Non-communicable disease multi-morbidity in policies from India, Thailand, and South Africa: A comparative document review
Linju Joseph, Rakhal Gaitonde, Charutha Retnakumar, Athira Krishnan, Thoniparambil Ravindranathanpillai Lekha, Neethu Sasidharan, André van Rensburg, Naomi Levitt, Nilawan Upakdee, Jissa Vinoda Thulaseedharan, Mathew Joseph Valamparampil, Sivadasanpillai Harikrishnan

TL;DR
This paper compares how India, Thailand, and South Africa address multiple chronic non-communicable diseases in their health policies.
Contribution
The study reveals the absence of specific policies for managing multi-morbidity in NCDs in three LMICs.
Findings
None of the three countries have specific policies for NCD multi-morbidity.
Health promotion targets multiple risk factors, but self-management is limited to specific diseases like diabetes.
The study emphasizes the need for patient-centered policies addressing social determinants of health.
Abstract
Over the years, non-communicable diseases (NCDs), as well as the number of people with multiple chronic NCDs or multi-morbidity, are on a sharp rise globally, especially in low and middle-income countries (LMICs). This review attempts to deepen the knowledge (policy landscape) of how managing multiple NCDs and associated challenges are addressed across the health systems policies from India, South Africa and Thailand. We conducted a search of two search engines (PubMed and Google) and the websites of national departments from February 2022 to December 2022. An analytical framework was produced for the qualitative document analysis, focusing on definitions of multi-morbidity, potential policy actions at patient, provider, health system, and macro-level domains, including social determinants of health. We utilised framework analysis of the national-level policies and related documents to…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
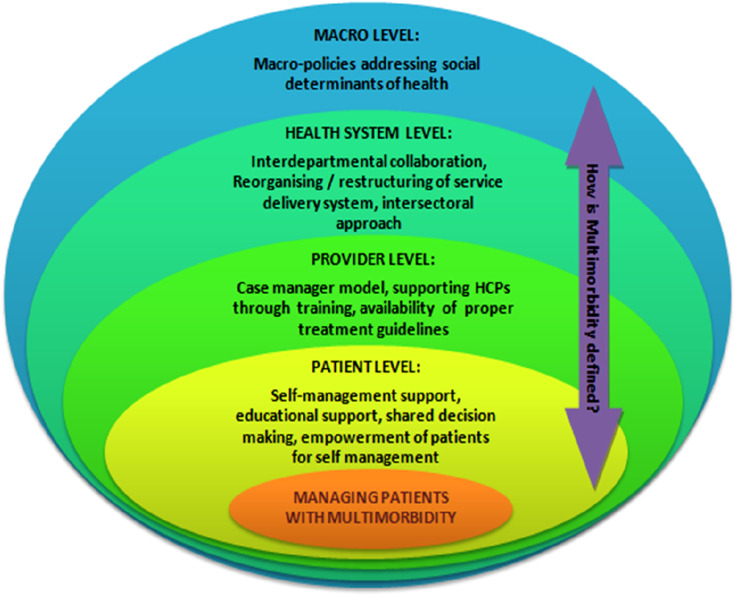 Figure 1
Figure 1 Figure 2
Figure 2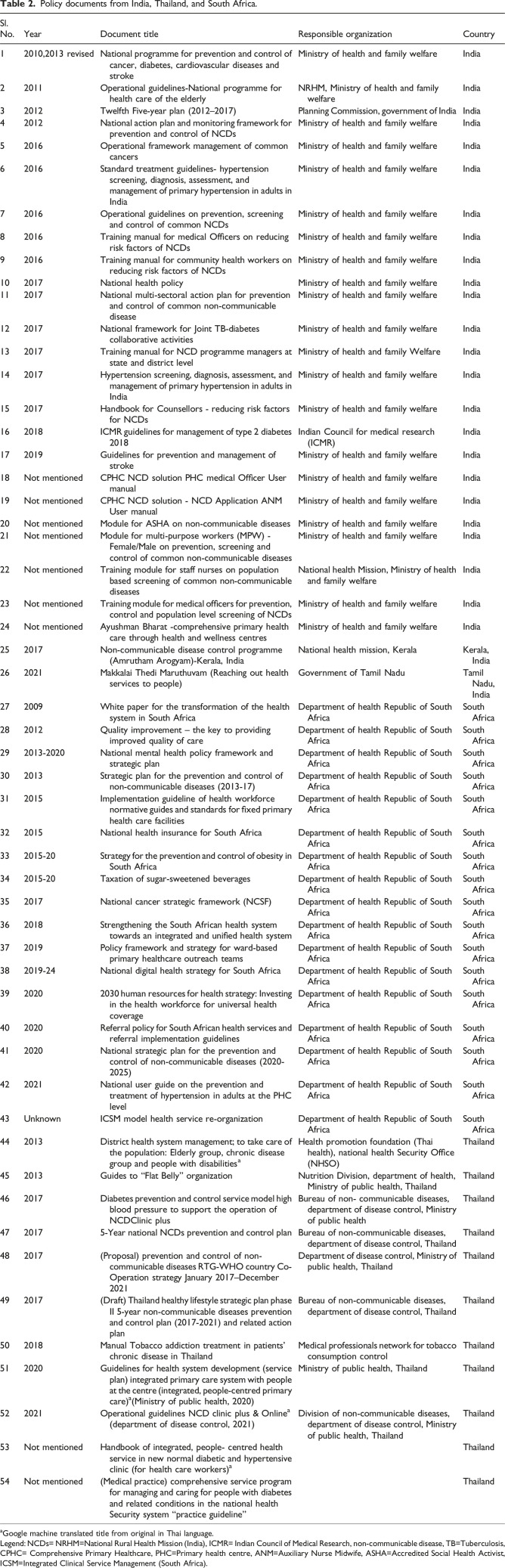 Figure 3
Figure 3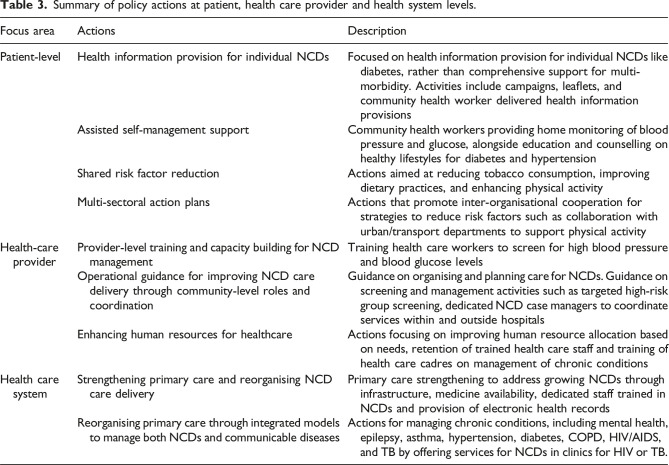 Figure 4
Figure 4- —Medical Research Councilhttps://doi.org/10.13039/501100000265
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsChronic Disease Management Strategies · Diabetes Management and Education · Global Public Health Policies and Epidemiology
Introduction
Over the past few decades, life expectancy has increased globally with dramatic changes in low- and middle-income countries (LMIC) settings.^ 1 ^ For example, the average life expectancy in India increased from 63 in 2002 to 70.2 years in 2022.^ 2 ^ In parallel with rising life expectancy, the demand for healthcare utilisation also increased owing to the rise in chronic non-communicable diseases (NCD).^ 3 ^ A nationally representative cross-sectional study from India reported that the average number of outpatient visits over the previous year rose from 2.2 to 6.2, while the proportion of individuals reporting a hospital stay in the last three years increased from 9% to 29% among those without any NCDs and those with two or more NCDs, respectively. NCDs include cancers, cardiovascular diseases, chronic respiratory diseases, mental, and behavioural conditions and diabetes.^ 4 ^ Furthermore, the average years spent in good health is not increasing in LMICs; even worse, it is declining in some countries.^ 5 ^ Despite this epidemiological transition, most healthcare systems in LMICs are disease-oriented and still primarily focused on episodic and acute care that is ill-suited for the needs of chronic NCDs.^6–8^ Within the context of rising prevalence and persistent socio-economic disparities prevailing in LMICs, NCDs tend to co-exist together in an individual rather than being seen in isolation.