Assessment of Long-Term Outcomes of Lower Limb Fractures Managed by Non-orthopaedic Specialist Surgeons in Rural Rwanda: A Pilot Feasibility Study
Lotta Velin, Alex Zhuang, Simon P Bigirimana, Andreas Wladis, Heritier Mfura, Jean-Bertrand A Hakizimana, Ellen Barrett, Cornelia Barth, Abebe Bekele, Robert Riviello, Andreas Meunier, Innocent Niyinkunda, Jules Iradakunda, Barnabas T Alayande

TL;DR
This pilot study in rural Rwanda shows that assessing long-term outcomes of lower limb fractures is feasible, revealing high disability and low quality of life among young patients.
Contribution
The study demonstrates the feasibility of long-term follow-up for lower limb fractures in a low-resource setting.
Findings
Most patients had high disability scores (mean WHODAS 80) at long-term follow-up.
Health-related quality of life was low, especially in the 'general health' domain (mean SF-36 score 30).
Fractures were common in the femur/hip and primarily caused by falls.
Abstract
Introduction Sub-Saharan Africa is disproportionately affected by injuries, and short-term morbidity and mortality are high in this context. Lower limb fractures (LLFs) are a common type of injury that can lead to severe disability with extensive negative social and economic consequences. However, little is known about the long-term outcomes of LLFs in sub-Saharan Africa. In this pilot study, we describe the feasibility of assessing epidemiological patterns of LLFs, the state of care, and long-term outcomes in rural Rwanda. Methods This study was conducted from July to December 2021. It consists of retrospective data collection from hospital charts and a cross-sectional, phone-based follow-up. Functional outcomes were assessed using the World Health Organization Disability Assessment Schedule (WHODAS; World Health Organization, Geneva, Switzerland) 2.0, and health-related quality of…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
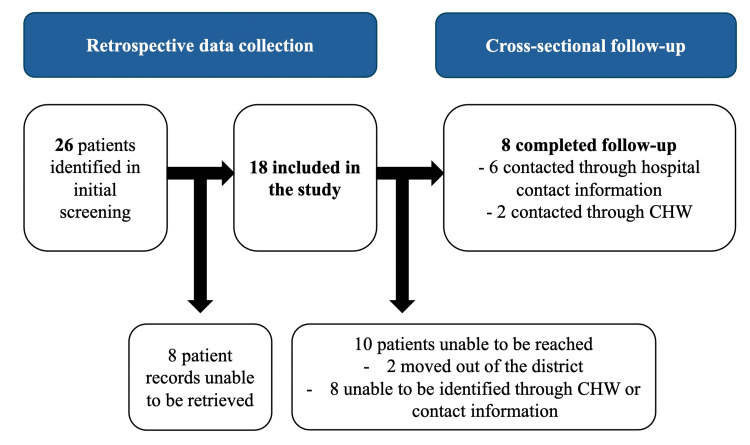 Figure 1
Figure 1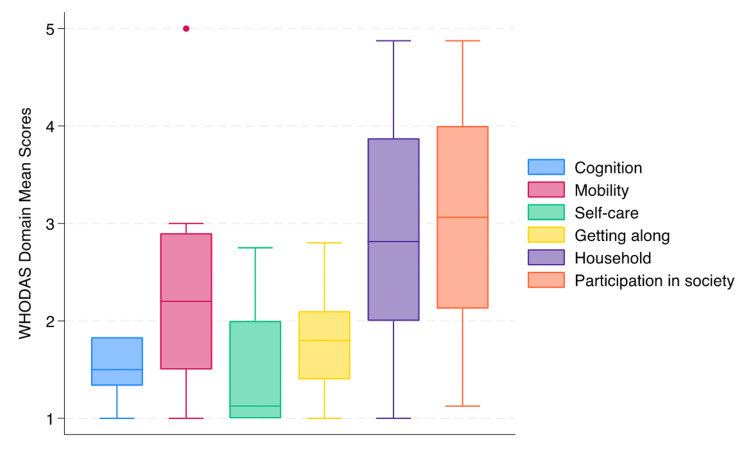 Figure 2
Figure 2| Exclusion criteria |
| No available contact information or participant not accessible using provided contact information and/or through a local community health worker. |
| Hospital admission for LLF not occurring at least 12 months preceding data collection. |
| Hospital admission occurring following major generalized trauma with LLFs existing only as a secondary diagnosis. |
| Hospital admission occurring following isolated soft-tissue injuries or joint luxation of the lower extremities. |
| Patient suffering from known comorbidities that could influence recovery or follow-up (i.e., diabetes, alcohol or substance abuse, psychiatric illness). |
| Patient does not speak English or Kinyarwanda. |
| Patient suffering from cognitive impairment affecting their ability to consent. |
| Patient has been incarcerated in the period between sustained injury and follow-up. |
| The permanent residence for the patient is outside of Rwandan borders. |
| N (%)/Median (IQR) | ||
| Age (median) | 23 (7-44) | |
| Sex | Female | 7 (39) |
| Male | 11 (61) | |
| Employment status before injury | Farmer | 6 (33) |
| Other employment | 2 (11) | |
| Not employed (age <15 years) | 7 (39) | |
| Not stated | 3 (17) | |
| Highest attained education level | High school | 2 (11) |
| Primary school | 3 (16) | |
| No schooling | 5 (26) | |
| Not stated | 9 (47) | |
| Comorbidities | Cardiovascular | 2 (11) |
| None documented | 16 (89) | |
| Type of trauma | Single fracture and no other injuries | 11 (61) |
| Multi-trauma with one fracture and other injuries | 3 (17) | |
| Multi-trauma with multiple fractures | 2 (11) | |
| Not stated | 3 (17) | |
| Trauma etiology | Fall | 10 (56) |
| Road traffic accident | 2 (11) | |
| Crush injuries | 2 (11) | |
| Violence/assault | 1 (6) | |
| Not stated | 3 (17) | |
| Main diagnosis on admission | Femur/hip fracture | 10 (56) |
| Tibial fracture | 4 (22) | |
| Pelvic fracture | 2 (11) | |
