Cholecystoenteric Fistula: A Single-Center Experience of Seven Cases with Unusual Complications of Gallstone Disease
Karamveer Singh, Nayana S Kumar, Manoj Joshua Lokavarapu, Satish Ammapalem, Monisha Selvarasu, Amit Gupta

TL;DR
This study examines seven cases of cholecystoenteric fistulas, a rare complication of gallstone disease, focusing on surgical management and outcomes at a single center.
Contribution
The paper provides insights into the surgical challenges and outcomes of a rare condition with a small, single-center cohort.
Findings
Cholecystoenteric fistulas were often diagnosed intraoperatively due to nonspecific symptoms.
Laparoscopic surgery was attempted in 57.14% of cases but required conversion to open surgery in some.
Postoperative complications included surgical site infections and one death.
Abstract
Background: Cholecystoenteric fistulas (CEFs) are rare complications of chronic calculous cholecystitis, often diagnosed intraoperatively due to their nonspecific clinical presentation and challenges in preoperative detection. This study analyzes the surgical management and outcomes of CEFs at a tertiary care center. Methods: A retrospective analysis was conducted on all patients who underwent surgery for CEF in the hepatopancreaticobiliary unit of the Department of Surgery at the All India Institute of Medical Sciences, Rishikesh, India, between June and December 2024. Data on preoperative characteristics, biochemical parameters, intraoperative findings, surgical techniques, conversion rates, and postoperative outcomes were collected and analyzed. Results: Seven patients were included, with a mean age of 55.6 years (range: 49-69 years). Abdominal pain was the most common symptom…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
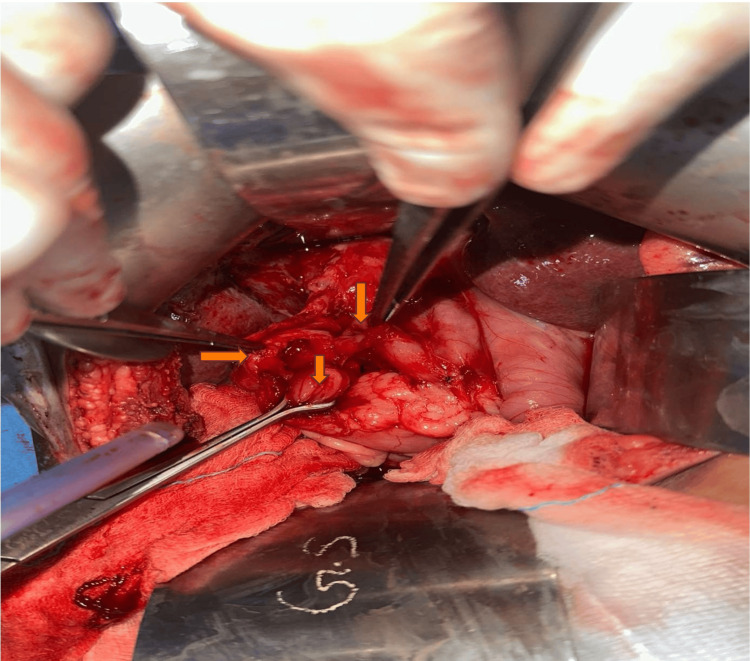 Figure 1
Figure 1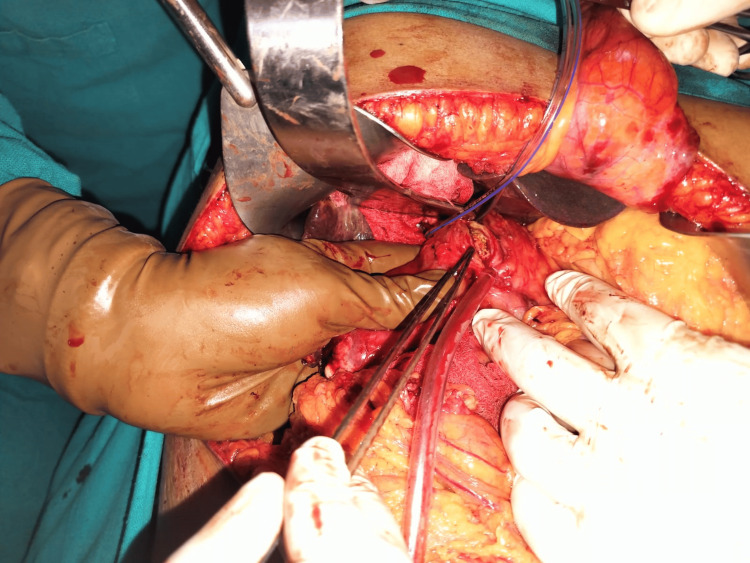 Figure 2
