Bilateral Idiopathic Sclerochoroidal Calcification: A Case Report
Boutayna Azarkan, Hamza Lazaar, Zineb Hilali, Noureddine Boutimzine, Lalla Ouafa Cherkaoui

TL;DR
This case report describes an elderly patient with bilateral eye calcifications found during a routine eye exam, with no symptoms or need for treatment.
Contribution
The novelty lies in presenting a rare case of bilateral idiopathic sclerochoroidal calcification confirmed through detailed clinical and imaging evaluation.
Findings
Bilateral sclerochoroidal calcification was identified in an 80-year-old patient with no history of high myopia or uveitis.
Systemic evaluations ruled out secondary causes like hyperparathyroidism or chronic renal disease.
The condition remained asymptomatic and did not require treatment, highlighting its benign nature.
Abstract
Sclerochoroidal calcification (SCC) is a rare and often asymptomatic condition characterized by the deposition of calcium pyrophosphate in the sclera and choroid. It predominantly affects elderly individuals of Caucasian descent and is most often idiopathic, although it can be secondary to systemic disorders such as hyperparathyroidism or chronic renal disease. The lesions appear as irregular, white-yellow plaques located in the mid-periphery, typically along the vascular arcades. We present the case of an 80-year-old patient with bilateral idiopathic SCC, incidentally discovered during an ophthalmologic examination. The patient’s medical history