Effect of Tofacitinib on Hemostasis in Patients with Ulcerative Colitis: A Comparative Ex Vivo Study
Cristina Sánchez-Sánchez, Fabio Suarez-Trujillo, Cristina Ramírez, Irene Soleto, Jorge Mercado, Macarena Orejudo, Paula J. Martínez, Celia Rubio Collado, Mar Orts, María Jesús Rubio Franco, Antonio Planas, Natalia Acedo, Nora Butta, María Chaparro, Javier P. Gisbert

TL;DR
This study compares how tofacitinib and anti-TNF drugs affect blood clotting and platelet function in ulcerative colitis patients and healthy individuals.
Contribution
The study provides novel ex vivo evidence that tofacitinib does not alter platelet function or coagulation in UC patients compared to anti-TNF.
Findings
Tofacitinib and anti-TNF similarly increased platelet activation markers in UC patients and healthy controls.
No differences in platelet aggregation or coagulation parameters were observed between tofacitinib, anti-TNF, and no drug.
The increased thromboembolic risk with tofacitinib cannot be attributed to platelet or coagulation changes in UC patients.
Abstract
Background: Tofacitinib is effective for refractory ulcerative colitis (UC), a chronic inflammatory disease of the colonic mucosa. However, its use has been associated with an increased risk of thromboembolic events, prompting regulatory restrictions. Understanding the pathophysiological mechanisms contributing to these potential risks is critical for patient safety. We aim to evaluate and compare ex vivo the effects of tofacitinib and anti-TNF on coagulation parameters and platelet function. Methods: Whole blood and platelet-rich plasma from 10 active UC (aUC) and 10 quiescent UC (qUC) patients and 10 healthy controls (HC) were spiked ex vivo with tofacitinib, anti-TNF (as comparator), or a sterile solution. Coagulation kinetics were measured by rotational thromboelastometry (ROTEM), platelet aggregation by aggregometry, and platelet activation by flow cytometry. The study was…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
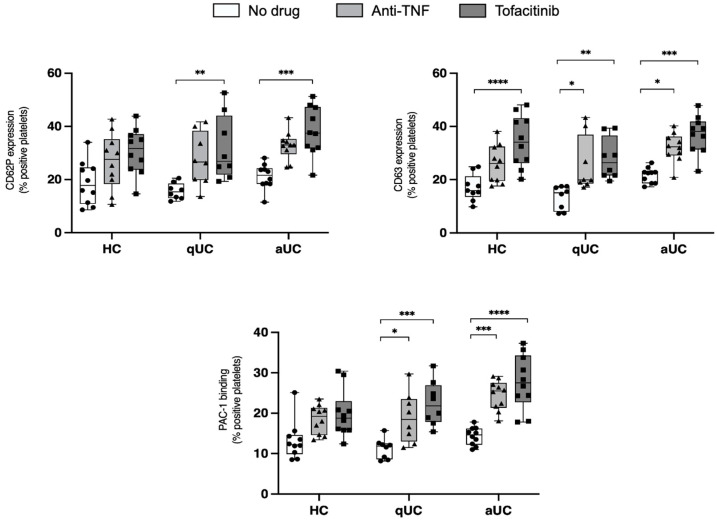 Figure 1
Figure 1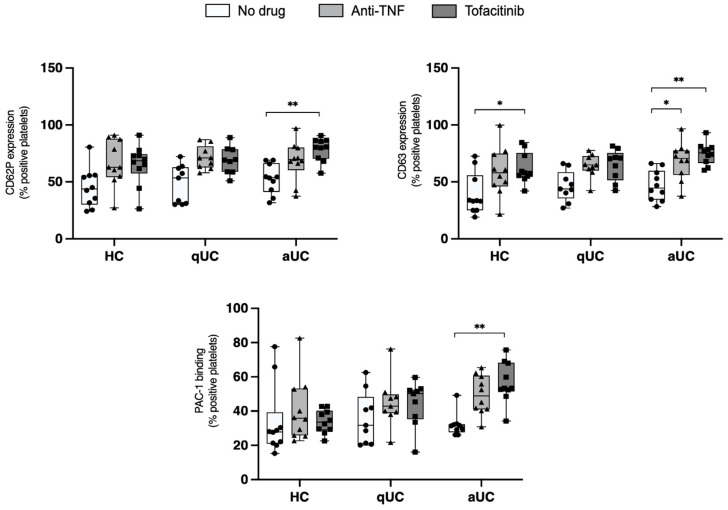 Figure 2
Figure 2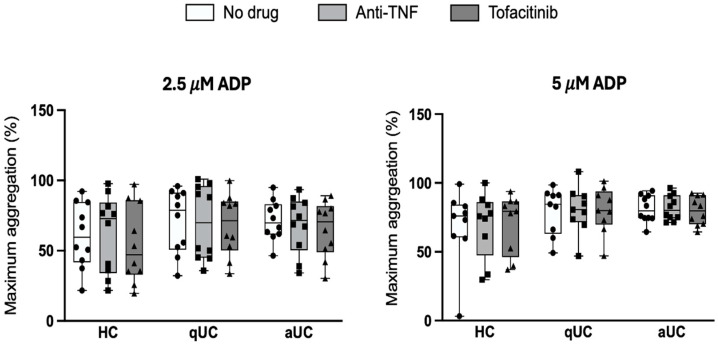 Figure 3
Figure 3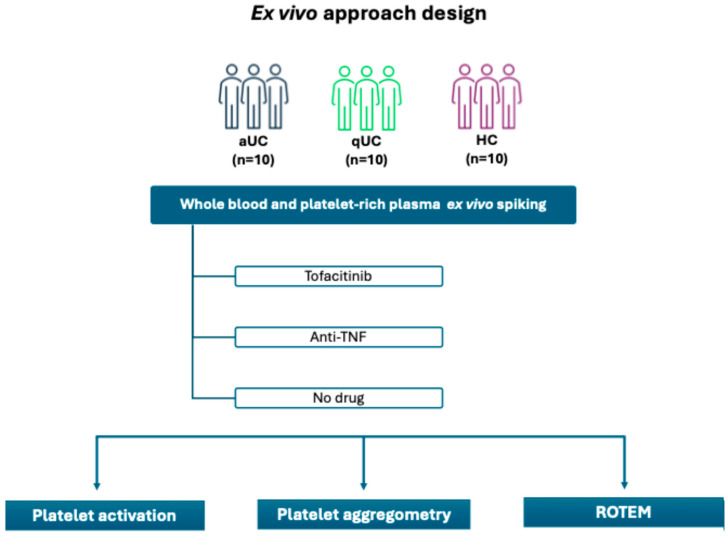 Figure 4
Figure 4- —Pfizer Inc. ASPIRE program
- —Instituto de Salud Carlos III
- —Plan Estatal de Investigación Científica y Técnica y de Innovación
- —ISCIII—Subdirección General de Evaluación y Fomento de la Investigación
- —European Regional Development
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsInflammatory Bowel Disease · Systemic Lupus Erythematosus Research · Biosimilars and Bioanalytical Methods
1. Introduction
Ulcerative colitis (UC) is a chronic inflammatory disease of the colonic mucosa that typically starts in the rectum and extends proximally [1,2]. Clinical manifestations include bloody diarrhea, abdominal pain, and extra-intestinal manifestations [3]. UC’s etiology is unknown but involves genetic, environmental, and immune factors. While first-line treatments include salicylates, immunosuppressive drugs, and corticosteroids, moderate-to-severe cases often require biologic therapies [4]. However, approximately 50% of patients do not achieve clinical remission with these agents [5].
