agitation (CMAI) |
| Hillebrand et al., 2023 ( | Germany | OPWD | T: 83.84 (7.25) | T: 44/18.2% | Medical diagnosis | Personalized music | TAU | BPSD (DeCS) |
| Huang et al., 2019 ( | China | OPWD | T: 81.90 (6.00) | T: 36/NR | DSM-IV/CDR | Tai Chi | TAU | Depression (GDS) |
| Lin et al., 2011 ( | China | OPWD | T: 81.46 (7.34) | T: 49/46.9% | DSM-IV | Group music | TAU | Agitation (CMAI) |
| Liu et al., 2021 ( | China | OPWD | T: 86.56 (4.54) | T: 25/NR | CDR | Music with movement | TAU | Anxiety (HAMA) |
| Lyu et al., 2018 ( | China | OPWD | T: 68.90 (7.10) | T: 97/41.2% | NINCDS-ADRDA | Traditional music | TAU | BPSD (NPI) |
| McCreedy et al., 2022 ( | USA | OPWD | T: 79.80 (12.20) | T: 483/32.3% | Medical diagnosis | Personalized music | TAU | Agitation (CMAI) |
| Noone et al., 2023 ( | UK | OPWD | T: 77.80 (10.63) | T: 10/10.0% | DSM-IV/MMSE/PHQ | Mindfulness | TAU | Anxiety (RAID) |
| Park et al., 2020 ( | USA | OPWD | T+C: 84.30 (7.70) | T: 10/NR | Medical diagnosis/MMSE | Yoga | TAU | Anxiety (HADS) |
| Prick et al., 2024 ( | Netherlands | OPWD | T: 81.70 (7.60) | T: 49/38.8% | Medical diagnosis | Personalized music | TAU | BPSD (NPI) |
| Raglio et al., 2015 ( | Italy | OPWD | T: 81.70 (7.80) | T: 32/NR | DSM-IV/CDR/MMSE/NPI | Personalized music | SC | BPSD (NPI) |
| Raglio et al., 2010a ( | Italy | OPWD | T: 85.40 (6.50) | T: 30/3.3% | Medical diagnosis/MMSE/DSM-IV | Traditional music | SC | BPSD (NPI) |
| Raglio et al., 2010b ( | Italy | OPWD | T: 84.00 (6.00) | T: 10/20.0% | NINCDS-ADRDA | Traditional music | SC | BPSD (NPI) |
| Raglio et al., 2008 ( | Italy | OPWD | T: 84.40 (5.50) | T: 30/16.6% | DSM-IV/MMSE/CDR | Traditional music | SC | BPSD (NPI) |
| Ridder et al., 2013 ( | Denmark | OPWD | T: 82.17 (8.84) | T: 20/NR | Medical diagnosis/MMSE/Global Deterioration Scale | Personalized music | SC | Agitation (CMAI) |
| Sakamoto et al., 2013 ( | Japan | OPWD | T: 80.40 (7.41) | T: 13/15.4% | DSM-IV/MMSE/CDR | Personalized music | TAU | BPSD (BEHAVE-AD) |
| Sing et al., 2019 ( | China | OPWD | T: 85.00 (7.10) | T: 40/30.0% | Medical diagnosis | Group music | SC | BPSD (NPI) |
| Sisti et al., 2024 ( | USA | OPWD | T: 79.80 (12.20) | T: 483/32.3% | Medical diagnosis | Personalized music | TAU | BPSD (ABMI) |
| Sung et al., 2006a ( | China | OPWD | T: NR | T: 32/NR | Medical diagnosis | Personalized music | TAU | Agitation (CMAI) |
| Sung et al., 2006b ( | China | OPWD | T: 76.78 (9.12) | T: 18/61.1% | DSM-IV/Global Deterioration Scale | Music with movement | TAU | Agitation (CMAI) |
| Sung et al., 2012 ( | China | OPWD | T: 81.37 (9.14) | T: 27/NR | Medical diagnosis | Group music | TAU | Anxiety (RAID) |
| Vink et al., 2013 ( | Netherlands | OPWD | T: 82.42 (7.62) | T: 43/32.6% | DSM-IV | Group music | TAU | Agitation (CMAI) |
| Weise et al., 2020 ( | Germany | OPWD | T+C: 85.05 (5.93) | T: 10/NR | Medical diagnosis | Personalized music | Wait-list | Agitation (CMAI) |
| Xu et al., 2024 ( | China | OPWD | T: NR | T: 61/52.5% | Medical diagnosis | Group music | TAU | Depression (CSDD) |
| Study ID | Outcome | Domains | |||||
|---|---|---|---|---|---|---|---|
| D1 | D2 | D3 | D4 | D5 | Overall rating | ||
| Baker et al., 2022 ( | Depression | Low | Low | Some concerns | Low | Some concerns | Some concerns |
| Baker et al., 2022 ( | BPSD | Low | Low | Some concerns | Low | Some concerns | Some concerns |