Figure 2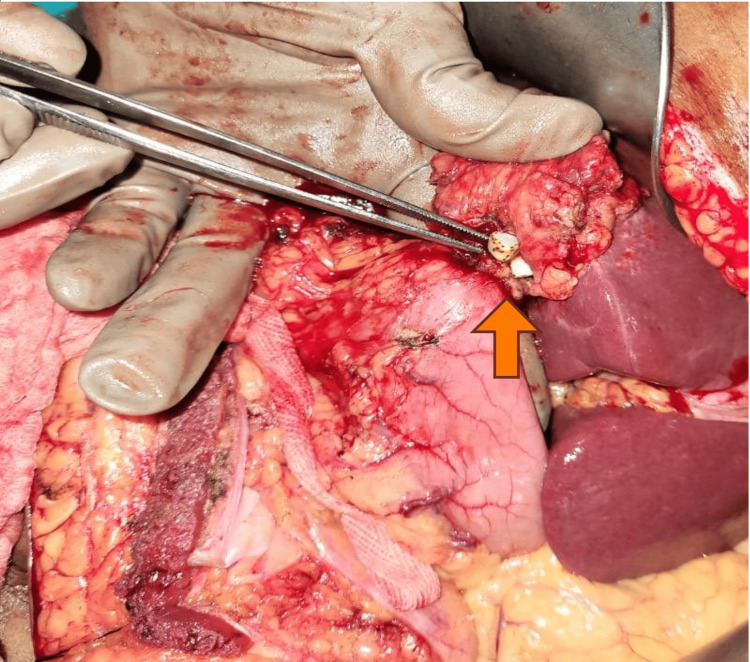 Figure 3
Figure 3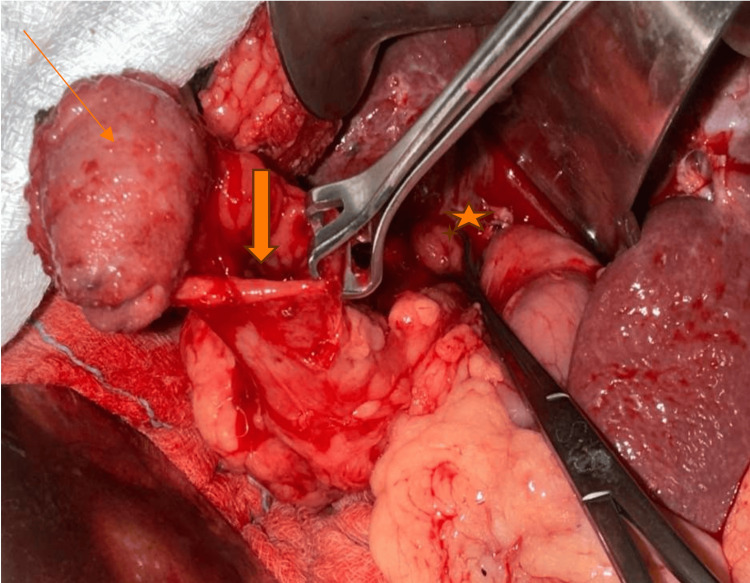 Figure 4
Figure 4| Characters | Patient 1 | Patient 2 | Patient 3 | Patient 4 | Patient 5 | Patient 6 | Patient7 |
| Age (years) and sex | 49/M | 55/F | 50/F | 69/M | 55/F | 67/M | 52/F |
| Symptoms | Abdominal pain, fever | Abdominal pain | Abdominal pain | Pain in the right upper abdomen | Abdominal pain | Abdominal pain, fever | Abdominal pain |
| Signs | Right hypochondrial tenderness | Right hypochondrial tenderness | Jaundice | Nil | Nil | Nil | Right hypochondrial tenderness |
| Comorbidities | Nil | Nil | DM | Nil | Nil | Nil | HCV positive |
| Total count (normal range: 4,000-11,000 cells/ µL) | 14,100 | 8,420 | 14,530 | 7,730 | 6,390 | 11,800 | 17,040 |
| Liver function test | - | - | - | - | - | - | - |
| Total bilirubin (normal range: 0.3-1.2 mg/dl) | 1.6 | 0.84 | 12.9 | 0.98 | 0.39 | 1.09 | 2.73 |
| Direct bilirubin (normal range: 0-0.2 mg/dl) | 0.84 | 0.20 | 7.08 | 0.1 | 0.16 | 0.65 | 1.1 |
| SGOT (normal range: 0-35 U/L) | 50 | 28 | 53 | 31 | 32 | 62 | 58 |
| SGPT(normal tange: 0-35 U/L) | 64 | 31 | 59 | 50 | 33 | 77 | 55 |
| Alkaline phosphatase (normal range: 30-120 U/L) | 275 | 163 | 390 | 139 | 181 | 189 | 433 |
| No. | Age (years)/sex | Preoperative diagnosis | Intra-op findings | Surgery | Duration of hospital stay | Postoperative complications |
| 1 | 49/M | Chronic calculous cholecystitis with choledocholithiasis | Dense adhesions, CDF, CCF, 3x3 cm impacted CBD stone with distal CBD stricture | Cholecystectomy + primary repair of CDF and CCF + RYHJ | 16 days | SSI |
| 2 | 55/F | Chronic calculous cholecystitis | Dense adhesions CGF, CCF | Cholecystectomy + primary repair of CGF and CCF | 18 days | SSI |