Tofacitinib is an oral small-molecule Janus kinase (JAK) inhibitor that has become a therapeutic option for refractory UC cases [6]. Initially approved for rheumatoid arthritis and psoriatic arthritis, it has demonstrated effectiveness in both inducing and maintaining remission in UC patients. However, the safety profile of tofacitinib raises significant concerns. Its use in patients with rheumatoid arthritis has been associated with an increased risk of thromboembolic events, including pulmonary embolism and deep vein thrombosis [7]. In particular, data from ORAL SURVEILLANCE in patients diagnosed with rheumatoid arthritis aged over 50 years with cardiovascular risk factors indicated a higher incidence of pulmonary embolism and venous thrombosis among patients treated with tofacitinib compared those treated with anti-tumor necrosis factor (TNF) agents [8]. More recent analyses have further refined the risk assessment, identifying two distinct subpopulations of tofacitinib with different relative risks when compared to TNF inhibitors [9]. Furthermore, studies from a large randomized cardiovascular safety trial and an extended analysis of phase 3b/4 safety data demonstrated a higher incidence of major adverse cardiovascular events and cancer in patients with rheumatoid arthritis receiving tofacitinib compared to anti-TNF [10,11].
Due to the increased risk of severe thromboembolic events, the European Medicines Agency (EMA) and the United States Food and Drug Administration (US FDA) have issued warnings advising against the long-term use of tofacitinib for maintenance in UC patients with one or more risk factors for venous thromboembolism [12,13]. In cases where no appropriate alternative treatments are available, the risk and benefits of tofacitinib should be carefully evaluated before its long-term use is considered. Additionally, other JAK-signal transducer and activator of transcription (STAT) pathway inhibitors such as baricitinib have also been associated with an increased risk for thromboembolic events, suggesting a potential class effect of JAK inhibitors [14].
JAK inhibitors target the JAK and STAT pathway, which is crucial for signal transduction and transcriptional activation. This pathway plays a key role in various cytokines and growth factors, and is essential for hematopoiesis, inflammation, and immune functions [15]. The JAK-STAT pathway mediates over 50 signaling molecules, including cytokines, hormones, and growth factors [16]. Given the broad impact of JAK inhibitors on this pathway, their use may disrupt the balance between prothrombotic and antithrombotic effects, potentially leading to thrombotic complications and cardiovascular events [17]. Some studies suggest that JAK inhibition may reduce endothelial prothrombotic activation and leukocyte–endothelial proadhesive interactions [18]. However, other research highlights that JAK inhibitors may increase cytokine production associated with immunothrombosis and delay clot lysis, particularly in active rheumatoid arthritis [19]. Further studies have proposed that the thromboembolic events observed with JAK inhibitors may be due to their low selectivity and pan-JAK blockade [20,21].
Thromboembolic events, associated with high morbidity and mortality, involve a complex interplay between pro-coagulant, anticoagulant, and fibrinolytic factors [22]. To elucidate the underlying mechanisms contributing to the increased thromboembolic risk in patients receiving JAK inhibitors, and to identify potential preventive measures, this study aims to clarify the effect of tofacitinib (in comparison with anti-TNF agents) on platelet function and coagulation parameters in UC patients.
2. Results
2.1. Baseline Clinical Characteristics
A total of 30 individuals (10 with active UC (aUC), 10 with quiescent UC (qUC), and 10 healthy controls (HC)) were included in the study. No significant differences were observed in baseline characteristics of the study population such as age, sex, smoking status, and body mass index between the different study groups (Table 1).
2.2. Effects of Tofacitinib and Anti-TNF on Platelet Activation
Platelets have an essential role in clot formation, playing a crucial part in both hemostasis and thrombosis. In the current study, the effect of tofacitinib and anti-TNF drugs on platelet activation in patients with aUC, qUC, and HC was evaluated. As observed in Figure 1, the results demonstrate that tofacitinib enhanced exposure of CD63 and CD62P and binding of PAC-1 in quiescent platelets from qUC and aUC, indicating an activating effect on platelets. CD63 is a lysosomal marker associated with granule release, CD62P (P-selectin) is a key molecule involved in platelet aggregation and interaction with leukocytes, and PAC-1 binding reflects the conformational activation of the fibrinogen receptor (GPIIb/IIIa), which is crucial for platelet aggregation. However, this effect does not appear to be specific to tofacitinib, as anti-TNF also produced the same effect on CD63 exposure and PAC-1 binding. Notably, while there is actually a general trend toward increased platelet activation in qUC and HC following exposure to tofacitinib and anti-TNF, the only statistically significant effect observed in these groups is the increase in CD63 expression.
