Validating the socio-spiritual items of the Utrecht Symptom Diary—4 Dimensional: Content and construct validity
Tom Lormans, Everlien de Graaf, Frederieke van der Baan, Carlo Leget, Saskia Teunissen

TL;DR
The study confirms that the socio-spiritual items of the USD-4D accurately measure what they are intended to in palliative care patients.
Contribution
The study validates the socio-spiritual items of the USD-4D for use in clinical palliative care.
Findings
At least 80% of participants found the items comprehensible and relevant.
About half of the respondents identified missing items in the USD-4D.
For every item, at least 75% of hypotheses were confirmed, except one.
Abstract
The Utrecht Symptom Diary—4 Dimensional (USD-4D) is a multidimensional Patient-Reported Outcome Measure to monitor symptoms and needs and increase patients’ self-efficacy. Assessing the content and construct validity of the USD-4D ensures it accurately measures the intended construct and is contextually relevant. This study aimed to assess the content and construct validity of the socio-spiritual items of the USD-4D in a population of Dutch patients in the palliative phase of their illness. A multiple method study was performed consisting of a cross-sectional survey and an observational cohort study. The study population consisted of (a) healthcare providers working with patients in the palliative phase and (b) a cohort of patients with a life limiting illness in all settings supplemented by a cohort of hospice patients. At least 80% of participants positively assessed the items…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
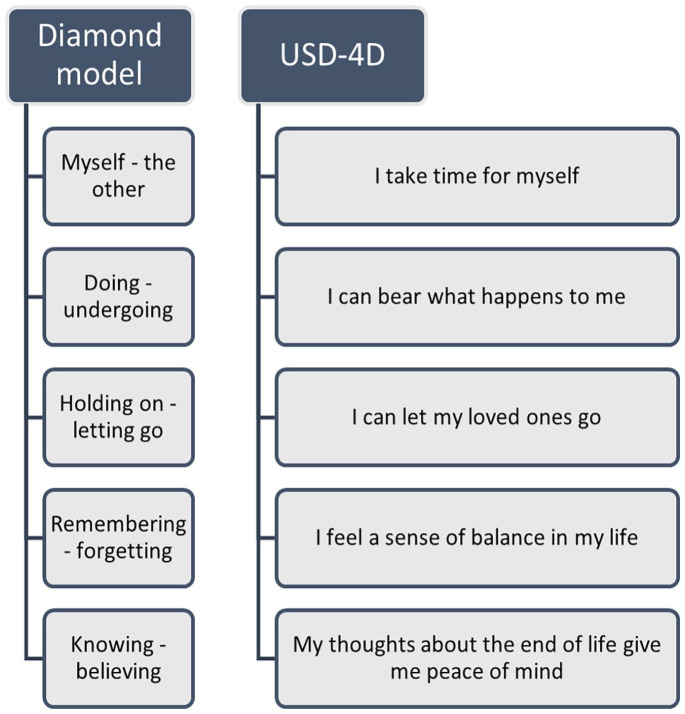 Figure 1
Figure 1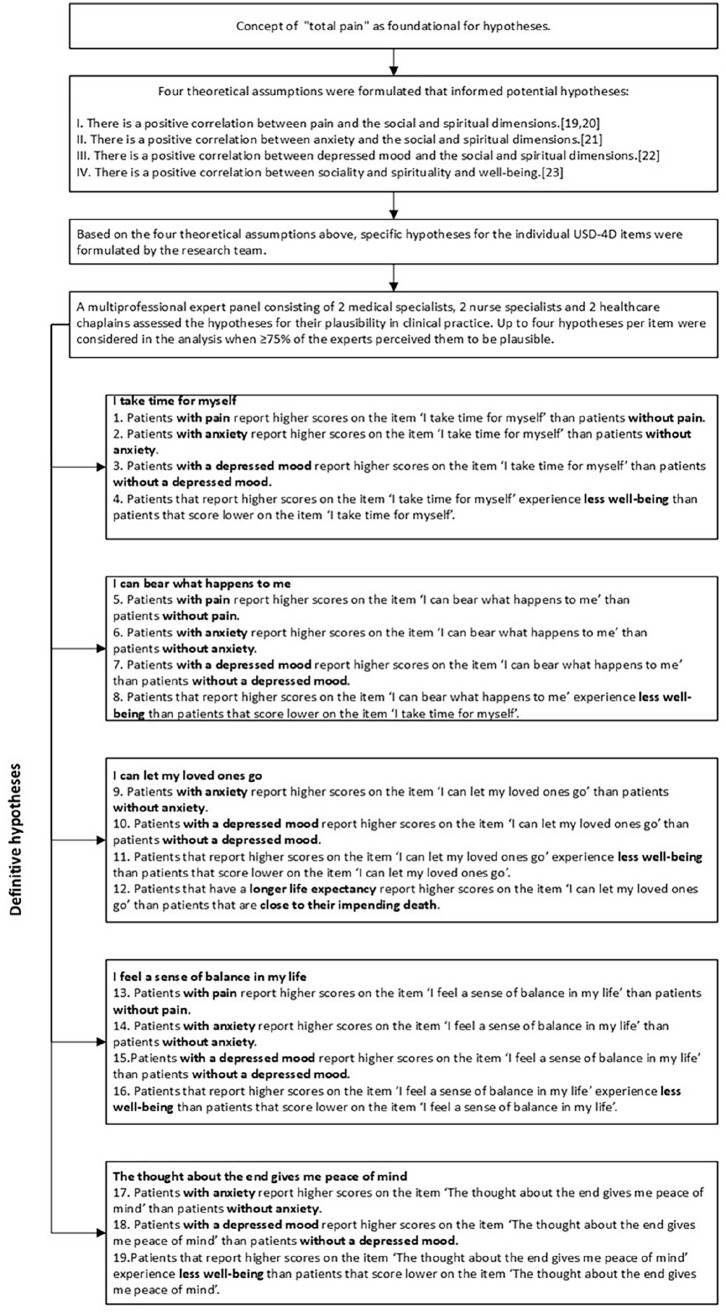 Figure 2
Figure 2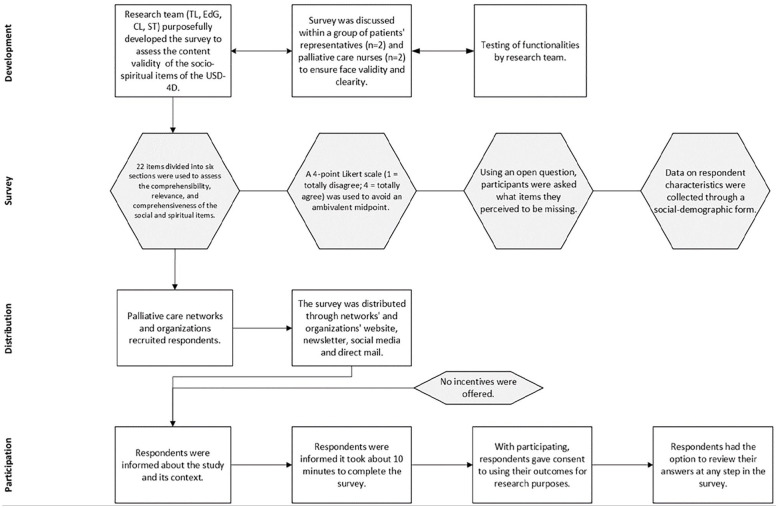 Figure 3
Figure 3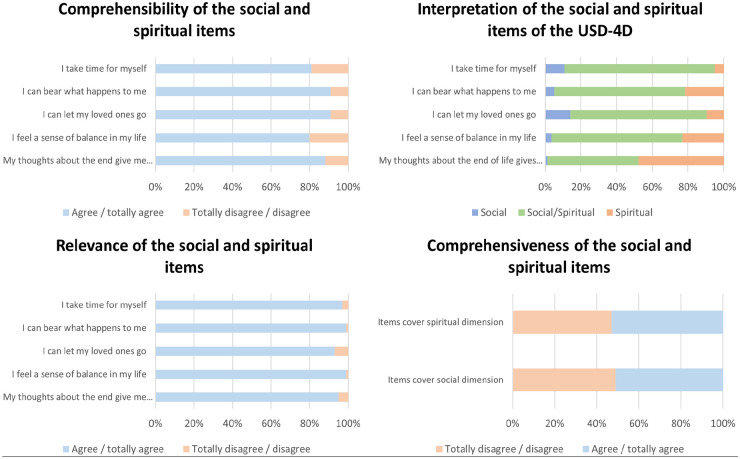 Figure 4
Figure 4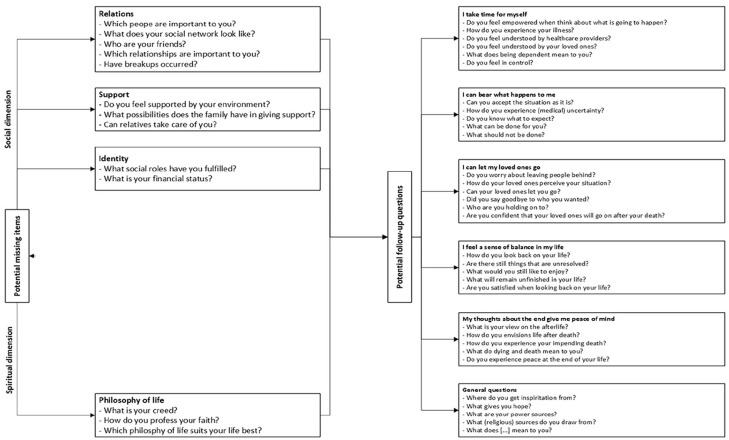 Figure 5
Figure 5- —zonmwhttps://doi.org/10.13039/501100001826
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPalliative Care and End-of-Life Issues · Cancer survivorship and care · Grief, Bereavement, and Mental Health
Introduction
Patients with life-limiting illnesses face multidimensional symptoms and needs that require personalized care to maintain quality of life.^1 ?–3^ Patient-Reported Outcome Measures (PROMs) support symptom management by incorporating patients’ assessments of their symptom severity,^2,3^ alleviating suffering and improving well-being.^ 4 ^
The Edmonton Symptom Assessment System (ESAS) is a widely used PROM for physical and psychological symptoms.^5,6^ In the Netherlands, its adapted version, the Utrecht Symptom Diary (USD), fulfills a similar role.^ 7 ^ However, the social and spiritual dimensions of care fall outside of the scope of these PROMs and often remain insufficiently addressed in clinical practice.^8,9^
PROMs like the Social Difficulties Inventory (SDI),^ 10 ^ Functional Assessment of Chronic Illness Therapy—Spiritual Well-Being (FACIT-Sp),^ 11 ^ and Spiritual Needs Assessment for Patients (SNAP)^ 12 ^ focus on the social and spiritual dimensions. However, they are time-intensive, lack holistic scope, and are most effective when specific needs are already identified and the social and spiritual dimensions must be explored further.
To address this gap, the USD was expanded into the Utrecht Symptom Diary—4 Dimensional (USD-4D), incorporating five socio-spiritual items based on the Diamond Model.^ 13 ^ The Diamond Model is a validated tool that helps patients and healthcare providers discuss social and spiritual issues.^14,15^ It centers on the concept of “inner space,” a state of mind connecting individuals to their emotions and attitudes. Its five polarities have been adapted into five USD-4D items that reflect social, spiritual, or both dimensions, depending on the patient’s perspective, see Figure 1.^ 9 ^ Now, the USD-4D’s 21 items, scored on an 11-point intensity scale, allow patients to prioritize multidimensional symptoms and needs, fostering autonomy and patient-centered care (Appendix 1).