| 3 | 50/F | Chronic calculous cholecystitis with Mirizzi Type 5 | Dense adhesions, CDF, hard 3x2 cm impacted CBD stone with the destruction of CBD wall (CBF) | Cholecystectomy + primary repair of CDF + RYHJ | 14 days | Nil |
| 4 | 69/M | Chronic calculus cholecystitis | Dense adhesion, CGF | Cholecystectomy + having excision of CGF + primary repair of pylorus | 10 days | Nil |
| 5 | 55/F | Chronic calculus cholecystitis | Dense adhesions, CDF, CCF | Cholecystectomy + primary repair of CDF with omental patch and CCF primary repair | 12 days | Nil |
| 6 | 67/M | Chronic calculous cholecystitis with Mirizzi Type 5 | Dense adhesions CDF with CBF | Cholecystectomy + primary repair of CDF + RYHJ | 8 days | Nil |
| 7 | 52/F | Chronic calculous cholecystitis | Gall bladder contracted and hard, dense adhesions, CDF, CCF | Cholecystectomy + primary repair of CDF and CCF | 16 days | MODS, death |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBiliary and Gastrointestinal Fistulas · Esophageal and GI Pathology · Gastrointestinal disorders and treatments
Introduction
Cholecystoenteric fistula (CEF) was first documented by Bartholin in 1654; it’s an uncommon consequence of cholelithiasis, having an incidence of 3% to 5% within patients having cholelithiasis as well as 0.15% to 4.8% within those following biliary surgery [1-4]. It is characterized by a spontaneous, pathological communication between the gallbladder and the gastrointestinal tract, most often secondary to chronic inflammation caused by gallstones. These abnormal connections, collectively referred to as CEFs, include cholecystogastric fistulas (CGF), cholecystoduodenal fistulas (CDF), and cholecystocolonic fistulas (CCF). The duodenum is the most common site, comprising 75% to 80% of all such fistulas, followed by the colon and stomach [5]. An inflamed, constricted gallbladder adherent to adjacent viscera with a history of chronic calculous cholecystitis should alert the surgeon regarding the CEF.