^9,10^ Consequently, multi-morbidity, commonly defined as the co-occurrence of two or more chronic conditions, has emerged as a growing public health concern in LMICs.^11,12^ While the above definition is widely used, there have been criticisms for the lack of reflection on the complexities of living with multi-morbidity.^ 13 ^ Several authors suggested that multi-morbidity should be understood as the presence of two or more chronic conditions (whether chronic diseases, acute diseases, bio psychosocial factors, or somatic risk factors) within an individual, along with consideration of various modifiers that influence its effects, such as social networks, healthcare utilisation, disease burden, and coping strategies. The more inclusive definition seeks to capture the complexities and consequences of living with multi-morbidity, providing a foundation for better understanding and addressing them in public health policies.^14,15^
One of the significant challenges faced by patients with multi-morbidity (those accessing care) is the treatment burden due to managing multiple appointments, complicated medication regime, and several lifestyle changes.^16,17^ Therefore, treatment itself can represent an excessive burden for patients with multi-morbidity, alongside their burden of illness.^ 18 ^ The growing literature on multi-morbidity treatment burden from LMICs suggests how treatment burden in multi-morbidity is linked with poor quality of life from LMICs.^19,20^ Further, multi-morbidity increases out-of-pocket expenditure for patients from low-resource health systems.^4,21–23^
Given the evidence on poorer health care access and quality of care, managing multi-morbidity necessitates health system redesign in LMICs. The Sustainable Development Goals (SDG)-3 recommends universal health coverage to ensure access to high-quality care across the life course.^ 24 ^ The World Health Organization (WHO) also recommends better policies for tackling social determinants of health and increasing awareness of multi-morbidity among policymakers.^ 25 ^ Therefore, we selected three countries based on convenience from three WHO regions; Sub-Saharan region (South Africa), South-Asian region (India) and South-East Asia (Thailand) to assess the current national policies on co-existent nature of chronic NCDs. The health system’s structure and financing differ in South Africa, Thailand, and India. For example, Thailand’s universal health coverage (UHC) efforts ensure free primary care for most of the Thai population.^ 26 ^ Both India and South Africa launched national health insurance schemes to provide protection against catastrophic out of pocket payments as a step towards UHC and are currently in different phases of implementation.^27,28^
A clear and well-defined policy sets the foundation for proactive care, and in the context of multi-morbidity, it can lead to care that is more integrated, which necessitates the strengthening of primary care. Policy, in this context, is a crucial acknowledgment of the existing problem and serves as an expression of the intent to address it effectively. However, it is important to note that the mere existence of a policy may not automatically lead to significant changes in practice and outcomes.^ 29 ^
Within this context, our study aims to synthesise and identify the gaps in the current policies of NCD multi-morbidity management in primary care settings in India, Thailand, and South Africa. Further, we examined policies to gather any lessons that may be adapted for the effective management of NCD multi-morbidity in LMICs. The following research questions were formulated for our review:
- • How have the current policies constructed the problem of NCD multi-morbidity, and what type of solutions are being suggested?