The anthropological polarities of the diamond model and their respective operationalized items in the USD-4D.
The USD-4D has been implemented in Dutch healthcare, showing feasibility in addressing patients’ symptoms, wishes, and needs.^ 16 ^ Its socio-spiritual items were validated by patients for comprehensiveness, relevance, and clarity.^ 17 ^ However, content validity from the healthcare providers perspective and construct validity, how well the PROM measures its intended constructs, remain to be evaluated.^18,19^
This study aims to assess the content validity of the USD-4D from healthcare providers’ perspectives and evaluate the construct validity of its socio-spiritual items in Dutch patients facing life-limiting illness.^ 19 ^
Methods
This observational, multi-method study addressed two aims: (1) content validity was assessed via a cross-sectional online survey of healthcare providers (October 2020–August 2021); and (2) construct validity was evaluated in 2022 through a cohort study using the USD-4D, completed by patients with a life expectancy under 1 year.
The study adhered to the Checklist for Reporting Results of Internet E-Surveys (CHERRIES)^ 20 ^ as well as the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines^ 21 ^ to ensure reporting rigor.
Population and setting
Content validity
A convenience sample of healthcare providers working in palliative care were invited to participate based on accessibility. The sample included nurses, physicians, social workers, chaplains, and volunteers aged 18 or older across various settings (hospital, nursing home, home, hospice). Participants were selected through palliative care organizations. Prior experience with the USD-4D was not required. The goal was to recruit at least 15 healthcare providers per discipline and setting for a diverse, representative sample.
Construct validity
Two patient cohorts in the palliative phase were included:
SYMPAL Cohort: Established in 2009, this hospice-based cohort includes patients aged 18 or older with an estimated life expectancy under 3 months. Participants had self-completed at least one USD-4D during their admission.MuST-PC Cohort: Includes patients aged 18 or older with an estimated life expectancy under 1 year, assessed using the “surprise question” (“Would I be surprised if this patient died in the next 12 months?” with a “No” response). Participants self-completed a USD-4D for this study.
Ethical issues
This study followed the Declaration of Helsinki and General Data Protection Regulation to ensure ethical conduct and data protection. The UMC Utrecht institutional review board determined the research was exempt from the WMO (decisions 18-499/C, July 2018, and 19-602/C, 2019). Similarly, the University Medical Center Groningen concluded the MuST-PC cohort study was outside WMO’s scope (decision 2018/307).
Study outcome
Content validity
The study outcome was the content validity of the socio-spiritual items of the USD-4D as perceived by healthcare providers (Table 1).
Table 1.: Aspects of content validity. 22 .
Construct validity
The outcome of this study was the assessment of the construct validity of the socio-spiritual items within the USD-4D. Each of the five socio-spiritual items was treated as a distinct construct, and consequently, the construct validity of each item was evaluated through hypothesis testing.^ 19 ^ At the basis of the formulation of the hypotheses laid the concept of “total pain”: “the suffering that encompasses all of a person’s physical, psychological, social, and spiritual struggles.”^ 23 ^ In other words, social and spiritual well-being affects and is affected by physical and psychological symptoms and needs and vice.^24 ???–28^
For all items except one, four hypotheses were developed. For the final item, “The thought about the end gives me peace of mind,” three hypotheses were formulated (Figure 2). Following the COSMIN methodology, construct validity for an item was confirmed when at least 75% of the formulated hypotheses for that item were confirmed. For the item with only three hypotheses, a cut-off of 66% was applied to establish construct validity.^ 19 ^
Flowchart of hypotheses-development.
Data collection
Content validity
Data were collected using a Survey Monkey-based survey designed for this study. The survey included 22 items evaluating the comprehensibility, relevance, and comprehensiveness of the USD-4D socio-spiritual items, rated on a four-point Likert scale (“totally disagree” to “totally agree”). An open-ended question invited suggestions for missing items, and additional questions captured respondent characteristics. The survey link was openly shared, ensuring broad access while maintaining participant anonymity by collecting no identifiable information.
