A Canadian algorithm for upper gastrointestinal cancer management
Frédéric Lemay, Amindeep S. Sandhu, Barry D. Stein, Rachel Goodwin

TL;DR
This paper presents a new Canadian algorithm for managing upper gastrointestinal cancers, incorporating expert opinions and patient input to guide treatment and improve care.
Contribution
The novel contribution is a case-based educational program leading to a practical algorithm for upper GI cancer management in Canadian clinical practice.
Findings
An algorithm was developed integrating expert and patient input for upper GI cancer care.
The algorithm includes recommendations for immune checkpoint inhibitors and supportive care.
A needs assessment identified educational gaps in upper GI cancer treatment.
Abstract
Recent advances in immunotherapy have changed the treatment landscape for cancers of the upper gastrointestinal (GI) system. Immune checkpoint inhibitors can lead to better survival and improved quality of life for affected individuals. Adopting new treatment strategies in real-world practice can be challenging, and algorithms that are easy to implement in Canadian oncology practices would benefit clinicians and patients. In this study, we present expert opinion on best practices for upper GI cancer management, including a new algorithm that integrates the latest evidence for screening, workup, diagnosis, treatment, and survivorship. The algorithm is based on a novel approach comprising a case-based, accredited educational program with asynchronous discussion among clinicians practicing across Canada, with the input of expert medical oncologists and gastroenterologists. A needs…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
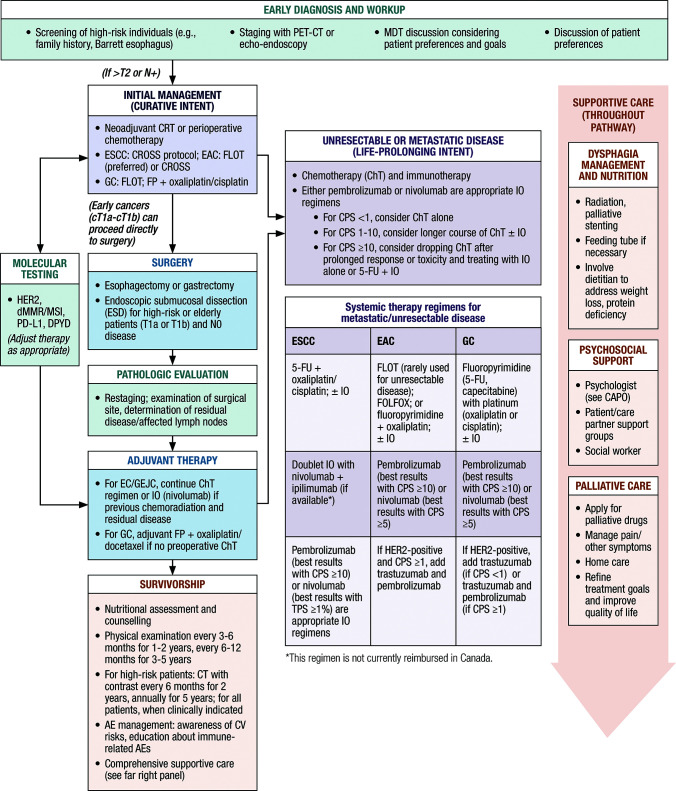 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGastric Cancer Management and Outcomes · Colorectal and Anal Carcinomas · Cancer Immunotherapy and Biomarkers
Introduction
1
Cancers of the upper gastrointestinal (GI) system are aggressive and heterogeneous. Esophageal cancer (EC), gastroesophageal junction cancer (GEJC) and gastric cancer (GC) are often diagnosed at advanced stages, and as a result, treatment options are limited (1–3). Interdisciplinary management and comprehensive supportive care are crucial (1).
Immunotherapy has improved survival and quality of life for individuals with EC and GC (4, 5). However, treatment paradigms are still being refined (1, 2, 6, 7), and individuals who are treated at high-volume centers tend to have better outcomes (8, 9). An Ontario study reported worse survival in routine practice compared with clinical trials (10). In an American study, one-quarter of patients with advanced cancer received no treatment, and treatment was of limited duration (3). Clinicians aiming to improve outcomes would benefit from guidance on integrating novel therapies into treatment and optimizing interdisciplinary care.
Current care pathways (11–14) may not reflect the latest advances and may not apply to all regions. In this Perspective we present expert opinion on best practices, based on an educational program with 77 participants from practice settings across Canada, with input from an expert Scientific Planning Committee. These best practices include patient input and reflect the latest evidence as it applies to the Canadian health care system.
