Anesthetic Management of a Patient With Acute Necrotizing Encephalopathy Type 1
Shamim A Beigh, Andrea Yap

TL;DR
This case report details the anesthetic care of a child with a rare brain condition during hip surgery, highlighting the challenges and strategies used.
Contribution
The paper provides a detailed anesthetic management approach for a rare neurological condition with limited existing literature.
Findings
ANE1 shares symptoms and pathology with mitochondrial disorders, complicating anesthetic choices.
Perioperative management included careful medication selection and monitoring to avoid triggering seizures or metabolic crises.
The case highlights the importance of a multidisciplinary approach for patients with rare neurological conditions.
Abstract
Acute necrotizing encephalopathy (ANE) is a progressive neurodegenerative condition that often arises after exposure to a variety of viruses and systemic infections, including influenza and SARS-CoV-2. It typically presents with developmental delay, seizures, dysarthria, and ataxia. Acute necrotizing encephalopathy type 1 (ANE1) is recurrent, and familial cases have been associated with mutations in the RAN-binding protein 2 (RanBP2) gene. The disease shares symptomatic and pathological resemblance with mitochondrial metabolic disorders. In this case report, we present the anesthetic management of a seven-year-old boy with ANE1 who underwent total hip reconstruction. Literature on the anesthetic management of such patients is sparse, and we discuss the patient's perioperative anesthetic management, including medications, monitoring, and care, along with a literature review.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
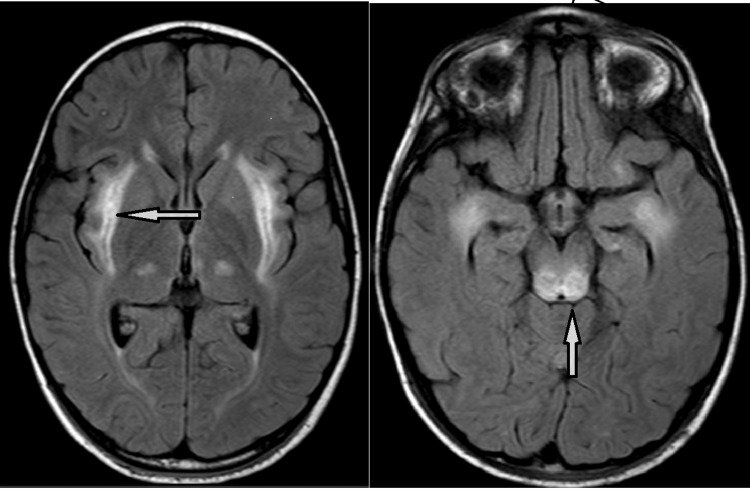 Figure 1
Figure 1| Anesthetic considerations for managing acute necrotizing encephalopathy | |
| Cardiac and respiratory evaluation | Preoperative cardiac and respiratory evaluation to rule out any underlying decompensation. Preoperative cardiac and respiratory optimization to improve post-procedure outcome. |
| Seizure management | Preoperative management of antiepileptic therapy. Documentation of therapeutic anticonvulsant levels. Normalize serum electrolytes and glucose. Midazolam has antiepileptic effects. |
| Acid-base and blood sugar management | Minimize preoperative fasting. Use dextrose-containing IV fluids for maintenance in the preoperative fasting period to provide basal glucose requirements. Avoid hypoglycemia in the perioperative period. Check preoperative lactate levels. Frequent intraoperative serum lactate, pH, and glucose monitoring. Avoid lactate-containing fluids (e.g., Ringer’s lactate). Monitor the depth of anesthesia and avoid long-acting opioids. Postoperative respiratory monitoring for major procedures. Maintain normothermia and normocapnia, and avoid any hypoxia. |
| Infection risk | Complete aseptic precautions. Proper antibiotic coverage. |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsInfectious Encephalopathies and Encephalitis · Viral Infections and Immunology Research · Long-Term Effects of COVID-19
Introduction
Acute necrotizing encephalopathy (ANE) was first described by Mizuguchi in 1995 and is an extremely rare and potentially lethal neurological disease. It is characterized by progressive neurodegeneration with the development of symmetrical necrotic lesions in the thalamus, pons, and brainstem that can arise following exposure to a variety of systemic infections, including influenza A and B, parainfluenza 2, and SARS-CoV-2 [1-3]. It usually presents in infancy with seizures, dysarthria, and ataxia with developmental delay. Most of the reported ANE cases are sporadic; however, recurrent and familial cases have been associated with RAN-binding protein 2 (RanBP2) gene mutations [4]. RanBP2, a multifunctional protein, plays a key role in nucleocytoplasmic transport [5-7]. The formation of abnormal RanBP2 can lead to disruptions in nuclear signal and blood-brain barrier function. This subset of ANE patients with RanBP2 gene mutations is categorized as acute necrotizing encephalopathy type 1 (ANE1) [4].