- • What are some of the policy actions (if any) based on current policies, that can be built upon for a policy on NCD-multi-morbidity at the primary care level?
Materials and methods
Study design
We conducted a qualitative document review and analysis^ 30 ^ on the national-level policies and policy-related documents relevant to patients with NCD multi-morbidity. Three countries India, Thailand, and South Africa were conveniently sampled to explore how NCD multi-morbidity has been articulated. Further details on NCD burden for the three countries are provided in Online Supplemental Box S1.
Search strategy and data selection
For this study, we were interested in government health policy documents to synthesise current management of NCD multi-morbidity. We developed a broad search strategy (LJ and CR) and focused on current policy documents, guidelines, action plans, and management frameworks for NCD multi-morbidity management.^15,31^We searched government health department websites and Google search engine between February 2022 to December 2022 without any restrictions on time period. Furthermore, NCD programme managers and health system experts from Thailand, India, and South Africa were consulted to identify policy or guideline documents related to the management of NCD multi-morbidity. We also included recent inter- and intra-departmental consultation documents from the government considered pertinent to informing forthcoming policies, as suggested by programme managers. (Search strategy is provided in the online supplement; Box S2, Additional country wise strategies in Box S3-S4).
Two researchers (LJ and CR) screened potentially eligible documents independently, and clarification of the eligibility of the inclusion of documents was performed with a wider team (PJ and RG). We excluded single-disease clinical practice guidelines, policies with a focus only on tertiary care, expert opinions and editorials, and policy documents superseded by more recent policy documents unless they provided additional crucial information related to the management of multi-morbidity (Table 1).Table 1.Inclusion and exclusion criteria for documents.DomainInclusion criteriaExclusion criteriaChronic conditionsNational policies addressing chronic NCDsSingle disease clinical practice guidelinesStrengthening of primary careNational policies detailing strengthening of primary care, reorganising care for managing chronic NCDsPolicies addressing tertiary or secondary care aloneUniversal health coverageNational policies detailing universal access to healthcareExpert opinions, editorials or articles mentioning universal health coverage without a national policy
Analytical framework
We developed an analytical framework (Figure 1) using an iterative approach that involved multiple discussions (LJ, CR, PJ, RG) and a focused literature review of approaches to managing NCD multi-morbidity. The overarching research question was to explore how multi-morbidity has been addressed (if at all) and the problem of multi-morbidity constructed in the policy documents from the three selected countries. Additionally, to identify the gaps in the current policies, we mapped potential strategies either that are suggested in the policy documents directly or that would have potential to manage NCD multi-morbidity. The main categories making up the framework were definitions of NCD multi-morbidity used or implied in the policy document and interventions/strategies (potential) for the management of NCD multi-morbidity categorised as being relevant at the patient, provider, health system and macro levels, including social determinants of health based on the literature.Figure 1.Analytic framework for classifying multi-morbidity management in policies.
As defined in the introduction, we explored whether the documents articulated NCD multi-morbidity holistically, i.e., by including the influence of broader social, environmental, aging, and recognition of the complexities of living with multi-morbidity, as they are important in managing multi-morbidity as a public health issue.
At the individual or patient level, we focused on policy directions for self-management support for NCD multi-morbidity.^ 32 ^ Furthermore, we explored patient-level strategies that encouraged patient-centred care for self-management, which incorporated personal preferences and functional priorities in the treatment planning of multi-morbidity.^ 33 ^
At the provider level, we assessed policy directions that support healthcare providers in delivering integrated care for the management of multi-morbidity. Based on evidence on efficacy from previous studies conducted in high-income countries, we incorporated case manager models that incorporated integrated management of multi-morbidity in our analytical framework.^34,35^ Case manager models incorporate nurses or specific health care workers for preliminary check-ups, including physical and mental health. Further, these models addresses difficulties with current treatment regimens, problems with daily activities and social problems, and support patients to achieve their goals followed by the diagnosis by the physician resulting in an improvement in the quality of life.^34,35^ Interventions for provider support such as training, availability of treatment guidelines, etc., were also included in our analytical framework and explored in the policy review.