| Fibular fracture | 1 (6) | |
| Other | 1 (6) | |
| Open/closed fracture | Closed fracture | 14 (78) |
| Open fracture* | 1 (6) | |
| Unknown | 3 (17) | |
| Comminuted versus non-comminuted fracture | Comminuted | 3 (17) |
| Non-comminuted | 9 (50) | |
| Unknown | 6 (33) | |
| Waiting time to initial treatment (median number of hours) | - | 36 (24-60) |
| Treatment location/referral | Treated at BL2TH only | 5 (28) |
| Treated at BL2TH initially, then referred to other hospital for continued care | 13 (72) | |
| Treatment at BL2TH | Non-surgical treatment | 13 (72) |
| Surgical treatment (internal fixation) | 1 (6) | |
| Unknown | 4 (22) | |
| Complications | Yes (infection) | 2 (11) |
| None documented | 16 (89) | |
| Length of stay at BL2TH (median number of days) | - | 3 (1-11) |
| Planned follow-up at discharge | Yes | 10 (56) |
| No | 8 (44) | |
| Physiotherapist seen during hospital stay | Yes | 1 (6) |
| No | 17 (94) | |
| Walking aid received at discharge | Wheelchair | 1 (6) |
| Crutches | 2 (11) | |
| None/unknown | 15 (83) | |
| Readmitted | Yes (planned)** | 1 (6) |
| No | 17 (94) |
| N (%)/Median (IQR) | ||
| Age (median) | 37 (11-55) | |
| Sex | Female | 3 (38) |
| Male | 5 (63) | |
| Comorbidities | Cardiovascular | 1 (13) |
| None documented | 7 (88) | |
| Type of trauma | Single fracture and no other injuries | 7 (88) |
| Not stated | 1 (13) | |
| Trauma etiology | Fall | 5 (63) |
| Road traffic accident | 1 (13) | |
| Crush injuries | 1 (13) | |
| Not stated | 1 (13) | |
| Main diagnosis on admission | Femur/hip fracture | 6 (75) |
| Pelvic fracture | 1 (13) | |
| Fibular fracture | 1 (13) | |
| Open/closed fracture | Closed fracture | 7 (88) |
| Not stated | 1 (13) | |
| Comminuted vs non-comminuted fracture | Comminuted | 2 (25) |
| - | Non-comminuted | 4 (50) |
| - | Not stated | 2 (25) |
| Waiting time to initial treatment (median number of hours) | - | 48 (24-120) |
| Treatment location/referral | Treated at BL2TH only | 1 (13) |
| Treated at BL2TH initially, then referred to other hospital for continued care | 7 (88) | |
| Treatment at B2TLH | Non-surgical treatment | 6 (75) |
| Surgical treatment (internal fixation) | 1 (13) | |
| Not stated | 1 (13) | |
| Complications | Yes (infection) | 1 (13) |
| Not stated | 7 (88) | |
| Length of stay at BL2TH (days, median) | - | 6 (3-12) |
| Planned follow-up at discharge | Yes | 5 (63) |
| No | 3 (38) | |
| Physiotherapist seen during hospital stay | Yes | 1 (13) |
| No | 7 (88) | |
| Walking aid received at discharge | Wheelchair | 1 (13) |
| Crutches | 1 (13) | |
| None/unknown | 6 (75) | |
| Readmitted | No | 8 (100) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBone fractures and treatments · Hip and Femur Fractures · Trauma and Emergency Care Studies
Introduction
In recent years, global injury mortality has declined, yet in low- and middle-income countries (LMICs), injury remains a common cause of death and disability, with sub-Saharan Africa being particularly affected [1]. This has occurred in parallel with reductions in communicable diseases, leading to injury now being the most common cause of death for young people [1]. Although short-term morbidity and mortality from trauma in LMICs have been documented in single-center, multi-center, and global studies [1-4], long-term outcomes of both general and musculoskeletal trauma are unknown [5]. This partly results from challenges in implementing and maintaining trauma registries, including poor data quality, lack of resources, high loss-to-follow-up rates, and lack of standardized protocols for assessment of long-term trauma morbidity and mortality [6]. The long-term consequences of trauma are likely more pronounced in LMICs, as injured patients face various barriers resulting in delays in seeking, reaching, and receiving care [7-9], including frequent shortages of human and material resources [10]. These barriers also impact access to physical and occupational therapy, assistive technology, rehabilitation, timely