Failure of timely removal of central and peripheral venous catheters after antibiotic therapy in nursing homes
Amarah Mauricio, Joshua B. Hsi, Tom Tjoa, Raveena D. Singh, Shereen Nourollahi, Raheeb Saavedra, Bardia Bahadori, Mohamad N. Alsharif, Steven Tam, Justin Chang, Syma Rashid, Shruti K. Gohil

TL;DR
Many nursing home residents keep venous catheters after finishing antibiotics, increasing safety risks.
Contribution
The study reveals a high rate of unnecessary catheter retention in nursing homes.
Findings
80% of catheters were retained after antibiotic therapy ended.
One-third of catheters were retained for over a week.
Abstract
Each day a venous catheter is retained poses unnecessary safety risks. In a retrospective evaluation of central/peripheral lines in nursing home residents receiving antibiotics, 80% were retained beyond antibiotic treatment end and nearly one third were retained longer than a week. Interventions for timely catheter removal are urgently needed.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
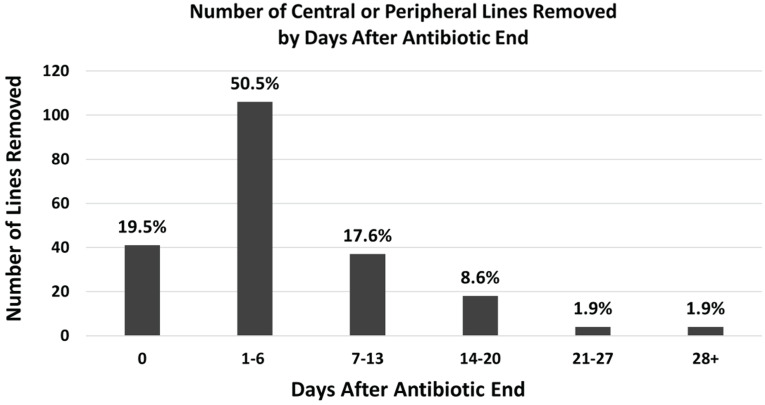 Figure 1
Figure 1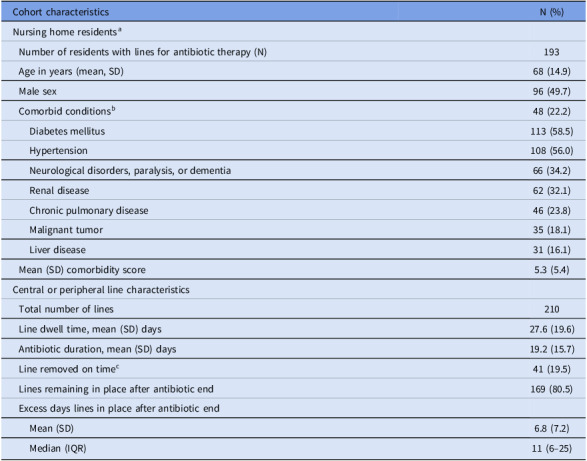 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCentral Venous Catheters and Hemodialysis · Urinary Tract Infections Management · Nosocomial Infections in ICU
Background
Each year in the United States, 2.7 million peripherally inserted central catheters (PICCs) are placed,^ 1 ^ a large proportion of which are managed postdischarge for antibiotic therapy. Continuation of intravenous antibiotic therapy is a common reason for nursing home placement.^ 2 ^ Completion of antibiotic therapy should signal line removal and ideally occur on the same day therapy is concluded in a nursing home. We sought to evaluate the extent to which central venous catheters that had exceeded their designated usage were promptly removed in nursing homes.
Methods
We conducted a retrospective analysis of the SAFER Lines nursing home study.^ 3 ^ In brief, this study involved an evaluation of central and peripheral catheter insertion sites and dressings in six nursing homes in Orange County, California, from September 2015 to December 2018. During the latter half of that study (January 2017–December 2018), efforts were made to train on evaluation of insertion sites and to ensure proper dressing changes, but timely catheter removal was not addressed. We identified the subset of the SAFER Lines cohort whose indication for a venous catheter was antibiotic therapy and whose antibiotic end date was known.