| Ceccato et al., 2012 ( | Depression | Low | Some concerns | Low | Low | Low | Some concerns |
| Ceccato et al., 2012 ( | Agitation | Low | Some concerns | Low | Low | Low | Some concerns |
| Chen and Pei, 2018 ( | Agitation | Low | Low | Some concerns | Low | Low | Some concerns |
| Cheng et al., 2012 ( | Depression | Low | Some concerns | Low | Low | Some concerns | Some concerns |
| Cheung et al., 2020 ( | Agitation | Low | Low | Low | Low | Some concerns | Some concerns |
| Chu et al., 2014 ( | Depression | Low | Low | Low | Low | Some concerns | Some concerns |
| Churcher Clarke et al., 2017 ( | Anxiety | Low | Some concerns | Some concerns | Low | Some concerns | Some concerns |
| Churcher Clarke et al., 2017 ( | Depression | Low | Some concerns | Some concerns | Low | Some concerns | Some concerns |
| Cooke et al., 2010a ( | Depression | Low | Low | Some concerns | Low | Some concerns | Some concerns |
| Cooke et al., 2010b ( | Anxiety | Low | Low | Some concerns | Low | Some concerns | Some concerns |
| Cooke et al., 2010b ( | Agitation | Low | Low | Some concerns | Low | Some concerns | Some concerns |
| Giulietti et al., 2023 ( | Depression | Low | Some concerns | Low | Low | Some concerns | Some concerns |
| Guétin et al., 2009 ( | Anxiety | Low | Low | Some concerns | Low | Some concerns | Some concerns |
| Guétin et al., 2009 ( | Depression | Low | Low | Some concerns | Low | Some concerns | Some concerns |
| Harrison et al., 2021 ( | Agitation | Low | Some concerns | Some concerns | Low | Some concerns | Some concerns |
| Hillebrand et al., 2023 ( | BPSD | Low | Some concerns | High | Some concerns | Low | High |
| Huang et al., 2019 ( | Depression | Low | Some concerns | Some concerns | Low | Some concerns | Some concerns |
| Huang et al., 2019 ( | BPSD | Low | Some concerns | Some concerns | Low | Some concerns | Some concerns |
| Lin et al., 2011 ( | Agitation | Low | Some concerns | Low | Low | Some concerns | Some concerns |
| Liu et al., 2021 ( | Anxiety | Low | Some concerns | Low | Low | Some concerns | Some concerns |
| Liu et al., 2021 ( | Depression | Low | Some concerns | Low | Low | Some concerns | Some concerns |
| Lyu et al., 2018 ( | BPSD | Low | Some concerns | Low | Low | Some concerns | Some concerns |
| McCreedy et al., 2022 ( | Agitation | Low | Low | Some concerns | Low | Some concerns | Some concerns |
| Noone et al., 2023 ( | Anxiety | Low | Low | Some concerns | Low | Some concerns | Some concerns |
| Noone et al., 2023 ( | Depression | Low | Low | Some concerns | Low | Some concerns | Some concerns |
| Park et al., 2020 ( | Anxiety | Low | Low | Some concerns | Low | Some concerns | Some concerns |
| Park et al., 2020 ( | Depression | Low | Low | Some concerns | Low | Some concerns | Some concerns |
| Park et al., 2020 ( | Agitation | Low | Low | Some concerns | Low | Some concerns | Some concerns |
| Prick et al., 2024 ( | BPSD | Low | Low | Low | Low | High | High |
| Raglio et al., 2015 ( | BPSD | Low | Low | Some concerns | Low | Some concerns | Some concerns |
| Raglio et al., 2010a ( | BPSD | Low | Some concerns | Some concerns | Low | High | High |
| Raglio et al., 2010b ( | BPSD | Low | Some concerns | Low | Low | Low | Some concerns |
| Raglio et al., 2008 ( | BPSD | Low | Some concerns | Some concerns | Low | High | High |
| Ridder et al., 2013 ( | Agitation | Low | Low | Low | Low | Some concerns | Some concerns |