diagnosis, and treatment of complications [4,8], essential for effective lower limb care. Moreover, low socioeconomic status itself has been associated with adverse outcomes after injury (anxiety, depression, and worse functional outcomes) [11,12], further increasing the vulnerability of patients with injury in low-resource settings. The lower limbs are a commonly injured anatomic region in Rwanda and other sub-Saharan African countries [13,14], and lower extremity injuries can lead to severe disability, with socioeconomic implications at a personal and societal level [15]. This pilot study aimed to describe the feasibility of assessing epidemiological patterns of lower limb fractures (LLFs) in a rural Rwandan hospital, the state of care for such injuries, and the effect of long-term outcomes on functioning and quality of life (QoL) after such fractures.
Materials and methods
Study design
This study consisted of a retrospective collection of injury and treatment data from hospital records and a cross-sectional phone-based follow-up with the same patients.
Defining LLFs
LLFs were defined as fractures of the hip, femur, tibia, fibula or any combination of these. We did not include soft-tissue injuries, joint luxation or subluxation.
Outcome measures* *
Functional outcomes were evaluated using the World Health Organization Disability Assessment Schedule (WHODAS; World Health Organization, Geneva, Switzerland) 2.0 (36-item version) to assess physical, social, and mental functioning after injury [6]. The 36-Item Short Form Health Survey questionnaire (SF-36) was used to assess health-related QoL. The survey tools were translated to Kinyarwanda before using. WHODAS 2.0 has been developed and used in a variety of settings [16], including a Rwandan study of functional status at a 28-day follow-up after severe injury [17], where it has demonstrated strong cross-cultural validity and feasibility in assessing post-injury function. It consists of six domains (cognition, mobility, self-care, getting along, life activities or household, and participation in society), each comprising multiple “items.” These are all built on the same question structure for assessing disability in activities, with response scales including “none,” “mild,” “moderate,” “severe,” and “extreme,” numerically represented as one to five to indicate increasing disability. Return to work was used as a proxy measure for economic repercussions. For simplicity, this was incorporated in the WHODAS 2.0 survey by adding two questions about work status before and after injury (Appendix 1). SF-36 consists of eight sub-scales: physical functioning (PF), role physical (RP), bodily pain (BP), general health (GH), vitality (VT), social functioning (SF), role emotional (RE), and mental health (MH) (Appendix 2). SF-36 [18] has also been widely used in injury research and demonstrated feasibility in sub-Saharan African settings [19,20]. *Study Location * The study was conducted at the Butaro Level Two Teaching Hospital (BL2TH), a rural hospital in Rwanda’s mountainous Northern Province. It serves as a 256-bed district hospital for Burera District and surrounding communities. The hospital has two full-time general surgeons but no orthopedic surgeon. BL2TH classifies as a bellwether-capable hospital (with capacity to perform cesarean sections or C-sections, laparotomies, and surgical management of open fractures), but the surgical caseload is heavily skewed toward C-sections and breast oncologic surgeries. As a result, most patients requiring orthopedic surgery or advanced sub-specialty surgical treatment are referred to Ruhengeri (Musanze) Referral Hospital, which is about a two-hour drive away. BL2TH was purposively chosen due to its rural location, the absence of an orthopedic surgeon, and its proximity to the University of Global Health Equity. The location was considered important since previous studies have indicated a large rural-urban gap in access to trauma care [7]. The absence of an orthopedic specialist was important for generalization to other rural district settings where general surgeons provide orthopedic care. *Study Sample * The study included all eligible patients admitted and treated for LLFs as their primary injury at BL2TH between July 1 and December 31, 2021. The exclusion criteria were defined in Table 1.