For each member of the antibiotic cohort, we collected the following information: nursing home of residence, age, sex, admission date, discharge date (if applicable), prescribed antibiotics, intravenous antibiotic start and end dates, and date of catheter removal. Comorbidities were defined using Elixhauser Comorbidity Conditions based on ICD-10-CM as available in Centers for Medicare and Medicaid Minimum Dataset; state hospitalization data were used to identify infection-related hospitalization and emergency department visits.^ 4,5 ^
Residents with a catheter removal date ≥ 1 calendar days after conclusion of intravenous antibiotics were considered to have a catheter that was not removed on time. Time (days) from intravenous antibiotic completion to catheter removal was calculated. Number of catheters removed were categorized by number of days in place beyond antibiotic end and graphically displayed. Catheters without an available removal date were not included in calculations for catheter insertion time after antibiotics were stopped. Analyses were performed using SAS version 9.4 software (SAS Institute, Cary, NC).
Results
The overall SAFER Lines cohort included 720 residents in six nursing homes. Of these, 193 residents from five nursing homes had 210 had venous catheter access for the sole purpose of intravenous antibiotic therapy with clearly documented completion dates during the study. Of these, 185 (88.1%) were central lines (177 PICCs, 5 subclavian, 2 internal jugular, and 1 femoral) and 25 were midlines. Catheters with missing antibiotic end dates were excluded (n = 22).
Table 1 summarizes nursing home resident and catheter characteristics. Mean (SD) age was 58 (17), 96 (49.7) were male, and mean (SD) comorbidity score was 5.3 (5.4). Among 210 catheters, mean (SD) dwell time was 27.6 (19.6) days and duration of antibiotic treatment was 19.2 (15.7) days. Antibiotic indication was documented for 54 (25.7%) catheters and included skin/soft tissue infection (n = 17, 31.5%), osteomyelitis (n = 16, 29.6%), urinary tract infection (n = 8, 14.8%), pneumonia (n = 7, 13.0%), and the remainder a mixture of other indications (n = 8, 14.8%). Timely removal on the day of antibiotic end occurred for 41 (19.5%) catheters. Of the remaining 169 (80.5%) lines that had late removal,106 (50.5%) were left in place for up to one week and 30% (63/210) remained in place longer than a week, with several lines in place up to one month without documented indication (Figure 1). Mean (SD) excess dwell time across the cohort was 6.8 (7.2) days (Table 1), ranging from 5.2 (6.7) to 8.6 (9.1) days across the five nursing homes. Among the 169 catheters with late removal, 59 (34.9%) had an infection-related hospitalization or emergency department visit of which 36 (61.0%) were in place ≥7 days of antibiotic end.
Table 1.Characteristics of nursing home residents with central and peripheral lines receiving intravenous antibioticsCohort characteristicsN (%)Nursing home residents^ a ^ Number of residents with lines for antibiotic therapy (N)193 Age in years (mean, SD)68 (14.9) Male sex96 (49.7) Comorbid conditions^ b ^ 48 (22.2) Diabetes mellitus113 (58.5) Hypertension108 (56.0) Neurological disorders, paralysis, or dementia66 (34.2) Renal disease62 (32.1) Chronic pulmonary disease46 (23.8) Malignant tumor35 (18.1) Liver disease31 (16.1) Mean (SD) comorbidity score5.3 (5.4)Central or peripheral line characteristics Total number of lines210 Line dwell time, mean (SD) days27.6 (19.6) Antibiotic duration, mean (SD) days19.2 (15.7) Line removed on time^ c ^ 41 (19.5) Lines remaining in place after antibiotic end169 (80.5) Excess days lines in place after antibiotic end Mean (SD)6.8 (7.2) Median (IQR)11 (6–25) a Patients with peripherally inserted central catheter (PICC) line in place in whom indication for a central line was antibiotic therapy and whose antibiotic end date was known. b Elixhauser Comorbidity Conditions based on ICD-10-CM. (n.d.). https://hcup-us.ahrq.gov/toolssoftware/comorbidityicd10/comorbidity_icd10.jsp. c Removed on the day that antibiotic treatment ended.
Figure 1.Number of central or peripheral lines removed by days after antibiotic completion. Number of central (n = 185) and peripheral (n = 25) lines removed, categorized by days after antibiotic end date. Percentages calculated among total 210 venous catheters.
