Letter to the editor: Urethrovesical anastomosis training: An innovative dual penile catheter approach
M. Tetou, M.A. Sobhi, M. Mrabti, A. Elbahri, A. Ameur, M. Alami

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
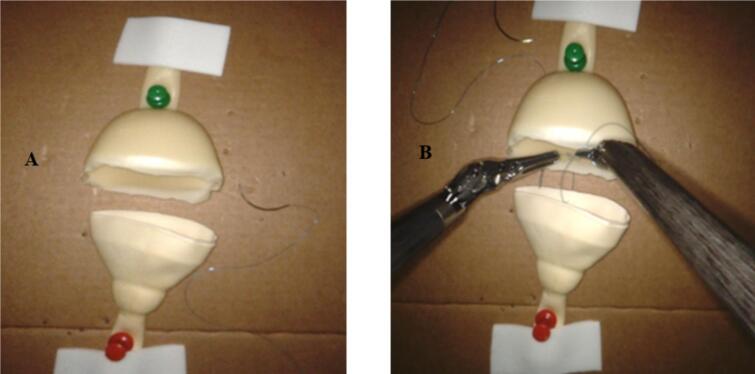 Figure 1
Figure 1 Figure 2
Figure 2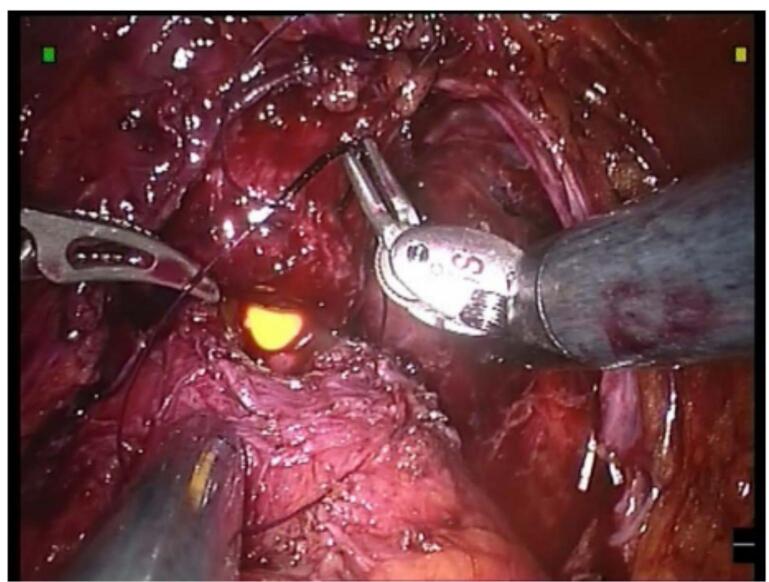 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSurgical Simulation and Training · Cardiac, Anesthesia and Surgical Outcomes · Colorectal Cancer Surgical Treatments
Dear Editor,
Urethrovesical anastomosis is a crucial stage in radical prostatectomy. Robot-assisted laparoscopic surgery makes it possible to perform this delicate procedure in a narrow space between the urethra and the bladder neck with great precision [1,2]. However, this procedure, performed at the end of the operation, becomes more difficult because of the fatigue accumulated by the surgeon [3].
Indeed, learning this technique by urologists can be difficult, notably because of the learning curve and the lack of accessible practical models [4,5]. In order to facilitate this training, we recently experimented with a simple and inexpensive method using two peniflow catheters, offering learners a realistic and repetitive training opportunity. This tip, which we wish to share with the urology community, has demonstrated a positive impact on technical mastery of urethrovesical anastomosis, particularly in a context of limited resources.
Methodology
1
Model setup
1.1
This training setup uses two Peniflow catheters to replicate the urethra and bladder (Fig. 1). Their latex composition and flexibility mimic the natural resistance of urethrovesical tissues, making the simulation both realistic and cost-effective. By providing a reproducible platform, this model allows surgical trainees to refine their suturing techniques in a structured and controlled setting.Fig. 1(A) A simulated urethrovesical anastomosis training model using two peniflow catheters. (B) The suturing of the posterior layer in the simulated urethrovesical anastomosis.Fig. 1
Step-by-step assembly
1.2
Bladder representation (vesical neck)
1.2.1
To replicate the bladder neck, a Peniflow catheter (outer diameter: 15–20 mm) is selected. A circular incision is carefully made at its tip, forming a vesical orifice (10–12 mm in diameter), which corresponds to the post-prostatectomy bladder opening seen in clinical practice.
Urethral section simulation
1.2.2
A second Peniflow catheter is modified to represent the membranous urethra, the portion that remains following prostate removal. The distal end is cut and shaped to closely mimic the urethral sleeve, ensuring an accurate anastomotic site for training purposes.
Secure attachment to base
1.2.3
Both components are firmly secured onto a stable, non-slip cardboard surface to ensure a fixed and realistic training experience.