The preoperative diagnosis of CEF has been challenging due to the vague nature of its symptoms, which include flatulence, dyspepsia, vomiting, diarrhea, and abdominal pain [6]. This poses a challenge to accurate preoperative diagnosis. Biliary fistulas are categorized as external or internal. External biliary fistulas (EBFs) are generally of iatrogenic origin. An internal biliary fistula (IBF) represents an abnormal connection between the biliary system and internal organs. It is categorized into bronchobiliary, biliobilary, as well as bilioenteric [7]. Chronic calculous cholecystitis is the most common etiology of IBF; less prevalent causes encompass peptic ulcer disease along with neoplasms of the pancreas, stomach, and colon, as well as the duodenum [7-9].
Materials and methods
Study design and setting
This retrospective study was conducted in the hepatopancreaticobiliary unit of the Department of Surgery at the All India Institute of Medical Sciences, Rishikesh, India. We analyzed all patients who were evaluated for symptomatic gallstone disease and were intraoperatively found to have CEF, undergoing surgical intervention between June 2024 and December 2024.
Patient selection
All patients who were diagnosed intraoperatively with CEF during surgery for symptomatic gallstone disease in our unit during the study period were included. Patients were identified retrospectively from hospital records and operative logs. No preoperative imaging criteria were used for diagnosis, as the condition was confirmed intraoperatively.
Inclusion and exclusion criteria
We included patients who were 18 years of age or older and were found to have a CEF during surgery. Only those who underwent surgical intervention for CEF within our unit between June 2024 and December 2024 were considered for inclusion. No specific exclusion criteria were applied in this study.
Data collection
The Institutional Ethics Committee of All India Institute of Medical Sciences, Rishikesh, approved (AIIMS/IEC/25/125) the study before data collection. Patient data were retrieved from medical records, operative notes, and electronic hospital databases. The following variables were collected and analyzed.
Preoperative Characteristics
These included demographics (age, gender), presenting symptoms, comorbidities, prior history of gallstone disease, and any preoperative imaging findings.
Biochemical Parameters
Liver function tests, complete blood counts, and renal function tests were the biochemical parameters included.
Intraoperative Findings
These included the presence of CEF, type of CEF, and additional biliary or gastrointestinal pathology.
Surgical Details
The type of surgical approach (laparoscopic vs. open) and procedures done were included.
Postoperative Outcomes
These included duration of hospital stay, postoperative complications (e.g., bile leak, surgical site infection, ileus), reoperation rates, and in-hospital mortality.
Statistical analysis
Descriptive statistics were used to summarize patient demographics, intraoperative findings, and postoperative outcomes. Categorical variables were presented as frequencies and percentages, while continuous variables were summarized as mean ± standard deviation (SD) or median with interquartile range (IQR), as appropriate.
Results
Seven patients were included in the study. Table 1 summarizes their preoperative characteristics. The mean age was 55.6 years (range: 49-69 years) with a male to female ratio of 3:4. Abdominal pain was present in all patients. Cholangitis was observed in three (42.86%), while four (57.14%) had no symptoms of cholangitis. Diabetes was present in one (14.29%) patient. Among those with cholangitis, three (42.86%) had an elevated total leukocyte count, of which one (14.29%) had an elevated total leukocyte count and abnormal liver function tests. All patients had elevated alkaline phosphatase levels. Gallstones were present in all patients, while bile duct stones were found in two (28.57%). Three (42.86%) patients underwent bilioenteric anastomosis using Roux-en-Y hepaticojejunostomy. Four (57.14%) patients had multiple fistulas: three (42.86%) had concomitant CCFs and CDFs, while one (14.29%) had both a CCF and a cholecystogastric fistula (CGF) (Figures 1-4). The mean hospital stay was 13.4 ± 3.8 days. Surgical site infections occurred in two (28.57%) patients, and one (14.29%) patient died in the postoperative period. The intraoperative findings and the procedures performed are detailed in Table 2.