For strategies at the organisational or health system levels, we included collaborative teamwork across different departments for the overall management of patients with multi-morbidity. Policy directions that aimed at a whole system change or service reorganisation were incorporated in the analytical framework. For example, a “Multiple Long-term Conditions Care Model” developed by the Joint Action on Chronic Diseases and Promoting Healthy Ageing across the Life Cycle focused on improving health outcomes through quality health care delivery, decision supports, self-management supports, utilisation of information systems and technology, and social and community resources that targeted interventions at the health system level.^ 36 ^ Furthermore, we considered the WHO’s framework for 'integrated people-centred health services' that focused on health systems redesign to meet the people’s needs particularly continuity of care in our analytical framework.^ 26 ^
For policy actions at the macro level, we considered policies and interventions improving social determinants of health as described by Dahlgren and Whitehead^ 37 ^ in our analytical framework. Interventions or policy actions aimed at mitigating upstream factors such as income inequalities, poverty, work-related health hazards, and lack of social cohesion with the aim of preventing or managing NCD multi-morbidity.
Data analysis
As described, we first developed our analytical framework.^ 38 ^ Next, we assessed all retrieved documents to identify the specific policies relevant to the management of multi-morbidity according to the inclusion criteria.^ 39 ^ Documents in Thai were translated using Google Translate. Documents from each country were coded according to the categories of the developed analytical framework in an Excel spreadsheet. Two coders (CR/ AK, and LTR/NS) applied the analytical framework. Another coder (LJ) coded randomly selected 10% of the policies for multi-analyst triangulation,^ 40 ^ and themes were finalised with discussion with a third analyst (RG). We then examined the results to understand the possible gaps and potential areas for further policy action. We extracted examples from policy documents to illustrate our analysis.
Results
Search results
We retrieved 175 potentially eligible documents, of which 54 were relevant to multi-morbidity. Among the 54 documents, 26, 17, and 11 were from India,^41–67^ South Africa,^68–84^ and Thailand,^85–95^ respectively (Online Supplemental Figure S1). The expert teams from South Africa and Thailand provided 14 documents in the review. The included documents had policies/programmes (n=11),^41,45,52,64,68,72,75,81,86,87,95^ operational or implementation or management guidelines (n=15),^42,46,48,54,57–59,69,73,78,84,91,93,94^ training manuals (n=12),^49–51,56,60–63,65,83,85,90^ action plans/frameworks/strategic plans (n=16),^43,44,47,53,55,70,71,74,76–80,82,88,89,92^ at the national level (Table 2). Two state-level NCD programmes from India were also included.^66,67^Table 2.Policy documents from India, Thailand, and South Africa.Sl. No.YearDocument titleResponsible organizationCountry12010,2013 revisedNational programme for prevention and control of cancer, diabetes, cardiovascular diseases and strokeMinistry of health and family welfareIndia22011Operational guidelines-National programme for health care of the elderlyNRHM, Ministry of health and family welfareIndia32012Twelfth Five-year plan (2012–2017)Planning Commission, government of IndiaIndia42012National action plan and monitoring framework for prevention and control of NCDsMinistry of health and family welfareIndia52016Operational framework management of common cancersMinistry of health and family welfareIndia62016Standard treatment guidelines- hypertension screening, diagnosis, assessment, and management of primary hypertension in adults in IndiaMinistry of health and family welfareIndia72016Operational guidelines on prevention, screening and control of common NCDsMinistry of health and family welfareIndia82016Training manual for medical Officers on reducing risk factors of NCDsMinistry of health and family welfareIndia92016Training manual for community health workers on reducing risk factors of NCDsMinistry of health and family welfareIndia102017National health policyMinistry of health and family welfareIndia112017National multi-sectoral action plan for prevention and control of common non-communicable diseaseMinistry of health and family welfareIndia122017National framework for Joint TB-diabetes collaborative activitiesMinistry of health and family welfareIndia132017Training manual for NCD programme managers at state and district levelMinistry of health and family WelfareIndia142017Hypertension screening, diagnosis, assessment, and management of primary hypertension in adults in IndiaMinistry of health and family welfareIndia152017Handbook for Counsellors - reducing risk factors for NCDsMinistry of health and family welfareIndia162018ICMR guidelines for management of type 2 diabetes 2018Indian Council for medical research (ICMR)India172019Guidelines for prevention and management of strokeMinistry of health and family welfareIndia18Not mentionedCPHC NCD solution PHC medical Officer User manualMinistry of health and family welfareIndia19Not mentionedCPHC NCD solution - NCD Application ANM User manualMinistry of health and family welfareIndia20Not mentionedModule for ASHA on non-communicable diseasesMinistry of health and family welfareIndia21Not mentionedModule for multi-purpose workers (MPW) - Female/Male on prevention, screening and control of common non-communicable diseasesMinistry of health and family welfareIndia22Not mentionedTraining module for staff nurses on population based screening of common non-communicable diseasesNational health Mission, Ministry of health and family welfareIndia23Not mentionedTraining module for medical officers