Figure 3 outlines the survey’s development, distribution, and participation process.
Development, distribution, and participation process of the survey.
Construct validity
For all hypotheses except hypothesis 12, only the first completed USD-4D per patient was analyzed. If multiple USD-4Ds were available, only the earliest was selected. For hypothesis 12, paired USD-4D scores were created for each patient, consisting of the first completed USD-4D and one completed within 2 weeks before death.
Statistical analysis
Content validity
Data from the online survey program were automatically imported into IBM SPSS 26 for analysis.^ 29 ^ Descriptive statistics (frequencies, mean, SD, and range) summarized respondents’ characteristics. Missing items identified by healthcare providers were analyzed using content analysis.
The Item-level Content Validity Index (I-CVI) was calculated for each item. Responses were dichotomized: “agree and totally agree” (scores 3 and 4) or not (scores 1 and 2). The I-CVI was then computed as the proportion of positive responses (“agree” and “totally agree”) out of the total responses, with values >0.8 considered excellent.^ 22 ^
Construct validity
Before analysis, data from the two cohorts were reorganized and recoded into similar variables. Age was categorized as an ordinal variable, consistent with the MuST-PC cohort.
Most hypotheses and theoretical assumptions focused on the absence versus prevalence of symptoms. To assess the alignment of USD-4D scores with these hypotheses, items were dichotomized into “no symptoms” (score = 0) and “severe symptoms” (score ⩾6). However, “well-being” was treated as a continuous variable, in line with previous research, and not dichotomized.^ 30 ^
Statistical tests included:
Chi-squared test: For hypotheses on dichotomized items (e.g., pain, anxiety, depressed mood).Mann–Whitney U test: For hypotheses on “well-being,” as it was not normally distributed and involved unpaired continuous variables.Wilcoxon signed-rank test: For paired analysis of the first and last USD-4D scores in hypothesis 12.
A hypothesis was confirmed when tested significant with p ⩽ 0.05.
Patient characteristics were summarized using descriptive statistics: mean and range or median and interquartile range for continuous data, and numbers and percentages for ordinal or dichotomous data. Analyses were conducted using SPSS Statistics 26.^ 29 ^
Results
Content validity
The online survey was completed by 601 healthcare providers, with 24 excluded as they did not provide palliative care. The final analysis included 577 respondents, predominantly female (88%), with a mean age of 48 years (range: 21–67). Most were nurses (51%). Table 2 summarizes their characteristics.
Table 2.: Respondents’ characteristics content validity.
The socio-spiritual reflection in the USD-4D is recognized by 51%–84% of the respondents. Only the item “My thoughts about the end of life, give me peace of mind” is considered either socio-spiritual (51%) or spiritual (48%).
Figure 4 summarizes results for comprehensibility, relevance, and comprehensiveness.
The results for the comprehensibility, relevance and comprehensiveness of the socio-spiritual items.
Comprehensibility of the USD-4D items was excellent, with I-CVI scores between 0.80 and 0.91. Relevance scored even higher, with I-CVI values ranging from 93% to 99%.
Approximately 51% of respondents rated the social dimension as comprehensive, and 53% rated the existential dimension similarly. However, half indicated that some items were missing for full coverage of these dimensions. Qualitative analysis of open-ended responses identified two themes: questions related to medical history and follow-up on the Diamond Model’s polarities (Figure 5). While these are important, they fall outside the USD-4D’s goal.
Potential missing items and potential follow-up questions.
Overall, the content validity of the USD-4D was confirmed.
Construct validity
A total of 897 patients (53% female, aged 68–80) completed at least one USD-4D across various care settings. Most patients had a cancer diagnosis (82%) and received hospice care (85%). Table 3 summarizes their characteristics.
Table 3.: Respondents’ characteristics construct validity.