Intraoperative picture of patient no. 2 showing cholecystocolonic and cholecystogastric fistulasImage credits: Nayana S Kumar
Intraoperative picture of a cholecystoduodenal fistula in patient no. 3.Image credits: Nayana S Kumar
Cholecystogastric fistula in patient no. 4 (arrow)Image credits: Nayana S kumar
Intraoperative picture of patient no. 5 showing gallbladder wall in continuity with the colon (arrow) and an excised cholecystoduodenal fistula (star).Image credits: Nayana S Kumar
Exemplary case presentations
Patient No. 2
A 55-year-old female patient presented with complaints of pain in her abdomen for the past six months. She underwent endoscopic retrograde cholangiopancreatography (ERCP) four months back for choledocholithiasis, and stenting was done, but no internal fistula opening was identified in ERCP. Other than pain, the patient had no other complaints. She was admitted for laparoscopic cholecystectomy and intraoperatively found to have dense adhesions, and both CCF and CGF. She underwent open cholecystectomy with primary repair of CCF and CGF. She developed a surgical site infection on postoperative day six, which was managed with IV antibiotics. The patient was discharged on postoperative day 18 with no other complications. During follow-up after one month, the patient was healthy with no complaints, and the wound fully healed.
Patient No. 3
A 50-year-old female patient presented with a history of pain in the abdomen, itching, and jaundice for one month. She was apparently asymptomatic before that. On examination, she was jaundiced and had scratch marks all over the body; investigation revealed slightly raised total counts, raised total bilirubin, and alkaline phosphatase. Intraoperatively found to have dense adhesions, CDF, a 3x2 cm hard impacted common bile duct (CBD) stone with destruction of the CBD wall and cholecystobiliary fistula (CBF) was noted. She underwent open cholecystectomy and primary repair of the CDF with Roux-en-Y hepaticojejunostomy. Her postoperative period was uneventful, and she was discharged on postoperative day 14 after one month; the patient was healthy with no complaints.
Discussion
A CEF is uncommon and typically observed in elderly female patients. Our case series included four female and three male patients. Spontaneous IBFs usually result from chronic calculous cholecystitis. Recurrent inflammatory episodes, often accompanied by gangrenous changes in the adjacent organ and gallbladder walls, can lead to erosion and fistula formation. The incidence of IBFs is as follows: cholecystoduodenal (70%), cholecystocolonic (14%), and cholecystogastric (6%), with simultaneous occurrences being much rarer [6, 10-12].
In our case study, four patients had more than one fistula; three patients had concomitant CCFs and CDFs, while one patient had CCFs as well as CGFs (Figures 1-4). All our patients had non-specific signs or symptoms indicative of biliary fistula. Consequently, a reliable preoperative diagnosis had not been established in any of the cases. The triad of symptoms, like right hypochondrial pain, diarrhea, and cholangitis, is typically regarded as the standard medical presentation of CEF. Diarrhea is the predominant symptom in nonemergency-onset CEF because of the laxative consequences of bile acids, which bypass the distal ileum and reach unabsorbed in the transverse colon [13,14].
Symptoms of CEF, including abdominal pain, nausea, weight loss, fever, vomiting, diarrhea, flatulence, and fat intolerance, aren't specific and common to several gastrointestinal disorders, leading to a frequent lack of prior suspicion for the diagnosis. Preoperative diagnosis based on signs was unattainable in all our cases. Jaundice secondary to CBD obstruction is frequently observed in patients with cholecystocholedochal fistula (CCDF) [10,15]. In our case series, two patients had jaundice. Although two of our patients underwent ERCP for choledocholithiasis, no fistulous opening had been observed.