for prevention, control and population level screening of NCDsMinistry of health and family welfareIndia24Not mentionedAyushman Bharat -comprehensive primary health care through health and wellness centresMinistry of health and family welfareIndia252017Non-communicable disease control programme (Amrutham Arogyam)-Kerala, IndiaNational health mission, KeralaKerala, India262021Makkalai Thedi Maruthuvam (Reaching out health services to people)Government of Tamil NaduTamil Nadu, India272009White paper for the transformation of the health system in South AfricaDepartment of health Republic of South AfricaSouth Africa282012Quality improvement – the key to providing improved quality of careDepartment of health Republic of South AfricaSouth Africa292013-2020National mental health policy framework and strategic planDepartment of health Republic of South AfricaSouth Africa302013Strategic plan for the prevention and control of non-communicable diseases (2013-17)Department of health Republic of South AfricaSouth Africa312015Implementation guideline of health workforce normative guides and standards for fixed primary health care facilitiesDepartment of health Republic of South AfricaSouth Africa322015National health insurance for South AfricaDepartment of health Republic of South AfricaSouth Africa332015-20Strategy for the prevention and control of obesity in South AfricaDepartment of health Republic of South AfricaSouth Africa342015-20Taxation of sugar-sweetened beveragesDepartment of health Republic of South AfricaSouth Africa352017National cancer strategic framework (NCSF)Department of health Republic of South AfricaSouth Africa362018Strengthening the South African health system towards an integrated and unified health systemDepartment of health Republic of South AfricaSouth Africa372019Policy framework and strategy for ward-based primary healthcare outreach teamsDepartment of health Republic of South AfricaSouth Africa382019-24National digital health strategy for South AfricaDepartment of health Republic of South AfricaSouth Africa3920202030 human resources for health strategy: Investing in the health workforce for universal health coverageDepartment of health Republic of South AfricaSouth Africa402020Referral policy for South African health services and referral implementation guidelinesDepartment of health Republic of South AfricaSouth Africa412020National strategic plan for the prevention and control of non-communicable diseases (2020-2025)Department of health Republic of South AfricaSouth Africa422021National user guide on the prevention and treatment of hypertension in adults at the PHC levelDepartment of health Republic of South AfricaSouth Africa43UnknownICSM model health service re-organizationDepartment of health Republic of South AfricaSouth Africa442013District health system management; to take care of the population: Elderly group, chronic disease group and people with disabilities^ a ^Health promotion foundation (Thai health), national health Security Office (NHSO)Thailand452013Guides to “Flat Belly” organizationNutrition Division, department of health, Ministry of public health, ThailandThailand462017Diabetes prevention and control service model high blood pressure to support the operation of NCDClinic plusBureau of non- communicable diseases, department of disease control, Ministry of public healthThailand4720175-Year national NCDs prevention and control planBureau of non-communicable diseases, department of disease control, ThailandThailand482017(Proposal) prevention and control of non-communicable diseases RTG-WHO country Co-Operation strategy January 2017–December 2021Department of disease control, Ministry of public health, ThailandThailand492017(Draft) Thailand healthy lifestyle strategic plan phase II 5-year non-communicable diseases prevention and control plan (2017-2021) and related action planBureau of non-communicable diseases, department of disease control, ThailandThailand502018Manual Tobacco addiction treatment in patients’ chronic disease in ThailandMedical professionals network for tobacco consumption controlThailand512020Guidelines for health system development (service plan) integrated primary care system with people at the centre (integrated, people-centred primary care)^ a ^(Ministry of public health, 2020)Ministry of public health, ThailandThailand522021Operational guidelines NCD clinic plus & Online^ a ^ (department of disease control, 2021)Division of non-communicable diseases, department of disease control, Ministry of public health, ThailandThailand53Not mentionedHandbook of integrated, people- centred health service in new normal diabetic and hypertensive clinic (for health care workers)^ a ^Thailand54Not mentioned(Medical practice) comprehensive service program for managing and caring for people with diabetes and related conditions in the national health Security system “practice guideline”Thailand^a^Google machine translated title from original in Thai language.Legend: NCDs= NRHM=National Rural Health Mission (India), ICMR= Indian Council of Medical Research, non-communicable disease, TB=Tuberculosis, CPHC= Comprehensive Primary Healthcare, PHC=Primary health centre, ANM=Auxiliary Nurse Midwife, ASHA=Accredited Social Health Activist, ICSM=Integrated Clinical Service Management (South Africa).
There were no policy documents specifically for NCD multi-morbidity. However, identified documents from the selected three countries addressed a few long-term NCDs and had policy directions for managing them (Online Supplemental Table S1). Policy documents did consider co-morbidities diabetes and hypertension, and guidance for health care providers (HCP) to screen or manage selected co-morbidities. For example, bi-directional screening for tuberculosis and diabetes has been recommended in India.^ 55 ^ However, none of the policies acknowledged or defined NCD multi-morbidity holistically.