No sample size calculation was conducted, as the aim was exploratory rather than hypothesis-testing. *Data Collection * Eligible patients were identified through a retrospective chart review of paper-based records from the hospital archives. The patient identification numbers were verified in the electronic medical system, where additional data were extracted if available. All data were extracted in a pre-set questionnaire (Appendix 3). The patients were contacted at least 12 months after the injury and were invited to participate in a phone-based follow-up interview. If unable to reach the patient after three attempts, the community health worker (CHW) in the patient’s village was contacted to retrieve patient contact information. If still unavailable, the patient was considered lost to follow-up. *Ethical Considerations * This study was approved by the Rwanda National Ethics Committee (No.141RNEC/2023). Codified data were stored securely on Research Electronic Data Capture (REDCap; Vanderbilt University, Nashville, Tennessee, USA) [21]. A patient key containing their respective study codes was stored in a password-protected Excel (Microsoft Corporation, Redmond, Washington, USA) file. For phone-based follow-up data collection, participants were provided with study information in Kinyarwanda, per the Helsinki Declaration and modeled on the University of Global Health Equity information and consent form. Oral consent was obtained before the interview. *Data Analysis * Descriptive statistics (means, standard deviations or SDs, proportions, and frequencies) were used for primary and secondary endpoints (patient demographics, injury characteristics, clinical, functional, and QoL outcomes). For continuous variables, the assumption of normal distribution was tested, and median and interquartile range (IQR) were reported if the assumption failed. For WHODAS, mean polytomous item scores (where the original coding was preserved rather than dichotomized) were calculated [16], as well as overarching mean and total summary domain scores. For SF-36, a mental component summary and a physical component summary can be calculated using z-distributions based on population norms. Since no such norm scores exist in Rwanda, we only present sub-scale scores. Original sub-scale scores were converted to standardized 0-100 scores [22], with means and SDs presented across each sub-scale, where 100 indicates the highest QoL (Appendix 4). No global SF-36 score was calculated, as this is not supported in the scoring, although this is frequently reported in literature [23]. Analysis was conducted using Stata/BE 18.0 (StataCorp. 2023. Stata Statistical Software: Release 18. College Station, TX: StataCorp LLC).
Results
Demographic characteristics* *
In the initial screening of the record book at the surgical and emergency department, 26 patients were identified between July 1 and December 31, 2021. Of these, 18 matching records in the hospital archives were successfully retrieved and included in the study (Figure 1). The majority were male (n=11, 61%), young adults (mean age 29 (SD 25)), and without any previous comorbidities (n=16, 89%) (Table 2).
Visualization of the recruitment process with the inclusion and exclusion of study participants.CHW: Community health worker.
Injury characteristics
Most patients had a single fracture, although nearly one-third presented with multi-trauma (n=5, 28%). The most common injury cause was falls (n=10, 56%). Fractures were most common in the femur/hip (n=10, 56%), and most fractures were closed (n=14, 78%) and non-comminuted (n=9, 50%) (Table 2).