| Sakamoto et al., 2013 ( | BPSD | Low | Some concerns | Low | Low | Some concerns | Some concerns |
| Sing et al., 2019 ( | BPSD | Some concerns | Low | Some concerns | Low | Some concerns | Some concerns |
| Sisti et al., 2024 ( | BPSD | Low | Low | Some concerns | Low | Some concerns | Some concerns |
| Sung et al., 2006a ( | Agitation | Low | Some concerns | Low | Low | Low | Some concerns |
| Sung et al., 2006b ( | Agitation | Low | Some concerns | Low | Low | Some concerns | Some concerns |
| Sung et al., 2012 ( | Anxiety | Low | Some concerns | Low | Low | Some concerns | Some concerns |
| Sung et al., 2012 ( | Agitation | Low | Some concerns | Low | Low | Some concerns | Some concerns |
| Vink et al., 2013 ( | Agitation | Low | Low | Some concerns | Low | Some concerns | Some concerns |
| Weise et al., 2020 ( | Agitation | Some concerns | Some concerns | Low | Low | Some concerns | Some concerns |
| Xu et al., 2024 ( | Depression | Low | Some concerns | Low | Low | Some concerns | Some concerns |
| Outcome | Study omitted | SMD | 95% CI | |
|---|---|---|---|---|
| Lower bound | Upper bound | |||
| BPSD | Baker et al., 2022 ( | -0.37 | -0.56 | -0.19 |
| Hillebrand et al., 2023 ( | -0.34 | -0.53 | -0.16 | |
| Huang et al., 2019 ( | -0.27 | -0.45 | -0.09 | |
| Lyu et al., 2018 ( | -0.29 | -0.50 | -0.08 | |
| Raglio et al., 2015 ( | -0.37 | -0.55 | -0.20 | |
| Raglio et al., 2010b ( | -0.34 | -0.51 | -0.17 | |
| Sakamoto et al., 2013 ( | -0.29 | -0.46 | -0.12 | |
| Anxiety | Cooke et al., 2010b ( | -0.95 | -1.81 | -0.09 |
| Guétin et al., 2009 ( | -0.54 | -1.18 | 0.09 | |
| Liu et al., 2021 ( | -0.62 | -1.32 | 0.09 | |
| Park et al., 2020 ( | -1.02 | -1.78 | -0.27 | |
| Sakamoto et al., 2013 ( | -0.84 | -1.70 | 0.01 | |
| Sung et al., 2012 ( | -0.93 | -1.82 | -0.03 | |
| Depression | Baker et al., 2022 ( | -0.61 | -1.16 | -0.07 |
| Ceccato et al., 2012 ( | -0.65 | -1.16 | -0.14 | |
| Cheng et al., 2012 ( | -0.57 | -1.10 | -0.05 | |
| Chu et al., 2014 ( | -0.56 | -1.13 | 0.01 | |
| Cooke et al., 2010a ( | -0.64 | -1.16 | -0.13 | |
| Guétin et al., 2009 ( | -0.58 | -1.11 | -0.05 | |
| Huang et al., 2019 ( | -0.42 | -0.88 | 0.04 | |
| Liu et al., 2021 ( | -0.60 | -1.14 | -0.07 | |
| Park et al., 2020 ( | -0.62 | -1.14 | -0.11 | |
| Xu et al., 2024 ( | -0.43 | -0.85 | 0.01 | |
| Agitation | Ceccato et al., 2012 ( | -0.12 | -0.29 | 0.05 |
| Chen and Pei, 2018 ( | -0.10 | -0.27 | 0.06 | |
| Cheung et al., 2020 ( | -0.11 | -0.29 | 0.06 | |
| Cooke et al., 2010b ( | -0.09 | -0.26 | 0.07 | |
| Lin et al., 2011 ( | -0.06 | -0.23 | 0.11 | |
| Park et al., 2020 ( | -0.11 | -0.27 | 0.05 | |
| Ridder et al., 2013 ( | -0.08 | -0.24 | 0.09 | |
| Sing et al., 2019 ( | -0.08 | -0.25 | 0.09 | |
| Sung et al., 2006a ( | -0.04 | -0.21 | 0.12 | |
| Sung et al., 2006b ( | -0.05 | -0.22 | 0.11 | |
| Sung et al., 2012 ( | -0.14 | -0.31 | 0.03 | |
| Outcome | Risk of bias | Inconsistency | Indirectness | Imprecision | Publication bias | Certainty of the |
|---|---|---|---|---|---|---|
| BPSD | No downgrade, as trials at high risk of bias constituted less than 30%. | Downgrade by one level due to unexplained inconsistency ( | Downgrade by one level due to the inclusion of certain participants (OPWD). | No concerns (SMD = -0.33; 95% CI -0.49 to -0.16). | / | ⊕⊕⊝⊝ |