RanBP2 mutations in ANE1 not only have neurological sequelae but also mitochondrial enzyme dysfunction. This leads to impaired glucose metabolism, adenosine triphosphate (ATP) production, and loss of coupling of oxidative phosphorylation [8,9]. This is further compounded by the development of hepatic and renal dysfunction and makes the patient sensitive to the development of hypoglycemia and lactic and metabolic acidosis. RanBP2 mutation can also affect immune function by impairing the ability of mitochondria to regulate the secretion of proinflammatory cytokines, such as IL-1ß and IL-18, thereby altering the cellular response to infection. Unrestrained immune activation results in marked systemic inflammation with deleterious consequences to the host, a condition termed "cytokine storm" [10-15].
Herein, we present the case of a patient with ANE1 disease who required general anesthesia for total hip reconstruction. Due to the rare nature of the disease, there is limited information in the literature regarding the anesthetic and perioperative management of such patients.
Case presentation
A seven-year-old boy, weighing 32 kg and a known case of ANE1, was scheduled for total hip reconstruction under general anesthesia. The child had been well until four years of age when he tested positive for influenza (H1N1) and later developed H1N1 meningitis. This progressed to acute disseminated encephalomyelitis. An MRI of the brain revealed a hyperintense signal in the external capsules, both thalami, dorsal pons, and hippocampi, with relative sparing of the basal ganglia, suggesting an infective or metabolic encephalopathy (Figure 1). A genetic workup revealed a monoallelic mutation of the RanBP2 gene.
FLAIR axial images showing hyperintense signals in the external capsules, both thalami, dorsal pons, and hippocampi, with relative sparing of the basal ganglia.The arrow in the left-side MRI image indicates a hyperintense signal in the external capsule, while the arrow in the right-side image points to the signal in the dorsal pons.FLAIR: Fluid-attenuated inversion recovery
Upon further inquiry, it was noted that two of his siblings had died from meningitis. Over the next few years, he experienced multiple recurrences of ANE, which worsened his motor and cognitive function. He developed global developmental delay, poorly controlled seizures, a spastic-dystonic lower limb movement disorder, upper limb dystonic posturing, and right-sided hip dislocation. All his symptoms resulted in him being wheelchair-bound and dependent for all activities of daily living, with a Gross Motor Function Classification System (GMFCS) level of V. His medications included levetiracetam, clonidine, and clobazam, administered twice a day. In the past, he had undergone short diagnostic and surgical procedures, with a post-procedure admission to a high dependency unit (HDU), and these procedures were uneventful.
On clinical examination, he was wheelchair-bound, and his vitals were within normal limits. His cardiac and respiratory evaluations were unremarkable. His laboratory investigations, including liver, coagulation, and renal function tests, were within the normal range. Hemoglobin was 13.8 g/dl, and preoperative blood sugar was 103 mg/dl. His airway examination revealed a Mallampati score of 2, and there was no documented history of a difficult airway in the past.
The patient was premedicated with oral midazolam 0.4 mg/kg, 30 minutes before induction of anesthesia. ECG, blood pressure, oxygen saturation probe, and depth of anesthesia monitors were connected prior to the induction of anesthesia. Anesthesia was induced with a propofol bolus of 2 mg/kg and fentanyl 2 mcg/kg. He was paralyzed with cisatracurium 3 mg and intubated easily. Following induction, an arterial line was inserted, along with a 22 G cannula and a second large-bore IV cannula. Anesthesia was maintained with dexmedetomidine 0.2 mcg/kg/hr, remifentanil 0.2-0.3 mcg/kg/minute infusion, together with 0.4 minimal alveolar concentration (MAC) sevoflurane. Perioperatively, the patient received paracetamol 15 mg/kg and ketorolac 0.5 mg/kg. Plasmalyte was used intraoperatively to maintain hydration, and dextrose 10% was administered at 1-2 ml/kg/hr for glucose maintenance. Arterial blood gases were checked hourly, and the results were within normal limits. At the end of the surgery, the patient was extubated uneventfully and transferred to the post-anesthesia recovery unit before going to the general ward.
Discussion
ANE1 is an extremely rare neurological condition, and information on the anesthetic management of such patients is limited. ANE1 has a pathological and clinical resemblance to other mitochondrial metabolic disorders, particularly Leigh’s disease. The management of ANE1 patients can be given the same perioperative considerations as these patients. This includes the maintenance of hydration, normoglycemia, normothermia, and acid-base balance, as well as the prevention of stress, catabolism, and infection. We maintained the patient on 2 ml/kg/hr of 10% dextrose to prevent hypoglycemia and did a blood gas analysis every hour to ensure that his blood sugar and acid-base balance were maintained within normal limits. Plasmalyte was used in place of Ringer's lactate for maintenance fluid, as lactate-containing fluids are prone to induce lactic acidosis and should be avoided. Temperature regulation and prevention of hypothermia were managed with the use of a fluid warmer and convective air warming blanket (Bair Hugger, 3M, United States).