All hypotheses except one (hypothesis 12) were statistically significant. With 75%–100% of hypotheses confirmed per item, the construct validity of the socio-spiritual items was established (Tables 4 and 5).
Table 4.: Hypothesis testing of the socio-spiritual items of the USD-4D—pain, anxiety, depressed mood, and time to death.
Table 5.: Hypothesis testing of the socio-spiritual items of the USD-4D—well-being.
Discussion
This study assessed the content and construct validity of the socio-spiritual items in the USD-4D. From healthcare providers’ perspectives, the items demonstrated strong content validity, with I-CVI scores of 0.8–0.93 for comprehensibility and relevance. Most healthcare providers recognized these items as addressing both social and spiritual dimensions, although about 50% felt certain items were missing. However, the suggested additions were outside the USD-4D’s purpose of monitoring concern severity over time. At least 75% of hypotheses per item were confirmed, with 18 of 19 hypotheses validated. Thus, the USD-4D’s content and construct validity are affirmed.
The USD-4D, now a validated multidimensional PROM, can be used to effectively monitor patients’ symptoms and needs and facilitate patient-driven dialogue, supporting care tailored to their values and wishes. Content validity is particularly crucial for multidimensional PROMs, like the USD-4D, that do not focus on a single construct.^ 31 ^ Unlike PROMs such as the SDI,^ 10 ^ FACIT-SP12,^ 11 ^ and SNAP,^ 12 ^ which categorize items strictly within spiritual or social domains, the USD-4D adopts a flexible approach, allowing patients to articulate needs without rigid definitions. This flexibility aligns with research indicating that patients often use overlapping language for social and spiritual needs, promoting a holistic understanding.^ 9 ^
With only five socio-spiritual items, the USD-4D is not exhaustive but serves as a starting point to identify care needs through patient-driven dialogue. These items, derived from the Diamond Model’s polarities, are broad in scope to accommodate diverse interpretations, requiring healthcare providers to skillfully facilitate discussions to clarify and address patient concerns.^ 17 ^ Studies have shown that patients’ interpretations align well with the intended polarities, supporting the items’ validity while maintaining their adaptability.
The USD-4D is not designed to measure a single predefined construct, posing challenges for assessing construct validity. Despite this, combining theoretical frameworks and expert insights enabled hypothesis testing, validating the socio-spiritual items. The study deliberately avoided evaluating convergent validity due to the subjective and multifaceted nature of the social and spiritual dimensions, which complicates correlations with other instruments. This decision highlights the USD-4D’s unique role in capturing nuanced patient perspectives within these dimensions.
Strengths and limitations
This study’s strength in assessing content validity lies in the large response rate from HCPs and the representative distribution of respondents, reflecting clinical practice where the USD-4D is used. Generalist and specialist HCPs, especially nurses who primarily use the USD-4D in palliative care, were well represented. A multidisciplinary research team, comprising nurses, a chaplain, and an ethicist, enhanced data analysis and ensured conclusions aligned with clinical practice.
Some limitations should be considered. Data were collected exclusively through surveys, without focus groups as recommended by COSMIN methodology. However, the large sample size and consensus in responses suggest surveys were sufficient for evaluating content validity. Participants were mainly female (88%), which reflects national numbers and thus will not skew the validity measure.^ 32 ^ Additionally, 42% of respondents practiced religion, differing from national averages, but sensitivity analysis indicated no effect on results. Moreover, we did not study participants’ interpretation of spirituality. Physician, medical specialist, and social worker participation was lower, but primary end-users were well represented.
This study is the first to assess the construct validity of the USD-4D’s socio-spiritual items among Dutch palliative patients across care settings. Hypotheses were formed through literature and interprofessional collaboration, enhancing their relevance. Despite limited data from hospital and home care settings, results were robust for hospice settings, with 75% of hypotheses confirmed. The unconfirmed hypothesis on “I can let go of my loved ones” may reflect a lack of data from patients near death, as they typically do not complete the USD-4D in their final days.