| Anxiety | No downgrade, as trials at high risk of bias constituted less than 30%. | Downgrade by two levels due to unexplained inconsistency ( | Downgrade by one level due to the inclusion of certain participants (OPWD). | No concerns (SMD = -0.82; 95% CI -1.53 to -0.10). | / | ⊕⊝⊝⊝ |
| Depression | No downgrade, as trials at high risk of bias constituted less than 30%. | Downgrade by two levels due to unexplained inconsistency ( | Downgrade by one level due to the inclusion of certain participants (OPWD). | No concerns (SMD = -0.57; 95% CI -1.06 to -0.08). | No publication bias is suspected. | ⊕⊝⊝⊝ |
| Agitation | No downgrade, as trials at high risk of bias constituted less than 30%. | Downgrade by one level due to unexplained inconsistency ( | Downgrade by one level due to the inclusion of certain participants (OPWD). | Some concerns (SMD = -0.09; 95% CI -0.25 to 0.07). Downgrade by one level. | No publication bias is suspected. | ⊕⊝⊝⊝ |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDementia and Cognitive Impairment Research · Schizophrenia research and treatment · Anxiety, Depression, Psychometrics, Treatment, Cognitive Processes
Introduction
1
Dementia is a progressive cognitive disorder that impairs daily functioning and is a primary contributor to dependency, disability, and death (1, 2). It is characterized by cognitive decline, deteriorating functional status, and worsening of neuropsychiatric symptoms (3). Currently, over 50 million individuals worldwide are affected by dementia, and projections indicate this figure could rise to 131 million by 2050 (3, 4). Moreover, the overall prevalence of dementia, from all causes, stands at 7.0%, with its rate of occurrence increasing sharply with age for both men and women (5), suggesting the growing public health challenge posed by dementia as the global population continues to age.
Old age is not only a critical stage for changes in physical and mental health but also a vulnerable period for the development of dementia. During this period, older people are often exposed to multiple risk factors for developing dementia, which are classified as immutable (age, sex, ethnicity, etc.) or potentially modifiable (diabetes, smoking, social isolation, physical inactivity, etc.) (6, 7). Moreover, compelling evidence suggests that dementia is prevalent among older people and may increase their susceptibility to physical and mental health problems, including cognitive impairment (8), suicidal behavior (9), epilepsy (10), disability (11), anxiety (12), and depression (13).
Dementia can be diagnosed based on medical history, cognitive and physical examination, laboratory testing, and brain imaging (3). As dementia is a progressive, incurable illness, several medications have been developed to help older people with dementia (OPWD) alleviate the physical and mental discomfort, including donepezil, cholinesterase inhibitors, memantine, and statins (14, 15). However, prolonged use of these drugs can result in numerous adverse outcomes. Specifically, the increasing use of cholinesterase inhibitors results in increased adverse drug reactions, such as cardiovascular and gastrointestinal adverse effects (16); treatment with antipsychotics in older people is associated with an increased risk of cardiovascular incidents and mortality (17). Therefore, no compelling evidence supports the use of these drugs in such patients (14).