Treatment characteristics
The median time to initial treatment was 36 hours (IQR 24-60), and the majority were transferred to another hospital after initial treatment at BL2TH (n=13, 72%). Median length of stay at BL2TH was three days (IQR 1-11), and approximately half had planned follow-up at discharge (n=10, 56%). Only one patient (6%) had seen a physiotherapist during the stay at BL2TH, and only three received a walking aid at discharge (17%) (Table 2).
Follow-up demographics
Eight participants (44%) were followed up (Table 3), with a mean post-injury interview time being 895 days (SD 71). The follow-up sample was slightly older (median age 37, IQR 11-55) than the total study sample, but the majority were still male. Unlike the total sample, there were no participants with multi-trauma in the follow-up sample. Six were successfully contacted through the contact information in the patient records, and two were followed up through the village CHW. Of those unable to be reached, two were identified by their village CHW as having moved to a different area and, hence, were no longer reachable. The remaining eight were not recognized by their CHW and were deemed as not reachable. None declined to participate.
Disability and long-term functional outcomes
Of the eight participants with follow-up data, three (38%) were in full-time employment before injury, and five (62%) were in part-time employment. After injury, those who had been in full-time employment remained in full-time employment (n=3), whereas the others transitioned to unemployment (n=5). Two (25%) of those in full-time employment were living independently in the community, whereas the rest (n=6, 75%) resided in a form of assisted living. The total WHODAS mean summary score was 80 (SD 29) on a scale from 36 to 180, corresponding to a scale ranging from “no disability” to “full disability.” The domains with the highest mean summary scores (on a scale from one to five), indicating highest disability, were “participation in the society” (mean 3, SD 0.5), “household” (mean 3, SD 0.2), and “mobility” (mean 2, SD 0.3) (Figure 2; Appendix 5). The items with the highest mean scores were disability relating to sexual activities (item 4.5, mean 4, SD 2), emotional impact (item 6.5, mean 3, SD 1), and impact on the family (item 6.7, mean 3, SD 1).
The distribution of WHODAS domain mean scores among the participants, ranging from one to five, representing “no disability” to “extreme disability.” WHODAS: World Health Organization Disability Assessment Schedule.
The domain total summary scores were as follows: cognition (9, SD 2), mobility (23, SD 6), self-care (6, SD 3), getting along (5, SD 2), household (23, SD 11), and participation in society (24, SD 10).
Health-related QoL
The SF36 sub-scales “role limitations due to emotional health” (mean 88, SD 35) and “role limitations due to physical health” (mean 84, SD 35) had the highest health-related QoL scores, and the sub-scales “general health” (mean 30, SD 25) and “vitality” (mean 46, SD 25) had the lowest.
Discussion
This pilot study describes the feasibility of assessing the epidemiology and long-term functional outcomes of LLFs at a rural Rwandan hospital. The sample in this study indicates a different population demographic compared to the increasingly geriatric population seen in LLF studies in high-income countries [24]. In contrast with other LMIC studies of LLFs [3,25], falls, rather than road traffic accidents (RTAs), were the most common injury cause, and femur/hip fractures were the most common type of fracture, unlike previous injuries indicating the dominance of tibia/patella/fibula/ankle fractures in younger populations [26,27]. Follow-up after a minimum of one year, with a mean follow-up of 2.5 years, indicates high persisting disability, a large impact on functioning in professional capacities, household work, and social functioning, and low health-related QoL. This is especially alarming considering the low sample age. Since the follow-up sample exclusively consisted of patients with single fractures, there may additionally be a survivorship bias [28], excluding the more severely injured multi-trauma patients from the follow-up. Although research is needed at referral hospital levels to assess treatment outcomes, these study results suggest that it may be appropriate to opt for more conservative management in this setting. Surgical treatments such as open reduction and internal fixation (ORIF) are associated with risks and often require timely intervention, experienced staff, availability of adequate materials, and postoperative care, including rehabilitation. In line with this, the surgeons at B2TLH have experience and competency in ORIF procedures but prefer conservative management or refer patients for treatment due to limited time and material availability. Moreover, with load-bearing constructs such as internal fixation, patients are typically prevented from full weight bearing [29] until sufficient healing occurs, which often takes 6-12 weeks. It is uncertain whether compliance with such restrictions is feasible in a