To further explore the functional responsiveness of platelets to strong agonists, their activation following stimulation with thrombin receptor activating peptide (TRAP) was assessed, as depicted in Figure 2. Consistent with the findings in Figure 1, we observed that both tofacitinib and anti-TNF drugs significantly increased CD63 expression on platelets from patients with aUC after stimulation with TRAP.
2.3. Effect of Tofacitinib and Anti-TNF on Platelet Aggregation
Maximum platelet aggregation induced by adenosine diphosphate (ADP) (2.5 µM and 5.0 µM) was assessed in three groups (HC, qUC, and aUC) under three experimental conditions (incubation with tofacitinib, with anti-TNF, and without drug). No significant differences in platelet aggregation were observed between the different experimental conditions in any of the groups (Figure 3).
2.4. Effect of Tofacitinib and Anti-TNF on Thrombus Dynamics
To evaluate the effect of the treatments on hemostasis, blood coagulation was analyzed ex vivo for the different groups in the presence of tofacitinib, anti-TNF, or no drug using ROTEM. Extrinsic activation with tissue factor (EXTEM) and intrinsic activation with tissue factor (INTEM) assays were performed evaluating the hemostatic parameters MCF, CFT, and CT. No significant differences were observed in these parameters between the different experimental conditions in the three experimental groups (aUC, qUC, and HC) in both the EXTEM (Table 2) and INTEM (Table 3) assays.
3. Discussion
This is the first study evaluating the effect of tofacitinib on platelet function and coagulation in UC patients, in comparison with the anti-TNF agent infliximab. The ex vivo approach used in this study allows for better control of experimental conditions and minimizes inter-individual variability, thereby enhancing the reliability of our findings. Furthermore, evaluating patients in remission has allowed us to explore whether thrombotic risks in UC patients are a consequence of active inflammation or are inherently related to the disease or to treatment strategies. The goal was to pinpoint whether the prothrombotic susceptibility observed in UC, potentially due to treatment with tofacitinib, might necessitate the use of antiaggregant or anticoagulant therapy as part of patient management.
Our results demonstrate that both tofacitinib and anti-TNF increase the expression of platelet activation markers, such as CD63 and the PAC-1 binding antigen, in both aUC and qUC patients. This increase appears to result from the direct addition of these drugs to platelets in the ex vivo setting. However, these changes did not lead to measurable alterations in primary hemostatic functions, such as platelet aggregation. Notably, when TRAP, a specific agonist peptide for protease activated receptor (PAR)-1 and PAR-4, was added to platelet-rich plasma (PRP), differences in platelet activation between the groups were mitigated except for the patients with aUC. This finding suggests that prior drug exposure might modulate the response to TRAP stimulation through platelet desensitization or partial inhibition of specific signaling pathways.
Despite the increase in platelet activation observed with both drugs (tofacitinib and anti-TNF), no significant differences in aggregation were detected under the conditions tested. These results indicate that tofacitinib- and anti-TNF-induced increases in platelet activation are not sufficient to translate into changes in aggregation capacity, at least under the ex vivo conditions set in this study. It is possible that this is due to the fact that, despite the aggregometry and cytometry experiments being performed in PRP, the experimental conditions used in each were different. The unique effect of tofacitinib in the TRAP-induced dense granules release from platelets of aUC is not striking because the release of platelet granules is not uniform [23]. ROTEM analysis revealed no significant differences in clot formation parameters (in EXTEM and INTEM assays) between the treatment groups (tofacitinib, anti-TNF or no drug) in any of the patient groups (HC, qUC, or aUC). These results suggest that neither tofacitinib nor anti-TNF is able to substantially alter the dynamics of clot formation or the viscoelastic properties of the clot under the experimental conditions of these coagulation assays.