In this regard, complementary therapies could offer potential solutions to these challenges. Mind-body therapies (MBTs), rooted in ancient Eastern practices, are a non-pharmacological approach that focuses on interactions between mind, body, and spirit to improve mental and physical well-being (18, 19). Compared with other medications, MBTs are characterized by low risk and high therapeutic benefits and can be alternatives or adjuvant approaches to conventional treatments (20, 21). Common MBTs include Mindfulness training, Tai Chi, Qigong, Baduanjin, Yoga, Pilates, and Music therapy, which have been proven to exert beneficial effects on the physical and mental health of OPWD (22–28). However, evidence regarding the efficacy of MBTs in managing the behavioral and psychological symptoms of dementia (BPSD) in OPWD is inconsistent, and some studies do not support the significant efficacy of MBTs in this area (29–33). This study aimed to evaluate the potential multidomain benefits of MBTs for BPSD in OPWD.
Methods
2
This systematic review and meta-analysis adhered to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 (34) and was registered in the International Prospective Register of Systematic Reviews (PROSPERO) under the registration number CRD42024559809.
Search methods
2.1
Using Medical Subject Headings in conjunction with Boolean and proximity operators, a search was conducted across six electronic databases: PubMed, Embase, Web of Science, Scopus, EBSCOhost, and APA PsycINFO, to identify relevant literature. The search covered the period from the inception of each database up to June 2024, and the strategy adhered to the Population, Intervention, Comparator, Outcome, and Study design framework. Details of the search strategy are outlined in Table 1, as per the PubMed database.
Inclusion and exclusion criteria
2.2
The criteria for inclusion and exclusion of studies are presented in Table 2.
Study selection and quality appraisal
2.3
Two independent researchers, following predefined inclusion and exclusion criteria, utilized EndNote 20.6 for study selection. After duplicates were eliminated, the remaining references were independently reviewed by both researchers based on titles, abstracts, and full texts. Quality appraisal of the included trials was conducted using the Revised Cochrane risk-of-bias tool for randomized trials, with evaluation across five bias domains: (a) randomization process, (b) deviations from intended interventions, (c) missing outcome data, (d) measurement of the outcome, and (e) selection of the reported result (35). Disagreements during study selection and quality appraisal processes were resolved through consultation with a third author.
Data extraction
2.4
Two independent researchers used a data extraction form to gather relevant information from each included trial. The extracted data comprised the following: (1) basic details such as the first author, country, and year of publication; (2) participant characteristics, including mean age (with standard deviation), sample size, and the percentage of male participants; (3) diagnostic criteria for dementia; (4) intervention and control conditions; and (5) outcome and measure.
Data synthesis
2.5
Given the differences in the measurement scales used for continuous variables (BPSD, anxiety, depression, and agitation) across the included trials, standardized mean differences (SMDs; Cohen’s d) with 95% confidence intervals (CIs) for each outcome were pooled and presented in forest plots using Stata software, version 18.0 (36). Statistical heterogeneity between trials was assessed using the chi-square test based on Q-test and *I^2^
- statistics, with a significance threshold of p-value < 0.10 (37). A sensitivity analysis was performed for each outcome using a stepwise elimination method to assess whether the pooled results were significantly affected by individual studies (36). Given the number of included trials, publication bias was examined by visual inspection of funnel plots and using Egger’s test (38, 39). The trim-and-fill method was used to assess the robustness of the findings in the presence of a publication bias (40). The certainty of evidence for each outcome was evaluated by two independent researchers using the Grading of Recommendations, Assessment, Development, and Evaluations (GRADE) guidelines (41). All statistical analyses were performed using Stata 18.0.
Results
3
Search outcomes
3.1
Searches of electronic databases and additional sources yielded 2,120 results, of which 918 were duplicates. After the titles and abstracts of the remaining 1,202 records were screened, the full text of 441 articles was assessed, resulting in 35 eligible randomized controlled trials (RCTs) (42–76). After 11 additional trials with missing quantitative data were excluded, 24 were included in the meta-analyses. A PRISMA flow diagram of the literature search is presented in Figure 1.
PRISMA flow diagram.
Study characteristics
3.2
The 35 included trials (see Table 3) were published between 2006 and 2024 and were conducted in various countries, including China (13 trials), Italy (6 trials), the United States (4 trials), Australia (3 trials), Germany (2 trials), the Netherlands (2 trials), the United Kingdom (2 trials), Denmark, France, and Japan (one trial each). In total, 2,065 patients were assigned to the experimental group, with a mean age ranging from 76.78 to 86.56 years, while 1,978 patients were assigned to the control group, with a mean age of 76.80 to 87.20 years.