Implications for clinical practice
The validated content and construct of the USD-4D’s socio-spiritual items support its use as a reliable PROM in clinical practice. It is important to note that while these findings confirm the items’ accuracy and alignment with relevant hypotheses, they do not constitute formal proof or evidence of causality. Compared to other international PROMs focusing on the social and spiritual dimensions, the USD-4D has proven to be a clinically feasible PROM to monitor and facilitate dialogue on patients’ multidimensional symptoms and needs and foster holistic palliative care. After culturally sensitive translation and cross-cultural validation the USD-4D warrants international use.
For meaningful interpretation, ongoing dialogue between patients and healthcare providers is essential. The USD-4D should be integrated into clinical palliative care as more than a tool, becoming part of multiprofessional workflows and supported by continuous skill development for healthcare providers.
Implications for future research
This study focused on an autochthonous Dutch palliative care population. To ensure the USD-4D’s effectiveness in other cultures, future research should address cross-cultural validity. Further development is also needed for its use outside palliative care or with cognitively impaired patients.
Validation is an ongoing process, requiring continuous refinement as understanding of the constructs and empirical evidence grows. Future studies should further validate the USD-4D in diverse contexts, settings, and populations while also re-evaluating the underlying theories supporting the instrument.^ 12 ^
Conclusion
This study confirmed the content validity from healthcare providers’ perspectives and construct validity of the USD-4D’s socio-spiritual items, showing it effectively measures its intended constructs. By reliably monitoring multidimensional symptoms and needs, the USD-4D supports patient-centered palliative care. Furthermore, it shows how clinically feasible PROMs can be structurally used. It also highlights the need for patient-driven research into socio-spiritual well-being, emphasizing tools sensitive to the complex needs of patients facing a life-limiting illness without being too elaborate.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Teunissen S. In palliative care symptoms mean everything. Symptoms & symptom management in palliative care for cancer patients. Utrecht: Utrecht University, 2007.
- 2Richardson A Medina J Brown V , et al. Patients’ needs assessment in cancer care: a review of assessment tools. Support Care Cancer 2007; 15: 1125–1144.17235503 10.1007/s 00520-006-0205-8 · doi ↗ · pubmed ↗
- 3Tian L Cao X Feng X. Evaluation of psychometric properties of needs assessment tools in cancer patients: A systematic literature review. P Lo S One 2019; 14: e 0210242.10.1371/journal.pone.0210242 PMC 632483330620770 · doi ↗ · pubmed ↗
- 4Litchfield I Greenfield S Turner GM , et al. Implementing PRO Ms in routine clinical care: a qualitative exploration of GP perspectives. BJGP Open 2021; 5: 101135.10.3399/bjgpopen 20X 101135 PMC 796052633199306 · doi ↗ · pubmed ↗
- 5Hui D Bruera E. The Edmonton Symptom Assessment System 25 years later: past, present, and future developments. J Pain Symptom Manage 2017; 53: 630–643.28042071 10.1016/j.jpainsymman.2016.10.370PMC 5337174 · doi ↗ · pubmed ↗
- 6Bruera E Kuehn N Miller MJ , et al. The Edmonton Symptom Assessment System (ESAS): a simple method for the assessment of palliative care patients. J Palliat Care 1991; 7: 6–9.1714502 · pubmed ↗
- 7Van der Baan FH Koldenhof JJ Nijs EJ , et al. Validation of the Dutch version of the Edmonton Symptom Assessment System. Cancer Med 2020; 9: 6111–6121.32643871 10.1002/cam 4.3253 PMC 7476846 · doi ↗ · pubmed ↗
- 8Best M Butow P Olver I. Why do we find it so hard to discuss spirituality? A qualitative exploration of attitudinal barriers. J Clin Med 2016; 5: 77.27598212 10.3390/jcm 5090077 PMC 5039480 · doi ↗ · pubmed ↗