The clinical implications of our findings could be particularly relevant for treatment decision-making in UC patients receiving tofacitinib. Our study provides evidence that tofacitinib does not significantly alter primary hemostatic function or coagulation under ex vivo conditions, supporting its continued use without an immediate need for anticoagulant or antiplatelet co-therapy in this context.
The implications of these findings support the notion that the prothrombotic risks associated with UC are complex and may not be directly exacerbated by tofacitinib in the settings evaluated in this study. Moreover, they indicate that tofacitinib does not appear to significantly compromise primary hemostatic or coagulation processes in UC patients. Given the absence of studies directly addressing these aspects, our findings fill an important gap in the literature and offer a basis for further exploration. While the data suggest a lack of increase in thrombotic risks under tofacitinib treatment, this conclusion should be interpreted cautiously due to the limitations of our study.
We recognize that the ex vivo design of our study may not fully capture the complexity of in vivo physiological responses. The interactions between platelets, endothelial cells, and the immune system in a live organism could lead to different outcomes. Furthermore, the ex vivo nature of the study limits the assessment of potential confounding factors such as the influence of inflammatory cytokines or changes in the vascular environment, which could alter the results under in vivo conditions. Potential biases could also arise from the controlled nature of the ex vivo setting, as it does not account for the systemic effects of drugs or disease that might modulate platelet function and coagulation in a more dynamic, whole-body context.
The sample size of our study, with 30 patients, is relatively small and may limit the statistical power of our results, potentially reducing our ability to detect subtle differences between groups. To mitigate this limitation, we carefully controlled experimental conditions and employed paired analyses within the same individuals, minimizing inter-individual variability. Nevertheless, larger studies are needed to validate these findings and improve their generalizability.
Our results align with existing literature suggesting that tofacitinib does not increase thrombotic risk in UC patients [6,24], in contrast with some concerns raised in other immune-mediated diseases [8,14]. These discrepancies may be attributed to multiple factors. First, a key difference lies in the study population. While our study focuses on UC patients, previous reference studies analyze thromboembolic risk in rheumatoid patients. Second, our study employs an ex vivo approach, directly evaluating platelet function and coagulation through aggregometry, flow cytometry, and ROTEM analyses in samples from UC patients. In contrast, previous studies analyzed the incidence of thromboembolic events, without including direct assessment of platelet activation or coagulation. The differences observed between diseases such as rheumatoid arthritis and UC highlight the importance of disease-specific investigations and caution against broad extrapolation of data across distinct patient populations. These findings underscore that the thrombotic risk profile of therapies may not be universally applicable and emphasize the importance of tailored evaluations for each disease context.
4. Material and Methods
4.1. Study Design
A total of 30 participants were included in the study: 10 aUC patients, 10 qUC patients, and 10 HC. The study was approved by the Ethics Committee of Hospital Universitario de La Princesa (GIS-2021-JAKihemo). All participating patients provided written informed consent, and all data were anonymized to ensure confidentiality. Figure 4 summarizes the study design.
The inclusion criteria were as follows: (1) UC patients: age 18 years or older, with diagnosis of UC according to the criteria of the European Crohn’s and Colitis Organisation (ECCO). Concomitant treatments were allowed if the treatment had remained stable for at least three months prior to the study. For active UC patients, endoscopic activity within one month after starting the treatment was required (Mayo endoscopic sub-score ≥ 2). (2) HC: Individuals without UC or any other inflammatory, allergic, malignant, or autoimmune disease.
The exclusion criteria were as follows: (1) UC patients: age under 18 years; presence of an immune-mediated disease, neoplasm, or active infection; pregnancy or breastfeeding; alcohol or drug abuse; ostomy; abdominal surgery in the last 6 months; colectomy; active infection by hepatitis B, C or human immunodeficiency virus (HIV); medical history of thromboembolic events; treatment with anticoagulants, antiplatelets, or other medications affecting blood coagulation; use of combined hormonal contraceptives or hormone replacement therapy; and hereditary coagulation disorders. (2) HC: Age under 18 years; presence of advanced chronic disease or any condition that prevents the monitoring of the protocol of this study; pregnancy or breastfeeding; active infection with hepatitis B, C, or HIV virus; alcohol or drug abuse; medical history of thromboembolic events; ongoing treatment with anticoagulants, antiplatelets, or other medications that alter blood coagulation; use of combined hormonal contraceptives or hormone replacement therapy; and hereditary coagulation disorders.