included diabetes, hypertension, and cataract surgery, and there was no history of high myopia or uveitis. Fundus examination revealed yellowish choroidal lesions bilaterally, confirmed by autofluorescence and optical coherence tomography (OCT)…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
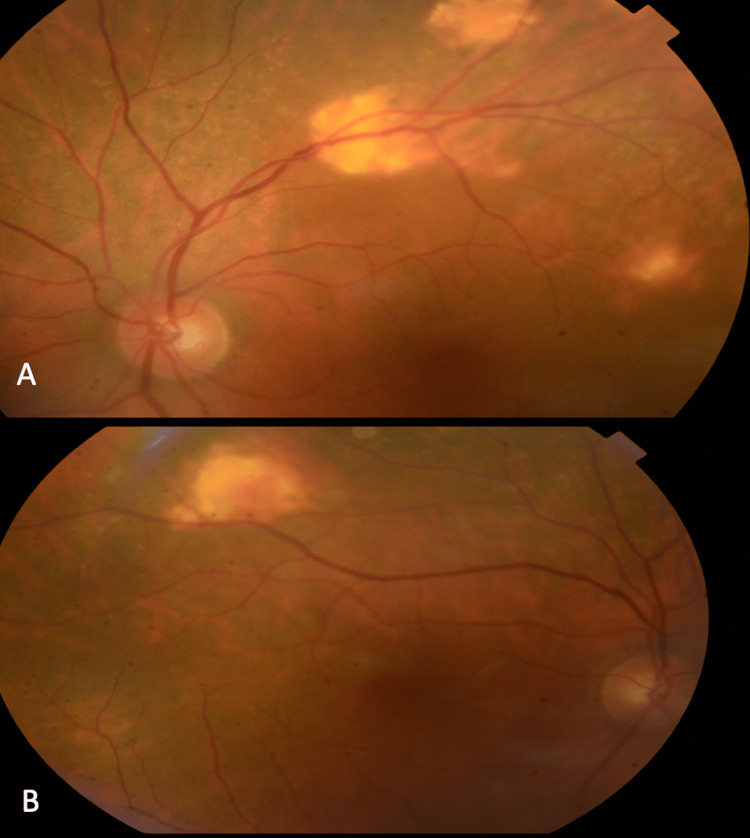 Figure 1
Figure 1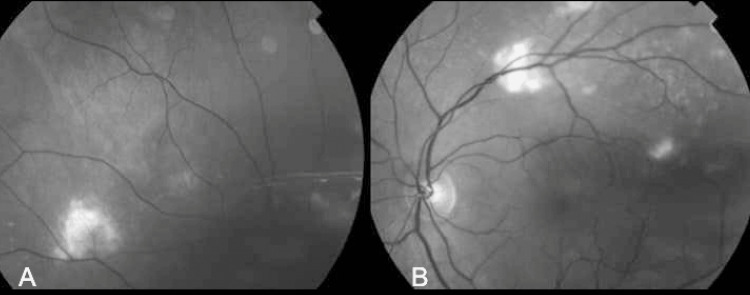 Figure 2
Figure 2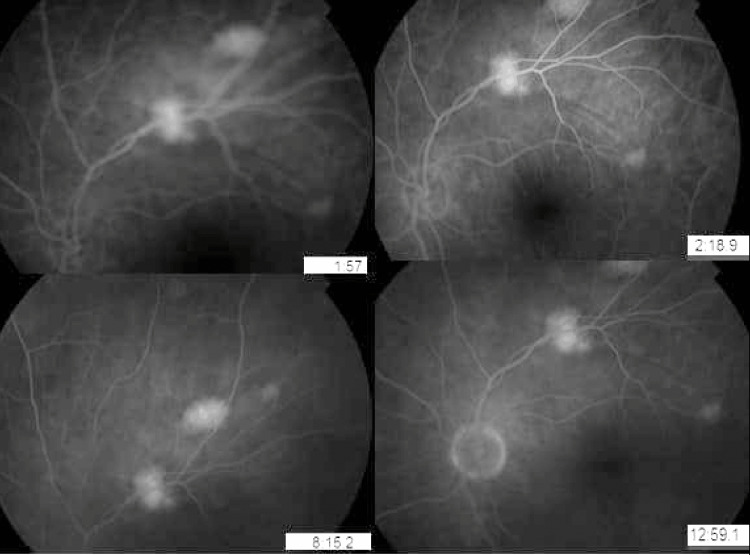 Figure 3
Figure 3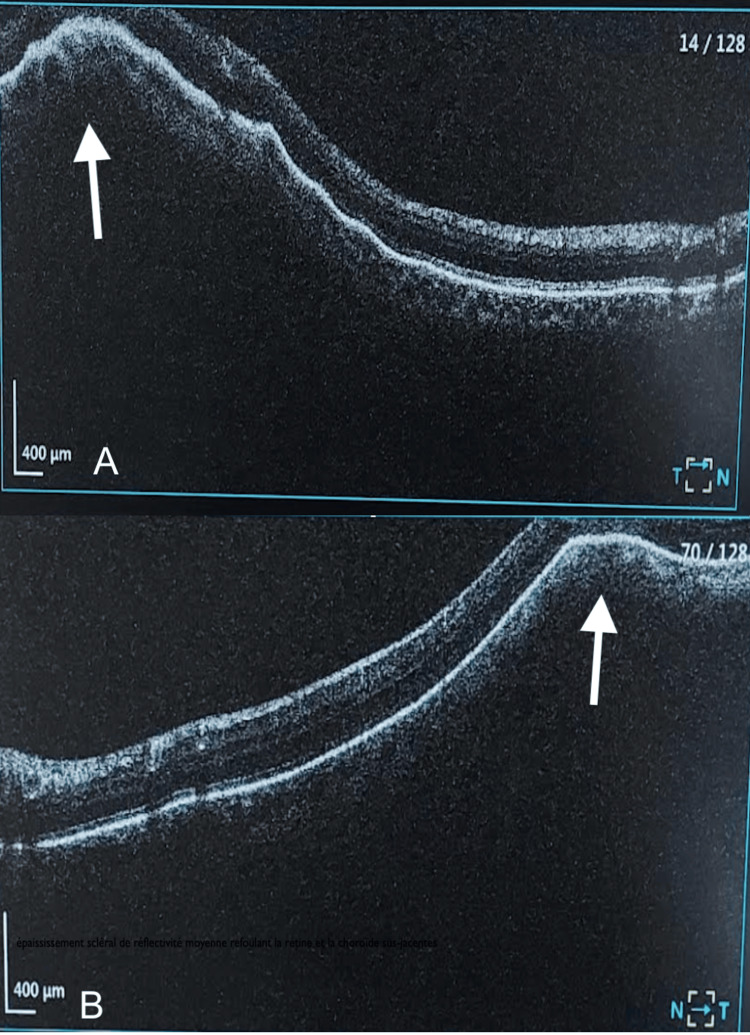 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDermatological and Skeletal Disorders · Medical Imaging and Pathology Studies · Bone health and treatments
Introduction
Sclerochoroidal calcification (SCC) is a rare and idiopathic pathology characterized by the deposition of calcium pyrophosphate within the sclera and choroid. It manifests as irregular, white-yellow plaques of varying sizes, located predominantly in the superotemporal mid-periphery along the vascular arcades [1]. This condition primarily affects elderly individuals of Caucasian descent, with no gender predilection [2]. Though most often idiopathic, it may, however, be secondary to disorders of hydro-electrolytic metabolism and other renal tubulopathies [3,4]. Given the nature of the diagnosis as one of exclusion, differential diagnoses, including choroidal osteomas, melanoma metastases, achromic lymphomas, Angoid streaks, and infective chorioretinitis, must first be ruled out [5].