Discussion
In this study, 80% of nursing homes residents who required central or peripheral venous catheters for intravenous antibiotics did not have their catheters removed on the calendar day antibiotics concluded, with nearly one-third of residents not having it removed until a week or more after antibiotics concluded. Across all residents, failure to remove these venous catheters resulted in an average of 6.8 days of excess dwell time. Each day a catheter is retained without a clear indication for its use poses unnecessary risks for residents, including thrombotic complications, local infection, and central line associated bloodstream infections.^ 6 ^
Nursing homes provide complex medical care but often lack the necessary staffing or resources to maintain proactive infection prevention processes.^ 4 ^ Resources should be allocated to encourage daily monitoring of line necessity to ensure prompt removal of catheters.^ 7 ^ Unfortunately, high-fidelity mechanisms that ensure on-time catheter removal have yet to be implemented in most nursing homes.^ 8 ^ The absence of such processes warrants concerted efforts to provide staff training and to set standards of practice to ensure that catheter removal is scheduled when intravenous therapy is discontinued. Although physicians are generally present in nursing homes only once or twice per week, scheduled antibiotic administration and known stop days should allow timely removal of catheters by nurses who are present at all shifts even when physicians may not be on-site.^ 9 ^
Timely catheter removal should be included in structured training of nurses and physicians related to catheter placement, maintenance, and discontinuation. With increasing use of electronic medical records in nursing homes, it is possible to implement electronic prompts tied to an antibiotic order which could prespecify the end date of intravenous therapy.^ 10 ^ This would tether catheter removal to the completion of therapy and ensure accountability among care staff.
This study has several limitations. The sample size is limited to five nursing homes in a single geographic region which may limit generalizability. In addition, this study was retrospective and reasons for delayed removal were not assessed. Similarly, any harm from delayed removal was not collected or quantified.
In summary, central and peripheral venous catheters used for antibiotic therapy in nursing homes are more often than not overdue for removal. Protocols are urgently needed to ensure that removal dates are linked to antibiotic completion dates to reduce the risk of thrombotic and infectious complications.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1i Data Research. Over 2.7 million PICC line insertion procedures are performed each year in the United States. https://idataresearch.com/over-2-7-million-picc-line-insertion-procedures-are-performed-each-year-in-the-us/. Published 2020. Accessed March 20, 2024.
- 2Thompson ND , Stone ND , Brown CJ , et al. Antimicrobial use in a cohort of US nursing homes, 2017. JAMA 2021;325:1286–1295.33821897 10.1001/jama.2021.2900 PMC 8025112 · doi ↗ · pubmed ↗
- 3Gohil SK , Bahadori B , Nourollahi S , et al. 1668. The SAFER lines project: a mobile-app strategy for prevention of outpatient central line associated bloodstream infection (CLABSI). Open Forum Infect Dis 2022;9:ofac 492.134.
- 4Centers for Medicare & Medicaid Services Minimum Data Set (MDS). 3.0 for Nursing Homes and Swing Bed Providers. https://www.cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-Instruments/Nursing Home Quality Inits/NHQIMDS 30. Published 2024. Accessed March 1, 2023.
- 5Agency for Healthcare Research and Quality. Elixhauser Comorbidity Software Refined for ICD-10-CM. https://hcup-us.ahrq.gov/toolssoftware/comorbidityicd 10/comorbidity_icd 10.jsp. Published n.d. Accessed July 6, 2024.
- 6Agency for Healthcare Research and Quality. Toolkit for Using the AHRQ Quality Indicators: Selected Best Practices and Suggestions for Improvement. Central Venous Catheter Related Bloodstream Infections. https://www.ahrq.gov/sites/default/files/wysiwyg/professionals/systems/hospital/qitoolkit/combined/d 4d_combo_psi 07-crbsi-bestpractices.pdf. Published 2016. Accessed July 15, 2024.
- 7Nguyen KP , Singh RD , Saavedra R , et al. Central-line team effort: recognizing insertion-site concerns in nursing homes. Infect Control Hosp Epidemiol 2023;44:1887–1889.37539731 10.1017/ice.2023.165PMC 10665860 · doi ↗ · pubmed ↗
- 8Smith PW , Bennett G , Bradley S , et al. SHEA/APIC guideline: infection prevention and control in the long-term care facility, July 2008. Infect Control Hosp Epidemiol 2008;29:785–814.18767983 10.1086/592416 PMC 3319407 · doi ↗ · pubmed ↗