Algorithm development
2
The algorithm was developed through an accredited educational program supported by the Canadian Association of Gastroenterology (CAG) (15). The program provided an opportunity for discussion and consensus on best practices. The Scientific Planning Committee included experts with diverse backgrounds and practice settings who treat upper GI cancers: two gastroenterologists (one representing the CAG; FL and AS), a medical oncologist (RG), and a patient representative (BDS). The patient representative’s role was to ensure that patient perspectives were included in all stages of the program and in the final algorithm.
To assess educational needs, a survey was distributed to Canadian health care professionals who treat GI cancers. Questions addressed their needs for education related to diagnosis, treatment, supportive care, and other aspects of interest. The respondents were primarily medical oncologists and gastroenterologists, with other specialties such as pharmacists and oncology nurses also represented. The identified areas of educational need included biomarker testing, immunotherapy, recent clinical trials, and treatment algorithms.
The program was designed to address these areas. Three fictional case studies were developed. Seventy-seven participants, practicing in community and academic settings from all provinces and the Yukon Territory, provided feedback through an online discussion board. Participants’ specialties were primarily gastroenterology or medical oncology, but family physicians, pharmacists, and pathologists were also represented.
After providing input regarding the initial cases, participants submitted anonymized cases based on their experience, and five cases were chosen for further discussion. The patient cases and peer discussions were available for all participants to see. The information from the discussions was collected and organized into best practices for diagnosis, management with curative intent, and management of advanced disease. The process of collecting, analyzing, and organizing the best practices was overseen by the Scientific Planning Committee (including a CAG representative). The results were summarized in a share-back presentation, which is available online along with the rest of the program (15). Finally, the best practices were assembled into an algorithm. The participants and the CAG have access to all materials and discussions.
Treatment algorithm
3
Overview
3.1
Figure 1 illustrates the steps for the diagnosis and treatment of upper GI cancers. Initial management should include either neoadjuvant chemoradiotherapy (CRT) with immunotherapy, perioperative chemotherapy (ChT), or surgery. Definitive CRT may be employed if the patient does not desire or is not eligible for surgery, whereas systemic therapy is required for unresectable disease. Systemic therapy includes ChT with a fluoropyrimidine and platinum; immune checkpoint inhibitors can extend survival (16, 17). Immunotherapy has been associated with improved quality of life (QoL) relative to ChT alone (5).
Canadian algorithm for the management of upper GI cancers. AEs, adverse events; CAPO, Canadian Association of Psychosocial Oncology; ChT, chemotherapy; CPS, combined positive score; CROSS, Chemoradiotherapy for Esophageal Cancer Followed by Surgery Study; dMMR, deficient mismatch repair; CT, computed tomography; DPYD, dihydropyrimidine dehydrogenase; EAC, esophageal adenocarcinoma; ESCC, esophageal squamous cell carcinoma; FLOT, fluorouracil, leucovorin, oxaliplatin, and docetaxel; FOLFOX, folinic acid, fluorouracil and oxaliplatin; FP, fluoropyrimidine; 5-FU, 5-fluorouracil; GC, gastric cancer; HER2, human epidermal growth factor receptor 2; IO, immunotherapy; MDT, multidisciplinary team; MSI, microsatellite instability; PD-L1, programmed cell death ligand 1; PET-CT, positron emission tomography-computed tomography; TPS, tumor proportion score.
All individuals should be treated by expert multidisciplinary teams. It is essential to discuss patient preferences and goals early on (18). Individuals often have impaired QoL, and survivorship is a fundamental aspect of management (19, 20). Regular follow-up is required to monitor disease progression, and most patients require symptom management (21). Comprehensive supportive care is needed.
Best practices and rationale
3.2
Diagnosis and workup
3.2.1
Clinicians should be aware of risk factors and screen patients with alarm symptoms. Early diagnosis is challenging but important to improve outcomes. There is no evidence to support screening for EC among patients presenting with gastroesophageal reflux disease (GERD) only (22). Patients with alarm symptoms such as dysphagia, odynophagia, anemia, weight loss, recurrent vomiting, loss of appetite, or GI bleeding should be evaluated. Risk factors for EAC include male sex, older age, White race, Barrett esophagus, nocturnal reflux, abdominal obesity, and tobacco use (23, 24). Risk factors for ESCC include low socioeconomic status, tobacco or alcohol use, consumption of hot or pickled foods, low consumption of fruits and vegetables, and radiation exposure (25).