Literature mentions that a CT scan is the most appropriate imaging modality for the diagnosis of CEF, as sonographic evaluation is frequently challenging. A nonoperative approach can be tried in asymptomatic patients or suboptimal surgical candidates [16]. In our study, all fistulas were identified only during the surgery, as preoperatively, patients were evaluated for symptomatic cholelithiasis, and only abdominal sonography was done. One should remain vigilant for the possibility of CEF, particularly in difficult dissection scenarios during cholecystectomy involving a small, contracted, chronically inflamed, and densely adherent gallbladder, while also taking care to avert iatrogenic damage. Furthermore, intraoperative cholangiography via the gallbladder assists in detecting any pre-existing fistulous tracts. The conventional management of CEF involves cholecystectomy as well as the closure of the fistulous orifice; this approach has been uniformly applied in all the surgeries done in our series. Exploration of the CBD, tube duodenostomy, T tube insertion, choledochoduodenostomy, enterolithotomy, and hepaticojejunostomy have been utilized as adjunctive procedures when warranted [17,18]. Initial reports indicated that diagnosis of CEF during laparoscopic cholecystectomy was associated with an increased rate of conversion to laparotomy [19,20]. Currently, because of the increased proficiency of surgeons in advanced laparoscopic techniques, including intracorporeal knotting and suturing, the duodenal mobilization conversion rate is minimal, and CEF is no longer deemed a laparoscopic limitation [20,21]. In our series, four procedures commenced laparoscopically but were switched to open surgery due to technical difficulties, while three cases were started as open-only. The average duration of hospital stay in our series was approximately 13 days (ranging from eight to 18 days). Our study recorded one mortality, representing 14% (1/7), which closely aligns with the literature, indicating rates between 15% to 22% [5, 10, 18].
Limitations
The retrospective design and small sample size (n=7) limit the generalizability of our findings, as a larger cohort would yield more robust statistical conclusions. Additionally, the series of cases evaluated represents the experience of a single tertiary care center, and long-term follow-up data were not included.
Conclusions
Preoperative diagnosis of CEFs is difficult, and intraoperative identification presents a significant challenge for surgeons, necessitating a modification of the intended treatment, usually an elective cholecystectomy. With the widespread adoption of laparoscopic cholecystectomy for symptomatic cholelithiasis, complications such as CEFs have become increasingly rare. However, they continue to be encountered in tertiary care centers, often as a consequence of neglected or long-standing cholelithiasis. Timely diagnosis and appropriate surgical management remain key to reducing morbidity associated with this uncommon but significant complication.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Biliary enteric fistula Surg Gynecol Obstet Glenn F Reed C Grafe WR 5275311531981 https://europepmc.org/article/med/7280941?client=bot&client=bot&client=bot&utm_medium=email&utm_source=transaction 7280941 · pubmed ↗
- 2Laparoscopic management of cholecystoenteric fistulas J Laparoendosc Adv Surg Tech A Chowbey PK Bandyopadhyay SK Sharma A Khullar R Soni V Baijal M 4674721620061700487010.1089/lap.2006.16.467 · doi ↗ · pubmed ↗
- 3Cholecystocolonic fistula: facts and myths. A review of the 231 published cases J Hepatobiliary Pancreat Surg Costi R Randone B Violi V 8181620091908931110.1007/s 00534-008-0014-1 · doi ↗ · pubmed ↗
- 4Laparoscopic management of cholecystoenteric fistula: a single-center experience J Int Med Res Li XY Zhao X Zheng P Kao XM Xiang XS Ji W 109010974520172841765110.1177/0300060517699038 PMC 5536399 · doi ↗ · pubmed ↗
- 5Cholecystoenteric fistula (CF) is not a contraindication for laparoscopic surgery Surg Endosc Angrisani L Corcione F Tartaglia A 103810411520011144342110.1007/s 004640000317 · doi ↗ · pubmed ↗
- 6Spontaneous internal biliary fistula, obstructive and nonobstructive types: twenty-year review of 55 cases Ann Surg Piedad OH Wels PB 75801751972506086110.1097/00000658-197201000-00013 PMC 1355161 · doi ↗ · pubmed ↗
- 7Spontaneous enterobiliary fistulas Surg Gynecol Obstet Safaie-Shirazi S Zike WL Printen KJ 7697721371973 https://europepmc.org/article/med/47464974746497 · pubmed ↗
- 8Bouveret's syndrome presenting as upper gastrointestinal hemorrhage without hematemesis Am Surg Jones TA Davis ME Glantz AI 786789672001 https://journals.sagepub.com/doi/pdf/10.1177/00031348010670081511510584 · pubmed ↗