One of the important considerations in the anesthetic management of patients with mitochondrial dysfunction is the possibility of propofol infusion syndrome. Propofol infusion syndrome is well described as a serious reaction in patients receiving long-term propofol infusion. The syndrome is characterized by severe lactic acidosis, followed by rhabdomyolysis and lipidemia, which can lead to cardiovascular collapse and death [16]. Propofol inhibits multiple electron transport chain complexes and acylcarnitine function in the mitochondria, resulting in an increase in serum acylcarnitines during prolonged infusions [17]. Multiple case reports suggest that patients with mitochondrial dysfunction are at risk of propofol infusion syndrome during prolonged exposure [18,19]. In our case, we maintained anesthesia with an infusion of dexmedetomidine and remifentanil with sevoflurane. Dexmedetomidine is considered safe for the anesthetic management of ANE patients [20]. Throughout the anesthesia procedure, anesthetic depth was monitored with the use of a Sedline Patient State Index (PSI) monitor (Sedline, Masimo Corp., United States).
Since ANE1 is known to get triggered by stress and infection, extreme care was taken to maintain an aseptic environment throughout the perioperative phase. We minimized the movement of staff in and out of the operating theatre and all aseptic precautions were taken throughout the procedure. The patient was given a stress dose of 50 mg hydrocortisone and also received two doses of antibiotic during the perioperative period. Table 1 summarizes the perioperative considerations for the management of patients with ANE.
Conclusions
In conclusion, preoperative evaluation and optimization of the cardiac, neuromuscular, and respiratory systems are mandatory in patients with ANE1. Perioperatively, every effort must be made to maintain hydration, normoglycemia, and the prevention and correction of acid-base imbalance. Avoidance of lactate-containing fluids and perioperative stress, as well as the prevention and treatment of infection, are paramount.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Acute necrotising encephalopathy of childhood: a new syndrome presenting with multifocal, symmetric brain lesions J Neurol Neurosurg Psychiatry Mizuguchi M Abe J Mikkaichi K Noma S Yoshida K Yamanaka T Kamoshita S 555561581995774540210.1136/jnnp.58.5.555PMC 1073485 · doi ↗ · pubmed ↗
- 2Acute necrotizing encephalopathy of childhood in non-Asian patients: report of three cases and literature review J Child Neurol Mastroyianni SD Gionnis D Voudris K Skardoutsou A Mizuguchi M 8728792120061700510410.1177/08830738060210101401 · doi ↗ · pubmed ↗
- 3COVID-19-associated acute hemorrhagic necrotizing encephalopathy: imaging features Radiology Poyiadji N Shahin G Noujaim D Stone M Patel S Griffith B 119120296202010.1148/radiol.2020201187 PMC 723338632228363 · doi ↗ · pubmed ↗
- 4The interplay of infection and genetics in acute necrotizing encephalopathy Curr Opin Pediatr Neilson DE 751757222010 https://pubmed.ncbi.nlm.nih.gov/216103322161033210.1097/MOP.0b 013e 3283402 bfe · doi ↗ · pubmed ↗
- 5Infection-triggered familial or recurrent cases of acute necrotizing encephalopathy caused by mutations in a component of the nuclear pore, RANBP 2Am J Hum Genet Neilson DE Adams MD Orr CM 4451842009 https://pubmed.ncbi.nlm.nih.gov/191188151911881510.1016/j.ajhg.2008.12.009PMC 2668029 · doi ↗ · pubmed ↗
- 6Localization of the Ran-GTP binding protein Ran BP 2 at the cytoplasmic side of the nuclear pore complex Eur J Cell Biol Wilken N Senécal JL Scheer U Dabauvalle MC 211219681995 https://pubmed.ncbi.nlm.nih.gov/86036738603673 · pubmed ↗
- 7A giant nucleopore protein that binds Ran/TC 4Nature Yokoyama N Hayashi N Seki T 1841883761995760357210.1038/376184 a 0 · doi ↗ · pubmed ↗
- 8Ran BP 2 modulates Cox 11 and hexokinase I activities and haploinsufficiency of Ran BP 2 causes deficits in glucose metabolism P Lo S Genet Aslanukov A Bhowmick R Guruju M 17722006 https://pmc.ncbi.nlm.nih.gov/articles/PMC 162610810.1371/journal.pgen.0020177 PMC 162610817069463 · doi ↗ · pubmed ↗