The workup includes a complete blood count, metabolic panel, HbA1C, and EKG. Thorough staging is important to optimize therapy (26). PET-CT should be employed to confirm the diagnosis and the clinical stage, and to identify metastatic disease (27, 28); echo-endoscopy is another option (22, 29). For GC, a diagnostic laparoscopy may be part of the workup, and ferritin and vitamin B_12_ levels should be assessed. Clinicians should be aware of red flags for genetic contributions. If diffuse-type cancer is found, consider a detailed family history and genetic testing (30).
Patients should receive a baseline malnutrition assessment and follow-up. The Canadian Nutrition Screening Tool can identify patients who are at risk of malnutrition (31). The Canadian Malnutrition Task Force offers a toolkit and resources (32).
Reflex molecular testing is recommended. DPYD gene variant carriers are at risk for severe toxicity with ChT (33). Clinical judgment is required; most research has been carried out in Caucasians, and individuals of other ethnicities may need further testing (34–37). HER2 expression guides the selection of targeted therapy (trastuzumab), whereas dMMR/MSI and the PD-L1 combined positive score (CPS) or tumor proportion score (TPS) determine immunotherapy eligibility (38).
Treatment of localized disease with curative intent
3.2.2
Esophagectomy and gastrectomy are the recommended modalities for patients with early-stage EC/GC and good performance status. Patients should undergo a perioperative assessment. Endoscopic submucosal dissection can be considered if the patient has the appropriate T stage, N0 disease, and is at high risk for open surgery complications. Upfront resection may be considered, but this can understage disease. Clinicians should assess whether the patient desires surgery. We recommend that care partners be included in all treatment decisions.
Multidisciplinary team (MDT) discussions that include a thoracic surgeon should be held for all patients. MDT discussion is essential, especially if the cancer is upstaged after PET-CT. Clinicians should consider whether research protocols are available.
Patients should receive neoadjuvant CRT with immunotherapy, or perioperative ChT. Curative-intent strategies include CROSS for ESCC (carboplatin + paclitaxel with radiotherapy), and perioperative FLOT (5-fluorouracil, leucovorin, oxaliplatin, and docetaxel) for EAC/GEJC/GC (39, 40). Other ChT regimens for ESCC include FOLFOX (folinic acid, fluorouracil, and oxaliplatin), carboplatin/etoposide, and carboplatin/paclitaxel. CROSS is an option for EAC/GEJC, but as shown by the ESOPEC trial, FLOT is preferred based on longer overall survival (OS) (41). Treatment decisions should be made in a multidisciplinary forum.
For GC, ChT options include perioperative FLOT, a fluoropyrimidine + cisplatin/oxaliplatin, and an adjuvant fluoropyrimidine with oxaliplatin or docetaxel (if there was no preoperative ChT). In the curative setting, there is currently no role for HER2-directed therapy. Clinicians should refer to provincial or international guidelines for further details of regimens (11–14, 17, 29, 42, 43)
The addition of immunotherapy to neoadjuvant or perioperative ChT is still experimental (2). Perioperative durvalumab + FLOT improved the rate of pathological complete response (pCR) in patients with GC/GEJC, compared with placebo + FLOT, in MATTERHORN (44). In KEYNOTE-585, neoadjuvant and adjuvant pembrolizumab added to ChT improved pCR among participants with resectable GC/GEJC (45). For MSI-H/dMMR GC/GEJC, trials suggest an important role of neoadjuvant immunotherapy (46). The NEONIPIGA trial reported 58.6% pCR after neoadjuvant nivolumab + ipilimumab, and the INFINITY trial demonstrated 60% pCR among patients who received neoadjuvant durvalumab + tremelimumab (47, 48). Patients with resectable MSI-H/dMMR adenocarcinoma should be included in a clinical trial or offered immunotherapy, if available.
Antibiotics should be prescribed carefully. Antibiotics within 1-2 months of initiating immunotherapy have been linked to poor survival (49–51). Clinicians should carefully consider antibiotics and should not prescribe them reflexively.
Patients with EC/GEJC who received neoadjuvant CRT and have residual disease should receive adjuvant immunotherapy. Adjuvant nivolumab improves disease-free survival (DFS) among patients with residual EC/GEJC after surgery and neoadjuvant CRT (52). CheckMate 577 identified a 31% risk reduction for disease progression or death among patients who received one year of nivolumab vs placebo (53). Patients should be educated on recognizing immune-related AEs.