While no policies explicitly acknowledged NCD multi-morbidity, there were findings from the policy documents that may be considered as potential strategies or policy actions that can be utilised to build an NCD multi-morbidity focus. The findings from the policy documents for a few NCDs have been presented under the three themes that helped to describe and highlight the gaps in policies: patient-level policy actions, healthcare provider-level policy actions, and health system-level policy actions (Table 3 and Online Supplement Table S2). Macro-level policy actions that have indirectly attempted to improve social determinants are interspersed within the appropriate themes.Table 3.Summary of policy actions at patient, health care provider and health system levels.Focus areaActionsDescriptionPatient-levelHealth information provision for individual NCDsFocused on health information provision for individual NCDs like diabetes, rather than comprehensive support for multi-morbidity. Activities include campaigns, leaflets, and community health worker delivered health information provisionsAssisted self-management supportCommunity health workers providing home monitoring of blood pressure and glucose, alongside education and counselling on healthy lifestyles for diabetes and hypertensionShared risk factor reductionActions aimed at reducing tobacco consumption, improving dietary practices, and enhancing physical activityMulti-sectoral action plansActions that promote inter-organisational cooperation for strategies to reduce risk factors such as collaboration with urban/transport departments to support physical activityHealth-care providerProvider-level training and capacity building for NCD managementTraining health care workers to screen for high blood pressure and blood glucose levelsOperational guidance for improving NCD care delivery through community-level roles and coordinationGuidance on organising and planning care for NCDs. Guidance on screening and management activities such as targeted high-risk group screening, dedicated NCD case managers to coordinate services within and outside hospitalsEnhancing human resources for healthcareActions focusing on improving human resource allocation based on needs, retention of trained health care staff and training of health care cadres on management of chronic conditionsHealth care systemStrengthening primary care and reorganising NCD care deliveryPrimary care strengthening to address growing NCDs through infrastructure, medicine availability, dedicated staff trained in NCDs and provision of electronic health recordsReorganising primary care through integrated models to manage both NCDs and communicable diseasesActions for managing chronic conditions, including mental health, epilepsy, asthma, hypertension, diabetes, COPD, HIV/AIDS, and TB by offering services for NCDs in clinics for HIV or TB.
Patient-level policy actions
At the patient-level, most activities in the policy documents were targeted at health information provision for individual NCDs such as diabetes rather than comprehensive and patient-centred self-management support aimed at NCD multi-morbidity. These health information/promotion activities included health care campaigns, distribution of patient information leaflets, and healthcare awareness through community health workers.^41,45,53,67,70,71,74,78,82,84–86,94^ South African NCD policy suggested an “assisted self-management support” where the community health care worker provides home monitoring of blood pressure and blood glucose in addition to education and counselling on healthy lifestyle behaviours intended to reduce risk factors such as overweight, tobacco cessation, etc., improving self-monitoring and medication adherence predominantly for diabetes and hypertension management.^78,82^ A similar programme called “Medicine at People’s Doorstep” or “Makkalai Thedi Maruthuvam” (MTM) was identified in Tamil Nadu, a state in India. This programme focused on home-based care and involved the delivery of drugs directly to the doorsteps of individuals aged 45 years and above who have hypertension and diabetes, as well as those with restricted or poor mobility.^ 67 ^
We identified policy documents from all three selected countries that focused on the shared risk factors and the preventive measures related to NCDs, such as policies on reducing tobacco consumption, better dietary practices, and improving physical activity.^44,46,47,49–51,53,56,57,59,62,63,65,66,75,82,87,89,91,92^ South Africa had a policy dedicated to reducing obesity.^ 74 ^ Similarly, we identified a strategy for improving physical activity in Thailand, which the WHO acknowledged as an essential step towards promoting physical activity.^ 96 ^ Furthermore, all three selected countries recognised the need for a multi-sectoral approach for health promotional activities related to NCDs in their policy documents. For example, the National Action Plan and Monitoring framework for preventing and controlling NCDs^ 48 ^ in India recognised the need to work with the urban department or transport department to create and preserve environments for supporting physical activity. Policies on reducing risk factors acknowledged poverty, lack of access for physical activity, and lack of social support as drivers for obesity and increasing tobacco consumption. For example, South African policy for reducing obesity has acknowledged poverty as a driver for obesity.^ 74 ^ However, the policy actions have been directed at improving awareness and suggestions for improving multi-sectoral co-ordination.
Healthcare provider-level policy actions
Most policy documents identified from the selected three countries for NCDs involved guidance or standards for healthcare providers and operational guidance for the main organisation-level activities to improve NCD care delivery. Of those policy documents from India addressing NCD management, provider-level activities pertained mainly to training and capacity building.^46–51,56–63,65,73,80,83,85,90–92,95^ We identified general guidance documents for training and actions to be carried out at the primary care level by the different cadres of health care providers from all three selected countries. For example, in India, the identified policy documents detailed guidance for training ASHAs (Accredited Social Health Activists) in screening for high blood pressure and blood glucose levels.^50,62^ Similarly, the role of village health volunteers in monitoring the self-measurement of blood pressure in high-risk groups was detailed in documents identified from Thailand. The use of NCD case managers of diabetes/hypertension clinics to coordinate and link services inside and outside hospitals were recommended in policy documents from Thailand.^ 85 ^ In South Africa, NCD policy recommended training of public health nurses on chronic conditions and community health workers for community level support.^77,82,84^ Furthermore, a policy document on improving the human resources for healthcare based on current and future needs was identified from South Africa.^ 80 ^
Health system level actions