Among the 35 included trials, the diagnostic criteria for dementia primarily consisted of medical diagnosis, Diagnostic and Statistical Manual of Mental Disorders-IV, Mini-Mental State Examination, Clinical Dementia Rating, and the Global Deterioration Scale. The interventions included personalized music (11 trials), group music (9 trials), traditional music (6 trials), mindfulness (3 trials), music with movement (3 trials), Tai Chi (2 trials), and yoga (1 trial). The controls included treatment as usual (25 trials), standard care (8 trials), no-intervention (1 trial), and wait-list (1 trial). In addition, the deliverers of the intervention primarily included music therapists, musicians, nursing staff, psychotherapist, and trained facilitators, all of whom were qualified to be responsible for the implementation of the intervention.
Quality appraisal
3.3
The risk of bias ranged from some concern to high (see Figure 2, Table 4). The main flaws (≥10% high risk) across the included trials were the randomization process (94.3% low risk, 5.7% some concerns, and 0.0% high risk); deviations from intended interventions (45.7% low risk, 54.3% some concerns, and 0.0% high risk); missing outcome data (48.6% low risk, 48.6% some concerns, and 2.8% high risk); outcome measurement (97.2% low risk, 2.8% some concerns, and 0.0% high risk); and selection of the reported results (14.3% low risk, 77.1% some concerns, and 8.6% high risk).
Risk-of-bias summary.
Pairwise meta-analyses
3.4
Effects of MBTs on BPSD
3.4.1
A meta-analysis of 7 RCTs (N = 564 patients) exhibited a significant improvement in BPSD (SMD = -0.33; 95% CI -0.49 to -0.16; p < 0.01) in OPWD, with no significant heterogeneity between RCTs (*I^2^
- = 43.68%; Q = 10.65; p = 0.10). A forest plot for BPSD is presented in Figure 3.
Main analyses for the effects of MBTs on BPSD.
Effects of MBTs on anxiety
3.4.2
A meta-analysis of 6 RCTs (N = 224 patients) exhibited a significant improvement in anxiety (SMD = -0.82; 95% CI -1.53 to -0.10; p = 0.02) in OPWD, but with significant heterogeneity between RCTs (*I^2^
- = 83.69%; Q = 30.66; p < 0.01). A forest plot for anxiety is presented in Figure 4.
Main analyses for the effects of MBTs on anxiety.
Effects of MBTs on depression
3.4.3
A meta-analysis of 10 RCTs (N = 607 patients) exhibited a significant improvement in depression (SMD = -0.57; 95% CI -1.06 to -0.08; p = 0.02) in OPWD, but with significant heterogeneity between RCTs (*I^2^
- = 87.39%; Q = 71.40; p < 0.01). A forest plot for depression is presented in Figure 5.
Main analyses for the effects of MBTs on depression.
Effects of MBTs on agitation
3.4.4
A meta-analysis of 11 RCTs (N = 618 patients) exhibited no significant improvement in agitation (SMD = -0.09; 95% CI -0.25 to 0.07; p = 0.27) in OPWD, with no significant heterogeneity between RCTs (*I^2^
- = 34.66%; Q = 15.31; p = 0.12). A forest plot for agitation is presented in Figure 6.
Main analyses for the effects of MBTs on agitation.
Sensitivity analyses
3.5
The results of the sensitivity analyses indicated that the pooled results for agitation and BPSD remained stable after excluding individual studies, indicating that these results were robust and insensitive to study selection. However, the pooled results for anxiety and depression were sensitive to study selection and were less robust when individual studies were excluded. The results of the sensitivity analyses are presented in Table 5.
Publication bias and certainty of evidence
3.6
Given the number of included trials with pooled results for depression and agitation, publication bias was assessed using funnel plots and the Egger’s test. Funnel plots for depression and agitation are presented symmetrically in Figure 7. The p-values of Egger’s test for depression and agitation were 0.42 and 0.55, respectively, indicating that publication bias did not affect this type of study. According to the GRADE ratings, the certainty of evidence across the outcomes ranged from low to very low, owing to inconsistency, indirectness, imprecision, and publication bias (see Table 6).
Publication bias for depression (left) and agitation (right).