Assessing patient and care partner preferences
3.2.3
The individual’s and care partner’s preferences should be discussed throughout the treatment journey. Many patients value autonomy in deciding whether to undergo surgery, choosing a systemic therapy, or changing therapy (18, 54–58). Integrating patient preferences into decision-making can improve compliance and increase the personalization of care (54, 59). Rather than facing difficult decisions alone, patients often wish to consider the needs of their loved ones and receive their support (60). Including care partners in decision-making enhances patients’ ability to process large amounts of new information and manage psychological distress (60, 61). Hence, both patients and care partners require reliable information and decision support (60, 62).
Follow-up after surgery
3.2.4
Because of the complex nature of upper GI cancers, multipronged follow-up is essential. There is no standard, but a reasonable surveillance program would include a physical examination every 3-6 months for 1-2 years, then every 6-12 months for 3-5 years. For high-risk patients, CT of the chest and abdomen (with oral and IV contrast, unless contraindicated) should be considered every 6 months for the first 2 years and annually for up to 5 years (29). Surveillance endoscopy is controversial (63).
If the cancer recurs, restaging with CT is required. Local esophageal recurrence may require stenting or palliative radiation, but left laryngeal nerve involvement is a concern. Proximal tumors are difficult to stent due to their proximity to the upper esophageal sphincter.
Treatment of unresectable/metastatic disease with life-prolonging intent
3.2.5
Immunotherapy should be incorporated into treatment for eligible individuals. The benefit of adding immunotherapy to ChT has been demonstrated in clinical trials, and efficacy correlates with PD-L1 expression. A general rule is as follows:
For CPS <1, consider ChT aloneFor CPS 1-10, consider a longer course of ChT with or without immunotherapyFor CPS ≥10, consider dropping ChT after prolonged response or toxicity and treating with immunotherapy alone or immunotherapy + 5-fluorouracil (5-FU)
For ESCC, the recommended ChT regimen is 5-FU + cisplatin/oxaliplatin. For EAC, the recommended regimens are FOLFOX/CAPOX, a fluoropyrimidine (5-FU or capecitabine) + oxaliplatin, or FLOT (rarely used for unresectable disease). For GC, a fluoropyrimidine and a platinum agent (oxaliplatin or cisplatin) are recommended.
The addition of immunotherapy to a ChT backbone benefits many patients. Generally, patients with CPS scores ≥10 should receive ChT with immunotherapy, whereas patients with CPS scores <1 (i.e., minimal PD-L1 expression) should receive ChT alone. For intermediate scores, consider combining ChT with pembrolizumab or nivolumab. Pembrolizumab yields the best results with CPS ≥10, whereas nivolumab yields the best results with TPS ≥1% (64, 65). For HER2-positive disease and CPS scores ≥1, trastuzumab should be added.
The benefit of immunotherapy for eso-gastric ACs has been demonstrated in several trials. CheckMate 649 identified better progression-free survival (PFS) and OS with nivolumab + ChT compared with placebo + ChT, among patients with EAC, GEJC, or GC (66). The benefit was greatest among patients with CPS ≥5 (66). Pembrolizumab + ChT led to improved survival among patients with GC/GEJC in KEYNOTE-859; individuals with CPS ≥10 experienced the greatest benefit (64). In KEYNOTE-811, which included patients with advanced or metastatic HER2-positive G/GEJ AC, pembrolizumab added to trastuzumab and ChT improved survival among individuals with CPS ≥1 (67).
For patients with advanced or metastatic MSI-H/dMMR EAC or G/GEJ AC, pembrolizumab or nivolumab should be used since these tumors are very sensitive to immunotherapy (4). The use of doublet immunotherapy, or combinations of immunotherapy and ChT, is still debated in this small patient population.
Immunotherapy with ChT is also beneficial for ESCC. In KEYNOTE-590, with a majority of ESCC patients, individuals who received pembrolizumab + ChT had a longer mOS than those who received ChT alone (68). Similarly, in CheckMate 648, an improved mOS was demonstrated with nivolumab + ChT vs placebo + ChT, with the greatest benefit in individuals with TPS ≥1% (65, 69). Other agents, such as camrelizumab, toripalimab, and sintilimab, have also demonstrated survival improvements (70–72). At present, these agents are not available in Canada.
According to a meta-analysis of randomized controlled trials, immunotherapy improves health-related quality of life (HRQoL) relative to ChT among individuals with advanced eso-gastric cancer (5). Immunotherapy is also associated with better control of pain and dysphagia than ChT alone; these findings were attributed to lower levels of inflammation and cytotoxic effects (5).