At the health system or organisational level, policy documents detailing the directions to reorganise care for people with NCDs, strengthen primary care, and achieve universal health coverage have been identified from all three selected countries.^57,66,72,77,78,82,84,93,94^ However, the reorganisation focus was primarily on provisions of physical infrastructure, medicine availability at primary care levels, and incorporation of patient medical records at the facility level. Additionally, a focus on providing quality care was emphasised in some documents. For example, under the National Programme for Prevention & Control of Cancer, Diabetes, Cardiovascular Diseases & Stroke (NPCDCS), different states in India initiated various programmes to control and manage chronic diseases and their complications.^41,45,48^ The policy documents from the state of Kerala in India enabled actions to strengthen the health system (primary care) by establishing family health centres with enhanced infrastructure, availability of medicines for common chronic NCDs, and electronic health records for all patients.^ 66 ^ Furthermore, under the Ayushman Bharat programme (Government of India), the creation of health and wellness centres staffed with mid-level health providers was recommended for better prevention and coverage of NCDs.^57^Similarly in South Africa, a primary care reorganisation and strengthening initiative for managing chronic conditions was introduced as a pilot through the Integrated Chronic Disease Management (ICDM) model in 2011. The chronic diseases covered under the ICDM model include NCDs such as mental health conditions, epilepsy, asthma, hypertension, diabetes, and chronic obstructive pulmonary disease (COPD). Additionally, the model also addresses communicable diseases, encompassing HIV/AIDS and all forms of tuberculosis (TB). This initiative was further expanded to cover all primary care health services through Integrated Clinical Services Model.^82,84^
Discussion
We examined 54 current policies and guidelines from India, Thailand, and South Africa to identify how policies acknowledged and suggested policy directions for managing NCD multi-morbidity. We employed an analytical framework to review and organise the content of policies and guidelines available online. We found that all three countries addressed the management of NCDs, particularly diabetes and hypertension, at the primary care level and focused on strengthening and reorganising primary care for managing these conditions. Furthermore, all three countries had policies for addressing shared risk factors, such as tobacco use and physical inactivity, which are likely to impact the prevention and management of NCD multi-morbidity. However, certain differences also exist among the countries in their focus on risk factors. For instance, South Africa has a dedicated policy aimed at reducing obesity, Thailand adopts a targeted approach to address obesity reduction among the working population, and India emphasises an overall risk reduction approach for NCDs. Additionally, the policies from the selected three countries did not address any explicit improvement in social determinants of health to aid in the prevention and control efforts of NCD multi-morbidity.
None of the current policy review documents acknowledged NCD multi-morbidity beyond the co-occurrence of diabetes and hypertension. In a similar policy review comparing policies for multi-morbidity in the UK, Australia, and Sri Lanka, only the UK had a dedicated policy for multi-morbidity.^ 97 ^ One significant implication of the absence of a dedicated policy is the failure to recognise the significance of multi-morbidity as an issue. However, this is not to suggest that the presence of an approach would result in better outcomes, as previous studies looking at NCDs and health system preparedness found no association between policy and high-quality care outcomes.^98–100^ Considering that many LMICs are experiencing an epidemiological transition and grappling with chronic infectious diseases and NCDs, it was expected that there would be an acknowledgment of the coexistence of NCD multi-morbidity and a need for coordinated management efforts in its policy documents.
Without clear policies and management plans, several potential drawbacks may arise in NCD multi-morbidity prevention and control efforts in LMICs. Previous studies examining patient experiences with NCD multi-morbidity identified the increased workload involved, encompassing self-care management, intricate treatment modalities, behaviour change, and multiple clinic visits as barriers to effective care.^16,17^ Patients with multi-morbidity often face diminished capacity, including compromised physical and mental functioning, limited health literacy, and insufficient family and social support, resulting in suboptimal outcomes.^17,20^ Moreover, multi-morbidity is more prevalent among individuals from lower socioeconomic backgrounds, who frequently encounter resource constraints in effectively managing their health issues.^101–103^ Consequently, policies targeting multi-morbidity management in LMICs must account for the unique challenges patients face in these settings and formulate interventions that specifically address these challenges.^ 104 ^
Recognition of the need for self-management was evident in the NCD policies of all three countries. However, limited consideration was given to the complexities of self-management for patients with NCD multi-morbidity in these contexts, resulting in minimal tailored support. The United Kingdom NICE (National Institute for Health and Care Excellence) guidelines suggest that policy actions in multi-morbidity should strive to empower patients and facilitate self-management.^ 105 ^ Potential interventions could encompass digital reminders for medication and appointments, doorstep availability of medicines for elderly patients with chronic NCDs, outreach programs, and educational initiatives for improving awareness and tailored support for self-management.^106–109^
Strategies at the Healthcare provider level should include technical training and capacity building for healthcare workers.^ 110 ^ A shift towards an integrated generalist approach to healthcare is crucial, moving away from an excessive emphasis on specialised roles based on a country’s context and capacity. Policy actions should address human resource shortages and integrate frontline health workers into the formal healthcare system.^ 111 ^ Longer consultation times are necessary for patients with multi-morbidity, especially in deprived regions where individuals face higher mortality risks and a range of chronic conditions. If expanded beyond specific NCDs, Thailand’s case manager model could be a suitable framework for future management of NCD multi-morbidities.^92^Task-sharing strategies involving increased participation of health workers may enhance communication and provide tailored self-management support.^ 112 ^
At the organisation level, there is a need to transition towards designing better-integrated systems encompassing primary and secondary care, social support systems, and mental healthcare to reduce fragmentation of care.^113,114^ Developing an integrated system requires attention to workforce planning in LMIC settings.^8,113^ Integrated clinical algorithms, standardised clinic stationery, and reorganised clinic flows may improve care delivery efficiency for managing NCD multi-morbidity.^ 36 ^ Previous studies from South Africa have shown that better staff support and leadership is needed for integrated models to be sustainable.^115–118^ Strategies to enhance the skills among generalist healthcare professionals and the establishment of integrated chronic disease teams to provide minimally disruptive care to individuals with multi-morbidity should be prioritised in primary care settings.