Discussion
4
Previous studies have predominantly investigated the efficacy of single interventions for OPWD and have provided inconsistent evidence regarding various outcomes (23–33). This study aimed to evaluate the potential multidomain benefits of MBTs for BPSD in OPWD. The pooled results of the meta-analyses indicated that MBTs effectively improved BPSD (SMD = -0.33; 95% CI -0.49 to -0.16; p < 0.01), anxiety (SMD = -0.82; 95% CI -1.53 to -0.10; p = 0.02), and depression (SMD = -0.57; 95% CI -1.06 to -0.08; p = 0.02), with no significant improvements observed in agitation (SMD = -0.09; 95% CI -0.25 to 0.07; p = 0.27) among patients with dementia.
Music-based interventions are likely the most common MBT for alleviating BPSD in OPWD, as evidenced in 26 of the 35 trials. Previous studies have confirmed the effectiveness of music-based interventions, particularly in improving anxiety and depression (77–81). Music-based interventions are among the most effective approaches for managing BPSD in OPWD. However, a recent systematic review revealed that music-based interventions may not have achieved the anticipated efficacy, suggesting that the generalizability and applicability of this evidence require further examination (82). Overall, MBTs have significant therapeutic benefits in alleviating BPSD in OPWD, and the underlying mechanisms may be explained from several perspectives. Dementia is associated with the hypothalamus-pituitary-adrenal (HPA) axis and the autonomic nervous system (ANS), which are the main components of emotional regulation (83, 84). By reducing the HPA axis activation and reactivity, MBTs may alleviate the effects of stress and foster multiple positive downstream effects by shifting the ANS balance from primarily sympathetic to parasympathetic, leading to positive changes in cardiac vagal function, mood, energy state, and related neuroendocrine, metabolic, and inflammatory responses (85–89), which may play a potential role in mediating BPSD in OPWD. In addition, an increase in neurotransmitters such as serotonin and dopamine (responsible for regulating emotions and behavior) can be induced through exercise interventions included in MBTs (e.g., Tai Chi, Qigong, and Yoga), which help improve BPSD in OPWD (90).
BPSD represents a heterogeneous group of non-cognitive symptoms and behaviors that occur in patients with dementia, including anxiety, depression, agitation, irritability, apathy, and delusions (91–93). Therefore, in the quantitative analysis, BPSD was subdivided based on existing data to further clarify the efficacy of MBTs for these specific symptoms. Although the pooled results of the meta-analyses indicated that MBTs effectively improved BPSD in OPWD, this impact did not include all symptoms. For instance, according to the pooled results for agitation in OPWD, MBTs did not provide significant therapeutic benefits as previously assumed, which is consistent with previous evidence (30, 32). This may be because, for OPWD, especially those with advanced dementia, the inability to perform activities of daily living, often accompanied by clinical complications such as dysphagia and infections (14), presents a significant challenge in addressing behavioral disorders (including agitation and aggressive tendencies) with short-term MBTs. Finally, in terms of improving anxiety and depression in OPWD, evidence confirming the therapeutic benefits of MBTs is urgently required because of the significant heterogeneity or sensitivity to study selection in the pooled results. This may stem from the fact that the specific interventions, implementation steps, and duration of the interventions varied between studies, resulting in large differences in effect sizes. Additionally, the CIs for certain pooled results were near the threshold of statistical significance after excluding individual studies. This indicates that the sample size and experimental design need to be further increased and refined to more precisely evaluate the potential benefits of MBTs on these outcomes.
Although MBTs are promising complementary therapies for enhancing physical and mental health in OPWD, their differential efficacy should be further explored and validated. Most existing trials focus on the efficacy of a single intervention for BPSD in OPWD while ignoring the differential efficacy between various interventions. This may lead to an overestimation of the actual efficacy of MBTs in clinical practice. In the context of limited medical resources and the increasing prevalence of dementia, MBTs that can be effectively applied to clinical practice should be identified. Doctors and nurses are inclined to use non-pharmacological treatments more than pharmacological treatments in clinical practice (94). Therefore, comparisons between non-pharmacological treatments should receive more attention. A network meta-analysis suggests that individualized nursing, behavior therapy, and reminiscence therapy have significant potential in improving BPSD in OPWD, particularly in reducing anxiety and depression (95). Thus, the differential efficacy of non-pharmacological treatments in improving various aspects of BPSD should be further examined to maximize the clinical benefits of non-pharmacological treatments in the context of limited medical resources. Notably, the efficacy of MBTs in improving BPSD in OPWD may vary depending on the intervention period, frequency, and duration, suggesting that the dose-response relationship of MBTs in this regard is also an important area for investigation. Although this study did not reveal the optimal dosage of MBTs for improving BPSD in OPWD, existing research indicates that the intervention period, frequency, and duration are critical factors influencing efficacy (31, 33, 96). Short-term, high-frequency interventions may lead to faster clinical improvements to some extent, while long-term, low-frequency interventions may help maintain long-term efficacy. Therefore, more high-quality RCTs must be conducted to explore the dose-response relationship of MBTs in improving BPSD in OPWD, and intervention programs should be flexibly adjusted in clinical practice based on patients’ individual differences to achieve the best therapeutic outcomes.