The stabilization technique involves Small pins or tacks, which provide precise anchoring while avoiding damage to the latex material.
Suturing simulation
1.2.4
Trainees engage in continuous suturing exercises, mimicking the posterior and anterior layers of a real urethrovesical anastomosis.
The following specifications are recommended:
- ‐Suture type: 3-0 or 4-0 monofilament (e.g., polydioxanone or polyglecaprone).
- ‐Needle selection: 17–19 mm curved needles, either reverse cutting or taper-point, to facilitate precise passage through the latex.
- ‐Standardized suturing sequence:
- •Posterior layer begins from 4 o'clock to 8 o'clock, using either an interrupted or continuous suture pattern (Fig. 1).
- •Anterior layer: Final alignment of urethral and bladder edges is completed meticulously (Fig. 2).Fig. 2. Completed urethrovesical anastomosis in the simulating model.Fig. 2
Evaluation and feedback
2
Although we have not conducted a formal quantitative study, we collected structured feedback from surgeons and trainees in our department who used the model in practice sessions.
- •All participants (n = 15) found the model realistic and beneficial for training (Fig. 3).Fig. 3. Peroperative image illustrating an urethrovesical anastomosis during a robot-assisted radical prostatectomy [6].Fig. 3
- •10 reported increased confidence in performing urethrovesical anastomosis.
- •8 noted improved suturing speed and precision after repeated practice.
This positive reception highlights the model's potential for skill acquisition and confidence-building among trainees. Future studies could integrate standardized assessment tools, such as the Visual Analog Scale (VAS) or validated simulation scoring systems, to formally evaluate its effectiveness.
Comparison with other training models
3
There is no universally accepted model for urethrovesical anastomosis training. Existing alternatives include:
- •Synthetic tube models (e.g., millimeter-scale silicone or rubber tubing): These lack anatomical realism and do not accurately replicate tissue resistance.
- •Cadaveric or animal models: While offering realistic tissue handling, these are costly, ethically restrictive, and require specialized facilities.
- •High-fidelity robotic simulators: While beneficial, these are expensive and not always accessible in resource-limited settings.
Conclusion
4
Our dual catheter approach provides a simple, realistic, and affordable alternative that bridges the gap between accessibility and simulation fidelity.
Author contribution
All authors have made substantial contributions to the manuscript as follows:
M. Tetou, MA. Sobhi, M. Alami: Concept and design of the training model, manuscript drafting.
M. Tetou, MA. Sobhi, M. Mrabti: Data collection and interpretation, manuscript revision.
M. Tetou, MA. Sobhi, M. Mrabti: Data analysis, manuscript editing.
M. Tetou, A. Elbahri, A. Ameur, M. Alami: Critical revision of the manuscript for important intellectual content.
All authors have reviewed and approved the final manuscript.
Consent
This training approach did not involve direct patient participation or identifiable patient data. Therefore, individual patient consent was not required.
Ethical approval
This study did not involve human participants or patient data; therefore, ethical approval was not required. The technique was developed and assessed in a simulated setting for educational purposes.
Guarantor
M. Tetou.
Research registration number
Our article focuses on a training model, not a research study, and therefore does not require registration of research studies.
Funding
This paper did not receive any specific grant from funding agencies in the public, commercial or non-profit sectors.
Conflict of interest statement
The authors of this paper declare that there are no conflicts of interest to disclose regarding the content of this manuscript.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Patel V.R.Shah K.Palmer K.J.Thaly R.Coughlin G.Robotic-assisted laparoscopic radical prostatectomy: a report of the current state Expert. Rev. Anticancer. Ther.792007126912781789242710.1586/14737140.7.9.1269 · doi ↗ · pubmed ↗
- 2Menon M.Shrivastava A.Tewari A.Sarle R.Hemal A.Peabody J.O.Laparoscopic and robot assisted radical prostatectomy: establishment of a structured program and preliminary analysis of outcomes J. Urol.168320029459491218719610.1016/S 0022-5347(05)64548-X · doi ↗ · pubmed ↗
- 3Satava R.M.Surgical education and surgical simulation World J. Surg.25112001148414891176075310.1007/s 00268-001-0134-0 · doi ↗ · pubmed ↗
- 4Abboudi H.Khan M.S.Aboumarzouk O.Guru K.A.Challacombe B.Dasgupta P.Current status of validation for robotic surgery simulators–a systematic review BJU Int.111220131942052267234010.1111/j.1464-410X.2012.11270.x · doi ↗ · pubmed ↗
- 5Hung A.J.Zehnder P.Patil M.B.Cai J.Ng C.K.Aron M.Face, content and construct validity of a novel robotic surgery simulator J. Urol.18632011101910252178446910.1016/j.juro.2011.04.064 · doi ↗ · pubmed ↗
- 6Rochat C.Prostatektomie radicale robot assistee (Da Vinci (R)): abord transperitoneal Journal für Urologie und Urogynäkologie 13420061721