One of the overarching findings from the analysis is that all three countries have implemented policy measures to prevent various risk factors associated with NCDs. To enhance the comprehensiveness of these policies, it could be valuable to include specific components that acknowledge shared risk factors, particularly behavioural determinants contributing to NCD multi-morbidity.^ 12 ^ For instance, obesity increases the likelihood of both osteoarthritis and type 2 diabetes.^ 119 ^ Specific policies targeting shared risk factors, such as policies on physical activity in Thailand and obesity prevention policies in South Africa, may be adopted for India and other LMICs.^45–47^ Preventing multi-morbidity in LMICs requires population-level structural changes in policies that go beyond individual behaviour change strategies, addressing risk factors within the specific socioeconomic-political context, including interventions targeting the food system and built environment to reduce socioeconomic inequalities.^120,121^
At the policy level, there is a notable absence of recognition regarding the coexistence of multiple NCDs and their adverse interactions. Such negative interactions may even affect the health and well-being of the affected individual’s family members with multi-morbidity. Social determinants of health play a vital role in such clustering of chronic conditions and their interactions.^ 122 ^ To adopt a comprehensive perspective, it is necessary to move beyond narrow approaches such as the co-occurrence of conditions and develop an all-inclusive understanding of disease clustering, interactions, and their biological, ecological, and social contexts. Ultimately, this approach calls for comprehensive public health policies that address the underlying causes of diseases.^ 123 ^
Limitations
Our search may have missed policy documents that are not publicly available and in regional languages. While we engaged with experts from each country to gather relevant documents, we might have missed some. Second, we have considered only policy content analysis rather than the health care system implementation and delivery in each country. This review is a first step in identifying and highlighting the lack of policies dedicated to multi-morbidity in LMICs.
Conclusion
The research examined the current policies, approaches, and deficiencies for people with multiple long-term conditions in three LMICs. The primary results indicate that all the selected three countries prioritise preventative measures such as screening, identifying risk factors, and promoting healthy behaviours to combat NCDs. Nevertheless, they fall short in acknowledging the impact of NCD multi-morbidity and its effective management in primary care settings. There is a lack of appreciation of the social determinants of health and strategies to tackle them to prevent and control multi-morbidity in the existing policies.
Supplemental Material
Supplemental Material - Non-communicable disease multi-morbidity in policies from India, Thailand, and South Africa: A comparative document reviewSupplemental Material for Non-communicable disease multi-morbidity in policies from India, Thailand, and South Africa: A comparative document review by Linju Joseph, Rakhal Gaitonde, Charutha Retnakumar, Athira Krishnan, Thoniparambil Ravindranathanpillai Lekha, Neethu Sasidharan, André van Rensburg, Naomi Levitt, Nilawan Upakdee, Jissa Vinoda Thulaseedharan Mathew Joseph Valamparampil, Sivadasanpillai Harikrishnan, Sheila Greenfield, Paramjit Gill, Justine Davies, Semira Manaseki-Holland and Panniyammakal Jeemon in Journal of Multimorbidity and Comorbidity
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Global Health Estimates . Life Expectancy and leading causes of death and disability. https://www.who.int/data/gho/data/themes/theme-details/GHO/mortality-and-global-health-estimates (2019, accessed 15 January 2023).
- 2United Nations . World population prospects: The 2017 revision. https://desapublications.un.org/publications/world-population-prospects-2017-revision (2017, accessed 10 January 2023).
- 3Mc Phail SM . Multi-morbidity in chronic disease: impact on health care resources and costs. Risk Manag Health Policy 2016; 9: 143–156.10.2147/RMHP.S 97248 PMC 493999427462182 · doi ↗ · pubmed ↗
- 4Pati S Agrawal S Swain S , et al. Non communicable disease multimorbidity and associated health care utilization and expenditures in India: cross-sectional study. BMC Health Serv Res 2014; 14: 451.25274447 10.1186/1472-6963-14-451PMC 4283077 · doi ↗ · pubmed ↗
- 5Sudharsanan N Bloom DE . The Demography of Aging in Low- and Middle-Income Countries: Chronological versus Functional Perspectives. Future Directions for the Demography of Aging: Proceedings of a Workshop 2018. https://www.ncbi.nlm.nih.gov/books/NBK 513069/ (accessed on 15 January 2023).
- 6Kruk ME Nigenda G Knaul FM . Redesigning primary care to tackle the global epidemic of noncommunicable disease. Am J Public Health 2015; 105(3): 431–437.25602898 10.2105/AJPH.2014.302392 PMC 4330840 · doi ↗ · pubmed ↗
- 7Boutayeb A . The double burden of communicable and non-communicable diseases in developing countries. Trans R Soc Trop Med Hyg 2006; 100(3): 191–199.16274715 10.1016/j.trstmh.2005.07.021 · doi ↗ · pubmed ↗
- 8Oni T Unwin N . Why the communicable/non-communicable disease dichotomy is problematic for public health control strategies: implications of multi-morbidity for health systems in an era of health transition. Int Health 2015; 7(6): 390–399.26103981 10.1093/inthealth/ihv 040PMC 4638105 · doi ↗ · pubmed ↗