4.2. Blood Collection and Processing
Blood samples were collected from each participant in 6 sodium citrate tubes (3.2%, 454332 BD Vacutainer, Greiner Bio-One International GmbH, Madrid, Spain). Prior to functional assays, whole blood or PRP from each patient was incubated at 37 °C for 30 min in gentle shaking under three different experimental conditions: (1) tofacitinib (2.9 mg/mL), (2) anti-TNF (infliximab) (10 mg/mL), and without any drug [phosphate-buffered saline (PBS) solution].
4.3. Evaluation of Platelet Activation by Flow Cytometry
Whole blood was centrifuged at 152 g for 15 min at 25 °C with 9 accelerations and 3 decelerations to obtain PRP. PRP was diluted 1:5 with wash buffer (137 mM NaCl, 2.7 mM KCl, 1 mM NaH_2_PO_4_, 20 mM HEPES, 0.1% glucose, and 0.1% bovine serum album; pH 7.4). Subsequently, PRP was incubated in the presence of tofacitinib or anti-TNF. Following incubation, PE-anti CD41 (5112-PE100T, BioCytex, Marseille, France), FITC-anti CD62P mAb (a marker of the release from platelet’s alpha granules), FITC-anti CD63 mAb (a marker of the release from platelet’s dense granules), and FITC-anti PAC-1, an mAb that only recognizes the active conformation of the fibrinogen receptor (555523, 557288, 340507, respectively; Biosciences, NJ, USA), were added for 20 min at room temperature. The samples were then diluted in PBS for flow cytometry (BD Canto II, BD Biosciences). Data were analyzed using FlowJo software 10.8 (Ashland, OR, USA). Platelet activation was assessed at baseline and after stimulation with TRAP (Roche Diagnostics, Rotkreuz, Switzerland).
4.4. Platelet Aggregation
Platelet aggregation was measured in PRP using a lumiaggregometer (Helena Biosciences Europe, Beaumont, TX, USA). PRP was prepared as described above, and platelet-poor plasma (PPP) was obtained by centrifugation of whole blood at 3250 rpm for 20 min at 25 °C. PPP served as the reference for equipment calibration, and PRP was adjusted to 200–300 × 10^3^ platelet/µL with PPP. PRP was incubated in the presence of tofacitinib, anti-TNF, or no drug (control group). Aggregation was induced by adding ADP at concentrations of 2.5 µM and 5 µM and measured for 10 min by light transmission aggregometry. Results were expressed as percentage of maximal aggregation.
4.5. Whole Blood Coagulation
Whole blood coagulation was assessed using rotational thromboelastometry ROTEM^®^ (TEM Innovations GmbH, Munich, Germany) according to the manufacturer’s instructions. Blood was collected in 3 sodium citrate tubes. One tube was incubated with tofacitinib, one with anti-TNF, and one with no drug. The assays used were EXTEM and INTEM. Maximum clot firmness (MCF), clot formation time (CFT), and clotting time (CT) were measured after ex vivo supplementation with tofacitinib or anti-TNF and without any drug (PBS buffer).
4.6. Sample Size
The sample size for the ex vivo study was 10 subjects for each experimental group (aUC, qUC, and HC). Based on previous studies, a sample size of 8 patients was considered capable of providing 80% power to detect a 2 mm difference in MCF, with a significance level of 0.05 and a standard deviation of 2 mm. An increase of 2 mm corresponded to approximately a 20% increase in MCF [25,26,27]. Therefore, for this pilot study involving comparisons between groups, a sample size of 10 subjects per group was deemed sufficient to detect changes in hemostasis. Furthermore, previous studies evaluating coagulation alterations using ROTEM parameters, as well as platelet function, included a similar sample size [25,28,29,30].