low-resource setting with limited access to rehabilitation services. LLFs and their surgical or non-surgical treatment, particularly periarticular knee fractures, are often complicated by joint stiffness. Reduced knee range of motion results in mobility limitations and impacts various gait phases and the ability to manage slopes and sit-to-stand transfers, which increases energy consumption and fatigue [30]. Reduced joint mobility may be a contributing factor to the persisting disability and reduced health-related QoL in our sample, although further studies focusing on rehabilitation are needed. The golden standard for studying functional outcomes is a physiotherapist assessment, including simple measures, feasible and relevant in the local context, such as maximum walking distance or ability to stand or jump on one leg. One tool that may be considered in future studies to assess functional outcomes is the Activity Independence Measure-Trauma, recently validated in humanitarian settings and suitable for patients with limited health literacy [31]. Access to rehabilitation services in Rwanda is severely limited, like many other LMICs [32]. The WHO Rehabilitation 2030 initiative [33] emphasizes the need for increased focus on rehabilitation, including data collection to understand service gaps and guide solutions. At B2TLH, there is one part-time physiotherapist but no standardized rehabilitation plan for injured patients, and only one patient in this sample saw a physiotherapist, indicating room for quality improvement. Previous studies indicated that even when rehabilitation services were offered, prohibitive costs and limited access to transportation made access to such services difficult for rural patients [34]. Most patients had planned follow-ups with a general practitioner in the outpatient department, who, in case of need, could refer them to higher levels of care. Globally, insufficient human resources limit rehabilitation care, prompting WHO to recommend integrating rehabilitative services into CHW systems. Although CHWs are integral to the Rwandan health system [35], their involvement in rehabilitation is yet to be implemented [32]. The major limitation of this study is the small sample size and the loss of follow-up. Several participants lacked phones and therefore provided the contact information of their partners or neighbours, complicating follow-up. The small sample is also likely a result of circumstances specific to Rwanda, such as the relatively short physical distances, which may facilitate the bypassing of district hospitals, with trauma patients often directly going to secondary hospitals with surgical capacities. Yet, the sample is comparable to a 2013 study of non-obstetric surgical patients in three Rwandan district hospitals, including B2TLH [36]. In this study, 1024 trauma patients sought care across the three hospitals over one year, with B2TLH receiving the lowest number of cases. Among these, only 41 patients (4.1%) received surgical management and were discharged from the district hospital, whereas the majority (n=573, 55.9%) received non-operative care before discharge. The low proportion of RTA patients is likely multifactorial and contrasts previous studies from urban Kigali [17]. Firstly, B2TLH is rurally located, far from major highways, with limited road access and significantly fewer motor vehicles. Most fractures result from falls from heights in this mountainous context, and such accidents are relatively few and far between. Secondly, when RTAs occur, police and/or emergency medical services (EMS) often arrive at the scene and take those requiring healthcare directly to a facility with trauma capacity (i.e., bypassing Butaro). Similarly, the proportion of open fractures may be underrepresented, assuming that severe injuries are more likely to be directly transported to other facilities. Although a large knowledge gap remains regarding injury outcomes in rural settings, future studies should consider that rural patients may bypass lower levels of care (such as health centers and district hospitals) and should therefore include secondary hospitals as study sites. The small sample further spurs questions regarding the representativeness of the study location and the sample, and the generalizability of the findings to other LMICs. Firstly, it is important to note that there is no one “typical” LMIC setting, as this umbrella term encompasses significant heterogeneity. Moreover, Rwanda’s pre-hospital EMS are considered well-developed [7], in contrast to findings from a 2013-2014 survey study that showed the absence of pre-hospital EMS in 33 (61%) of 49 African countries [37]. Previous regional studies have also reported a significant skew of EMS toward urban areas, with only 8.6% of the populations living within EMS coverage. In contrast, Rwanda has nationwide EMS coverage [38], further limiting the generalizability of the Rwandan context to other LMICs. Yet, we believe that certain elements of this study context, such as underdeveloped infrastructure, human resource limitations, and financial shortages, are