Nivolumab + ChT is Health Canada indicated for HER2-negative advanced/metastatic GC, GEJC, and esophageal AC, regardless of PD-L1; and for unresectable or metastatic ESCC with tumor cell PD-L1 expression ≥1% (52). Nivolumab + ipilimumab is also indicated for unresectable or metastatic ESCC with PD-L1 expression ≥1% (52), but is not available in Canada. Pembrolizumab + ChT is indicated for HER2-negative unresectable/metastatic EC (regardless of PD-L1 or histology), for HER2-negative unresectable/metastatic G/GEJ AC, regardless of PD-L1; and for HER2-positive, unresectable/metastatic G/GEJ AC with CPS ≥1, with trastuzumab (73).
Immunotherapy offers significant benefits, but access is province dependent. Clinicians are encouraged to connect patients with support services, financial navigation, and access programs (74).
Survivorship issues
3.2.6
Nutrition
3.2.6.1
All patients with upper GI cancer should undergo nutrition assessments starting early in the disease course. We recommend involving a dietitian to address challenges such as weight loss, protein deficiency, and aspiration. EC and GC are associated with malnutrition, which negatively affects treatment outcomes and QoL (21, 75–78). Individuals who are at moderate to high risk of malnutrition are almost five times more likely to experience postoperative complications compared with those who are not at risk (78). In a study of individuals with ESCC treated at Princess Margaret Cancer Centre, 58% were malnourished, and these individuals had poor survival (75). Similar trends have been identified in GC (76, 77). In particular, iron deficiency, vitamin B_12_ deficiency, and dumping syndrome are common in gastrectomy patients (79).
The use of validated screening tools has been linked to reduced rates of malnutrition (80). In individuals with GC, nutrition support is associated with better outcomes after ChT and surgery (81). Enteral immunonutrition reduces the incidence of infectious complications after esophagectomy, compared with standard enteral nutrition (82). Clinicians should refer to the ESPEN guidelines (83) for the details of nutrition regimens.
Dysphagia/reflux management
3.2.6.2
We suggest discussing patient preferences for dysphagia management. Dysphagia scoring may be useful to monitor symptoms (84, 85). Management depends on the tumor length, location, and residual luminal diameter. Radiation, ChT, and/or palliative stenting may be employed, as well as a feeding tube if necessary. The decision to use radiation may depend on how much benefit the patient experiences from ChT; radiation may be delayed for later use as a salvage therapy. A thoracic surgeon or gastroenterologist should review the case for a repeat endoscopy and possible stent. Intermittent balloon dilatation is helpful for short lesions, especially in the proximal esophagus.
Psychosocial support
3.2.6.3
Patients should be referred to support groups such as My Gut Feeling (https://www.mygutfeeling.ca/) at an early stage, and clinicians should access the Canadian Association of Psychosocial Oncology (CAPO) to find practitioners with expertise in supporting cancer patients. Individuals with upper GI cancer have high levels of stress, anxiety, and depression (86). Psychosocial support should be offered throughout the disease course (86–88). Governments and organizations such as the Canadian Cancer Society, BC Cancer, Alberta Health Services, and the Government of Québec, offer support and counseling. Individuals may be very reliant on their care partner or support network; care partners also have significant psychosocial needs.
Other supports
3.2.6.4
We suggest involving palliative care early in treatment so that individuals can receive support to improve their QoL, refine their treatment goals, and access pain management. Individuals are often more accepting of targeted therapy than ChT, but delaying ChT may render them ineligible for further treatment. Clinicians should ensure that the patient and care partner understand the implications of each option. An end-of-life discussion should be held to clarify the level of care and prognosis. Early palliative care is associated with a lower rate of ED visits and hospitalizations in the last month of life (89, 90).
Discussion
4
It is well established that the addition of immunotherapy to ChT is beneficial for patients with advanced or metastatic disease. The place of immunotherapy in neoadjuvant and perioperative approaches is still being investigated; nonetheless, there is a clear benefit of adjuvant therapy for patients with EC/GEJC who have residual disease after chemoradiation and surgery. Therefore, we recommend incorporating immunotherapy into treatment strategies where appropriate. It is essential to assess patient and care partner goals for treatment on an ongoing basis.