We report a rare case of an 80-year-old patient presenting with bilateral idiopathic SCC.
Case presentation
We report the case of an 80-year-old patient with a history of diabetes, hypertension, and previous cataract surgery of the left eye by phacoemulsification who presented for consultation due to complaints of floaters. The anterior segment examination revealed a best-corrected visual acuity of 4/10 on the Snellen scale in the right eye and 9/10 in the left eye. The patient has no important refractive error. An intraocular pressure (IOP) of 15 mmHg, a calm anterior chamber with good depth, normal iris and stromal appearance, and no retrocorneal precipitates were observed. The intraocular lens was clear in the left eye, and a grade II nuclear cataract was present in the right eye. Fundus examination revealed multiple yellowish choroidal lesions bilaterally (incidentally discovered) located at the superior temporal arcades with a good macular reflection, well-defined vessels, and without vascular sheathing in both eyes. They were better visualized in the left eye (Figure 1).
Fundus examination of the left (image A) and right eyes (image B) showing multiple sclerochoroidal calcifications
The green-light fundus photograph reveals irregular whitish lesions near the vascular arcades (Figure 2).
Green-light retinography of the right (image A) and left (image B) eyes showing the sclerochoroidal calcifications
The autofluorescence image demonstrated hyperautofluorescent lesions with early-stage hyperfluorescence without diffusion in angiography (Figure 3).
Angiography of the left eye showing hyperfluorescent lesions at early stage without diffusion
Optical coherence tomography (OCT) centered on the lesion showed a normal retina and retinal pigment epithelium, but elevated due to the sclerochoroidal lesion (Figure 4).
OCT centered on the right (image A) and left eyes (image B) showed a normal retina and retinal pigment epithelium, but elevated due to the sclerochoroidal lesion.OCT, optical coherence tomography.
A full biological workup was performed, confirming the idiopathic nature of these SCCs, in line with the majority of reported cases in the literature. Serologies for hepatitis B and C, HIV, anti-nuclear antibodies, complete blood count (CBC), and C-reactive protein (CRP) were normal; renal function tests, parathyroid hormone (PTH), T4, and serum protein electrophoresis (SPE) were within normal limits. After excluding any systemic pathology, no treatment was required. Prognosis is generally excellent.
Upon six-month follow-up, the examination and OCT imaging results remained unchanged.
Discussion
SCC is a rare benign intraocular lesion primarily found in elderly individuals, almost exclusively described in Caucasian patients [2]. It is idiopathic in 79% of cases and secondary in 21% [2]. It is bilateral in 52% of cases with no gender predilection [2]. The condition is most often incidentally discovered due to its typically asymptomatic nature [6]. It manifests as single or multiple irregularly bordered lesions of varying sizes, flat or slightly elevated, white-yellow in color, most commonly located in the superior temporal region, and less frequently in the superior nasal area, along the retinal vascular arcades in the mid-periphery between the equator and arcades. It can, more rarely, be found in the macular area, potentially leading to decreased visual acuity, exudation, and the formation of choroidal neovascularization [7].
Differential diagnoses primarily include choroidal melanoma, osteoma, and metastatic choroidal lesions.
Choroidal metastases are typically larger, well-defined, and often accompanied by serous retinal detachment, preferentially localized at the posterior pole [8].
Osteomas commonly appear as yellowish to orange, slightly elevated subretinal lesions with well-defined geographic margins and are most often solitary, located in the juxtapapillary or peripapillary region [9].
Choroidal melanoma is usually pigmented but can vary in pigmentation, even being amelanotic (non-pigmented). Characteristic findings include orange pigment (lipofuscin) at the retinal pigment epithelium level, exudative retinal detachment, and absence of calcium on imaging [10].
A study conducted at the Oncology Department of Wills Eye Hospital revealed that SCC lesions were often misdiagnosed as choroidal metastases (26%), choroidal melanoma (21%), choroidal nevus (11%), or an unidentified tumor (39%) [11].