Limitations
5
The findings of this systematic review and meta-analysis should be interpreted in the context of these limitations. First, owing to the limited information available on the study population from existing trials, this study mainly examined the overall therapeutic benefit of MBTs for OPWD and did not make specific distinctions based on the type and course of dementia. Second, although there was significant heterogeneity in the pooled results for some outcomes, sources of heterogeneity were not identified because of study data limitations. To address this problem, more comprehensive data should be collected in future studies. Finally, for some outcomes such as anxiety and depression, the pooled results were sensitive to study selection and were less robust; thus, the findings should be interpreted cautiously.
Conclusions
6
Effective nursing for patients with dementia is vital, as they are undergoing a major transition in their physical and mental health. Although MBTs effectively improved BPSD in OPWD to some extent, the dose-response relationship of MBTs in improving various aspects of BPSD remains unclear, and these relationships may be influenced by the intervention period, frequency, and duration. In clinical practice, healthcare and social care therapists should develop personalized intervention programs based on patient individual differences and the actual dose-response relationship, which will help maximize the clinical benefits of non-pharmacological treatments in the context of limited medical resources.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Malik R Kalra S Bhatia S Al Harrasi A Singh G Mohan S . Overview of therapeutic targets in management of dementia. Biomed Pharmacother. (2022) 152:1–15. doi: 10.1016/j.biopha.2022.113168 35701303 · doi ↗ · pubmed ↗
- 2Kornblith E Bahorik A Boscardin WJ Xia F Barnes DE Yaffe K . Association of race and ethnicity with incidence of dementia among older adults. JAMA. (2022) 327:1488–95. doi: 10.1001/jama.2022.3550 PMC 902021535438728 · doi ↗ · pubmed ↗
- 3Arvanitakis Z Shah RC Bennett DA . Diagnosis and management of dementia. JAMA. (2019) 322:1589–99. doi: 10.1001/jama.2019.4782 PMC 746212231638686 · doi ↗ · pubmed ↗
- 4Grande G Qiu C Fratiglioni L . Prevention of dementia in an ageing world: Evidence and biological rationale. Ageing Res Rev. (2020) 64:101045. doi: 10.1016/j.arr.2020.101045 32171784 · doi ↗ · pubmed ↗
- 5Cao Q Tan C-C Xu W Hu H Cao X-P Dong Q . The prevalence of dementia: a systematic review and meta-analysis. J Alzheimer’s Dis. (2020) 73:1157–66. doi: 10.3233/JAD-191092 31884487 · doi ↗ · pubmed ↗
- 6Licher S Ahmad S Karamujić-ČomićH Voortman T Leening MJ Ikram MA . Genetic predisposition, modifiable-risk-factor profile and long-term dementia risk in the general population. Nat Med. (2019) 25:1364–9. doi: 10.1038/s 41591-019-0547-7 PMC 673922531451782 · doi ↗ · pubmed ↗
- 7Livingston G Huntley J Sommerlad A Ames D Ballard C Banerjee S . Dementia prevention, intervention, and care: 2020 report of the Lancet Commission. Lancet. (2020) 396:413–46. doi: 10.1016/S 0140-6736(20)30367-6 PMC 739208432738937 · doi ↗ · pubmed ↗
- 8Amariglio RE Donohue MC Marshall GA Rentz DM Salmon DP Ferris SH . Tracking early decline in cognitive function in older individuals at risk for Alzheimer disease dementia: the Alzheimer’s Disease Cooperative Study Cognitive Function Instrument. JAMA Neurol. (2015) 72:446–54. doi: 10.1001/jamaneurol.2014.3375 PMC 439716425706191 · doi ↗ · pubmed ↗