4.7. Statistical Analysis
Descriptive statistics were employed to report characteristics of the study population including age, sex, and smoking status (smoker or non-smoker). These data were presented as means ± standard deviations (SD) for continuous variables and as percentages for categorical variables.
The data were analyzed using Graph Pad Prism software (version 9.5.1; Graph pad Software Inc., San, CA, USA). Comparisons of ROTEM, platelet aggregation, and platelet activation data between the three groups (aUC, qUC, and HC) under three experimental conditions (ex vivo incubation with tofacitinib, anti-TNF, or no drug) were performed using two-way ANOVA. p-values < 0.05 were considered statistically significant.
5. Conclusions
This study provides valuable insights into the effects of tofacitinib and infliximab on platelet activation and coagulation in UC patients. Although both tofacitinib and anti-TNF increased platelet activation markers, they did not significantly affect platelet aggregation or coagulation under our ex vivo experimental conditions. These findings suggest that, at least in the settings tested, tofacitinib and anti-TNF therapies do not significantly alter hemostatic function. Further research, including larger studies and in vivo models, is needed to better understand the long-term thrombotic risks and refine treatment strategies for UC patients.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Ordás I. Eckmann L. Talamini M. Baumgart D.C. Sandborn W.J. Ulcerative colitis Lancet 20123801606161910.1016/S 0140-6736(12)60150-022914296 · doi ↗ · pubmed ↗
- 2Høivik M.L. Moum B. Solberg I.C. Henriksen M. Cvancarova M. Bernklev T. Work disability in inflammatory bowel disease patients 10 years after disease onset: Results from the IBSEN study Gut 20136236837510.1136/gutjnl-2012-30231122717453 · doi ↗ · pubmed ↗
- 3Collins P. Rhodes J. Ulcerative colitis: Diagnosis and management Br. Med. J.200633334034310.1136/bmj.333.7563.34016902215 PMC 1539087 · doi ↗ · pubmed ↗
- 4Chaparro M. Gisbert J.P. Maintenance therapy options for ulcerative colitis Expert Opin. Pharmacother.2016171339134910.1080/14656566.2016.118713227240112 · doi ↗ · pubmed ↗
- 5Ford A.C. Sandborn W.J. Khan K.J. Hanauer S.B. Talley N.J. Moayyedi P. Efficacy of biological therapies in inflammatory bowel disease: Systematic review and meta-analysis Am. J. Gastroenterol.201110664465910.1038/ajg.2011.7321407183 · doi ↗ · pubmed ↗
- 6Chaparro M. Garre A. Mesonero F. Rodríguez C. Acosta M.B.-D. Martínez-Cadilla J. Arroyo M.T. Manceñido N. Sierra-Ausín M. Vera-Mendoza I. Tofacitinib in ulcerative colitis: Real-world evidence from the ENEIDA registry J. Crohn’s Colitis 202115354210.1093/ecco-jcc/jjaa 14532969471 · doi ↗ · pubmed ↗
- 7Zhang J. Li W. Gong M. Gu Y. Zhang H. Dong B. Guo Q. Pang X. Xiang Q. He X. Risk of venous thromboembolism with janus kinase inhibitors in inflammatory immune diseases: A systematic review and meta-analysis Front. Pharmacol.202314118938910.3389/fphar.2023.118938937351513 PMC 10282754 · doi ↗ · pubmed ↗
- 8Weitz J.I. Szekanecz Z. Charles-Schoeman C. Vranic I. Sahin B. Al Paciga S. Wang Z. Hyde C. A Martin D. Biomarkers to predict risk of venous thromboembolism in patients with rheumatoid arthritis receiving tofacitinib or tumour necrosis factor inhibitors RMD Open 20228 e 00257110.1136/rmdopen-2022-00257136323490 PMC 9639150 · doi ↗ · pubmed ↗