common in some other LMICs. This suggests that the findings may imply some generalizability, and the lessons learned could be used and contextually adapted in such settings [14]. Another study limitation is that the survey tools have not yet been officially translated to Kinyarwanda or validated in Rwanda. We experienced some difficulties in doing the interviews; however, we perceived that the participants easily understood the questions. One survey-related challenge was that, despite stating that the study did not involve financial compensation, some participants insisted on receiving compensation, and there may be a responder bias in participants having exaggerated their long-term disability to motivate such compensation. Although challenging, we believe that important measures were taken to reduce the effects of responder bias in patient-reported outcome measures such as using validated survey tools with neutrally framed questions and having local Kinyarwanda native speakers, who did not have a healthcare-provider relationship with the participants, conduct interviews. Despite the small sample, this study provides value due to the novel context and focuses on previously unexplored functional outcomes. This pilot study indicates many possible directions for future research and considerations that may be useful when planning such studies. Over half of the patients in this cohort suffered fractures due to falls, with femur/hip fractures being the most common. This raises questions about why and how such severe injuries occur, especially in a young population. Further investigations may highlight possible community or public health interventions to reduce these injuries. Another issue that must be addressed is the median wait time of 1.5 days (36 hours) before initial treatment. One previous qualitative study identified facility overload, lack of trained personnel, medication shortages, and hospital workflow as significant contributors to care delays at Rwandan hospitals [34]. Root cause analyses and process mapping can help identify areas for improvement, as the contributing factors are likely systemic and multifactorial. Future research involving prospective cohorts with a significantly larger sample size will be needed to assess the long-term disability outcomes of trauma patients in rural settings. Randomized controlled trials that address confounders will help provide higher quality evidence.
Conclusions
This study highlights the challenges of long-term follow-up after LLFs in a rural, low-resource setting but demonstrates that such a study is feasible if planned with contextual considerations. The demographic characteristics of patients with LLFs in rural Rwanda appear to be in stark contrast to the increasingly geriatric population in high-income countries and merit further research to guide contextually relevant treatment guidelines. Self-perceived disability is high, and health-related QoL is low at long-term follow-up, which should be considered in the context of this condition primarily affecting a young, previously healthy population.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Global injury morbidity and mortality from 1990 to 2017: results from the Global Burden of Disease Study 2017 Inj Prev James SL Castle CD Dingels ZV 011426202010.1136/injuryprev-2019-043494 PMC 757136632332142 · doi ↗ · pubmed ↗
- 224 h mortality and its predictors among road traffic accident victims in a resource limited setting; a multicenter cohort study BMC Surg Kamabu K La O Soria J Tumwesigye D 972320233710120710.1186/s 12893-023-02011-9PMC 10131391 · doi ↗ · pubmed ↗
- 3Epidemiology of injuries and outcomes among trauma patients receiving prehospital care at a tertiary teaching hospital in Kigali, Rwanda Afr J Emerg Med Mbanjumucyo G George N Kearney A 191197620163045609410.1016/j.afjem.2016.10.001PMC 6234177 · doi ↗ · pubmed ↗
- 4Trauma mortality patterns in three nations at different economic levels: implications for global trauma system development J Trauma Mock CN Jurkovich GJ nii-Amon-Kotei D 804812441998 https://journals.lww.com/jtrauma/abstract/1998/05000/trauma_mortality_patterns_in_three_nations_at.11.aspx 960308110.1097/00005373-199805000-00011 · doi ↗ · pubmed ↗
- 5Current status of musculoskeletal trauma care systems worldwide J Orthop Trauma Miclau T Hoogervorst P Shearer DW 07032 Suppl 7201810.1097/BOT.000000000000130130247404 · doi ↗ · pubmed ↗
- 6Trauma registry implementation in low- and middle-income countries: challenges and opportunities J Surg Res Bommakanti K Feldhaus I Motwani G Dicker RA Juillard C 728622320182943388810.1016/j.jss.2017.09.039 · doi ↗ · pubmed ↗
- 7Disparities in access to trauma care in Sub-Saharan Africa: a narrative review Curr Trauma Rep Alayande B Chu KM Jumbam DT 6694820223569250710.1007/s 40719-022-00229-1PMC 9168359 · doi ↗ · pubmed ↗
- 8Identifying, prioritizing and visually mapping barriers to injury care in Rwanda: a multi-disciplinary stakeholder exercise World J Surg Odland ML Whitaker J Nepogodiev D 290329184420203244095010.1007/s 00268-020-05571-6PMC 7385009 · doi ↗ · pubmed ↗