SCC can be subdivided into three pathophysiological entities: idiopathic, dystrophic, and metastatic. In dystrophic calcifications, calcium crystal deposition most often occurs on necrotic or damaged tissues, or in the context of chronic inflammation, with normal phosphocalcic balance. This corresponds to band keratopathy in the cornea or optic disk drusen at the papilla [11].
In metastatic calcifications, calcium crystal deposition is secondary to a disorder in phosphocalcic metabolism seen in several pathologies. Primary hyperparathyroidism is the most common condition associated with SCC, due to hypersecretion of PTH, which leads to elevated serum calcium levels [12]. Secondary hyperparathyroidism has also been described in SCC due to chronic renal failure [12]. SCC has been reported in cases of vitamin D-related disorders, such as sarcoidosis producing 1,25-dihydroxy-cholecalciferol and vitamin D intoxication from excessive intake of vitamin D [13], and more rarely in hypovitaminosis [14].
Bartter syndrome and Gitelman syndrome, uncommon tubular metabolic alkalosis syndromes, are linked to SCCs. These autosomal recessive renal tubular diseases impair sodium and chloride transport [15].
Although often idiopathic, a thorough systemic evaluation is crucial to rule out dystrophic or metastatic calcifications due to underlying pathological conditions associated with disturbances in calcium-phosphorus metabolism [16].
A classification of SCC based on OCT imaging has been proposed by Hasanreisoglu et al. [17], categorizing SCCs into four patterns based on scleral contours: flat, rolling, rocky-rolling, and table mountain.
The management of SCC is primarily conservative, focusing on addressing any underlying conditions. In cases of choroidal neovascularization, a rare complication of SCC, anti-VEGF (vascular endothelial growth factor) injections and photodynamic therapy have shown efficacy [18].
Conclusions
SCC should be considered as a differential diagnosis when examining patients with elevated fundus lesions. Fundoscopic clinical appearance should be compared to systemic review to determine if further workup is required. At minimum, patients with newly presenting SCC lesions should be referred for physical and complete blood work, including calcium and parathyroid function. Any systemic anomalies should be thoroughly vetted and correlated with both systemic and fundoscopic clinical findings. Consultation with endocrinology for high-risk cases is advised for the best continuity of care.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Idiopathic sclerochoroidal calcification Br J Ophthalmol Cooke CA Mc Avoy C Best R 2452468720031254376410.1136/bjo.87.2.245PMC 1771522 · doi ↗ · pubmed ↗
- 2Sclerochoroidal calcification: Clinical features, outcomes, and relationship with hypercalcemia and parathyroid adenoma in 179 eyes Retina Shields CL Hasanreisoglu M Saktanasate J Shields PW Seibel I Shields JA 5475543520152557478810.1097/IAE.0000000000000450 · doi ↗ · pubmed ↗
- 3Choroidal calcification in Bartter syndrome Am J Ophthalmol Marchini G Tosi R Parolini B Castagna G Zarbin M 7277291261998982224210.1016/s 0002-9394(98)00126-3 · doi ↗ · pubmed ↗
- 4Sclerochoroidal calcification associated with Gitelman syndrome Am J Ophthalmol Bourcier T Blain P Massin P Grünfeld JP Gaudric A 76776812819991061252010.1016/s 0002-9394(99)00277-9 · doi ↗ · pubmed ↗
- 5Idiopathic sclerochoroidal calcification Ophthalmology Sivalingam A Shields CL Shields JA Mc Namara JA Jampol LM Wood WJ Daubert G 720724981991206250710.1016/s 0161-6420(91)32228-0 · doi ↗ · pubmed ↗
- 6Sclerochoroidal calcification is primarily a scleral condition based on enhanced depth imaging optical coherence tomography JAMA Ophthalmol Fung AT Arias JD Shields CL Shields JA 96096313120132401540210.1001/jamaophthalmol.2013.67 · doi ↗ · pubmed ↗
- 7Multimodal imaging of choroidal neovascularization associated with sclerochoroidal calcification Ocul Oncol Pathol Bessette AP Singh AD 234238220162784390210.1159/000446214 PMC 5091282 · doi ↗ · pubmed ↗
- 8Choroidal metastases: Origin, features, and therapy Indian J Ophthalmol Arepalli S Kaliki S Shields CL 1221276320152582754210.4103/0301-4738.154380 PMC 4399120 · doi ↗ · pubmed ↗