Ongoing trials such as DESTINY-Gastric03 (trastuzumab deruxtecan in HER2-positive GC) and SKYSCRAPER-07 (tiragolumab + atezolizumab in ESCC) will provide further insights as to the roles of targeted agents and immunotherapy (91, 92). Recent studies using zolbetuximab, an antibody directed against claudin 18.2, showed extended OS among patients with advanced GC/GEJC (93, 94). The eventual addition of zolbetuximab to the therapeutic arsenal will provide more options, especially for low-CPS tumors. Research is also providing insights to improve supportive care, as in a trial which demonstrated improvement of cachexia through inhibition of the growth differentiation factor 15 (GDF-15) (95).
PD-L1 expression has an important role in therapy selection, although some aspects (e.g., cases with low to intermediate PD-L1 expression) remain controversial (96). Clinicians should use their judgment in applying this biomarker in the context of the patient’s history and disease course. Other biomarkers, such as DPYD, MSI/dMMR, and HER2, are also essential in individualizing therapy. Unfortunately, funding for molecular testing is not always available, and access is province dependent (97). Clinicians are encouraged to advocate for reflex testing and to offer access to clinical trials and experimental protocols.
The algorithm presented here is based on high-quality evidence and experience with the management of upper GI cancers. We envision this algorithm being used by any practitioner who manages upper GI cancers in Canada to inform clinical decisions. This algorithm aligns with recent international guidelines, and we refer clinicians to other documents for the details of later-line regimens (17, 29, 43).
Strengths and limitations
4.1
Strengths of this study include that the study addressed current areas of educational need in the field of upper GI cancer treatment, based on responses to a needs assessment survey. A novel approach was employed, consisting of asynchronous discussion of upper GI cancer cases, overseen by an expert Scientific Planning Committee of experts with diverse backgrounds. The algorithm includes perspectives provided by a patient representative. The best practices reported are based on the experiences of clinicians practicing across Canada in multiple specialties, and most best practices are supported by recent randomized controlled trials. Limitations include that some best practices may be region dependent; applicability will depend on local resources, access, and insurance.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Puhr HC Prager GW Ilhan-Mutlu A. How we treat esophageal squamous cell carcinoma. ESMO Open. (2023) 8:100789. doi: 10.1016/j.esmoop.2023.100789 36791637 PMC 9958251 · doi ↗ · pubmed ↗
- 2Dennehy C Khan AF Zaidi AH Lam VK. The evolving landscape of neoadjuvant immunotherapy in gastroesophageal cancer. Cancers (Basel). (2024) 16:286. doi: 10.3390/cancers 16020286 38254776 PMC 10814157 · doi ↗ · pubmed ↗
- 3Le DT Ott PA Korytowsky B Le H Le TK Zhang Y. Real-world treatment patterns and clinical outcomes across lines of therapy in patients with advanced/metastatic gastric or gastroesophageal junction cancer. Clin Colorectal Cancer. (2020) 19:32–8.e 3. doi: 10.1016/j.clcc.2019.09.001 31813769 · doi ↗ · pubmed ↗
- 4Dedecker H Teuwen L-A Vandamme T Domen A Prenen H. The role of immunotherapy in esophageal and gastric cancer. Clin Colorectal Cancer. (2023) 22:175–82. doi: 10.1016/j.clcc.2023.03.001 37005190 · doi ↗ · pubmed ↗
- 5Gupta K Roy AM Attwood K Nipp RD Mukherjee S. Effects of immunotherapy on quality-of-life outcomes in patients with gastroesophageal cancers: A meta-analysis of randomized controlled trials. Healthcare (Basel). (2024) 12:1496. doi: 10.3390/healthcare 12151496 39120199 PMC 11311609 · doi ↗ · pubmed ↗
- 6Narita Y Muro K. Updated immunotherapy for gastric cancer. J Clin Med. (2023) 12:2636. doi: 10.3390/jcm 12072636 37048719 PMC 10094960 · doi ↗ · pubmed ↗
- 7Kwak HV Banks KC Hung YY Alcasid NJ Susai CJ Patel A. Adjuvant immunotherapy in curative intent esophageal cancer resection patients: Real-world experience within an integrated health system. Cancers (Basel). (2023) 15:5317. doi: 10.3390/cancers 15225317 38001577 PMC 10669669 · doi ↗ · pubmed ↗
- 8Habbous S Yermakhanova O Forster K Holloway CMB Darling G. Variation in diagnosis, treatment, and outcome of esophageal cancer in a regionalized care system in Ontario, Canada. JAMA Netw Open. (2021) 4:e 2126090–e. doi: 10.1001/jamanetworkopen.2021.26090 PMC 845638334546371 · doi ↗ · pubmed ↗