Combined TaTME with SP Robot for Low Anterior Resection in Rectal Cancer: rSPa TaTME
Nouran O. Keshk, Mauricio E. Perez-Pachon, Ibrahim Gomaa, Sara Aboelmaaty, David W. Larson, Kristen K. Rumer, Sherief F. Shawki

TL;DR
This paper introduces a new surgical method combining robotic and transanal techniques for rectal cancer, showing it is safe and effective.
Contribution
The novel contribution is the combined use of robotic and transanal approaches for distal rectal cancer resection.
Findings
All ten patients had negative surgical margins with acceptable lymph node harvests.
No local or distal recurrences were observed during a mean follow-up of 20 months.
Nine out of ten patients had their ileostomy reversed, indicating good recovery.
Abstract
Transanal total mesorectal excision (TaTME) has been utilized to overcome the difficulties associated with distal proctectomy. At the same time, single-port robotic abdominal (rSPa) procedures allow minimally invasive, single-incision abdominal dissection during proctectomy (rSPa TaTME). We are reporting our initial experience with ten patients who underwent combined single-port robotic abdominal and TaTME approaches for the resection of distal rectal cancers. The benefits of this approach are that (1) the defunctionalizing stoma is placed at the SP site, so there is no appearance of incisions, and (2) the TaTME approach facilitates distal TME and anastomosis after the resection of very distal tumors, even in anatomically challenging pelvises, while maintaining oncologic principles. As such, rSPa TaTME can be considered a safe and feasible approach with appropriate experience,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
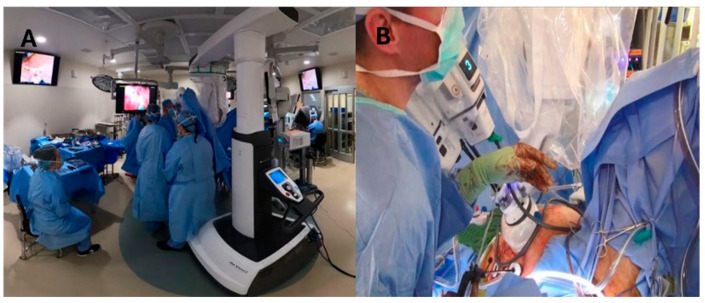 Figure 1
Figure 1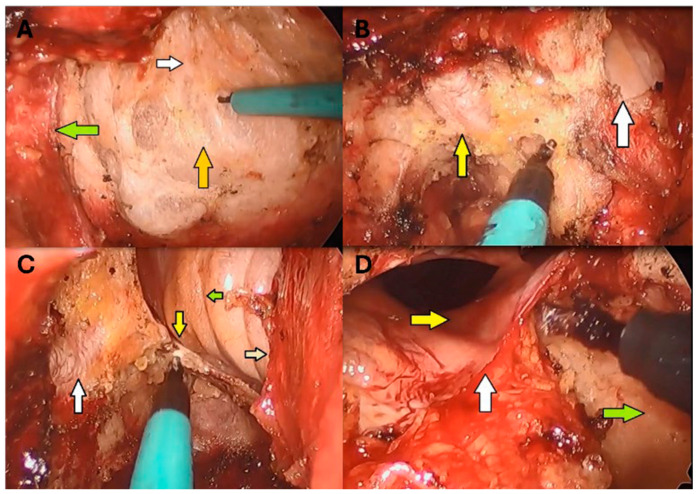 Figure 2
Figure 2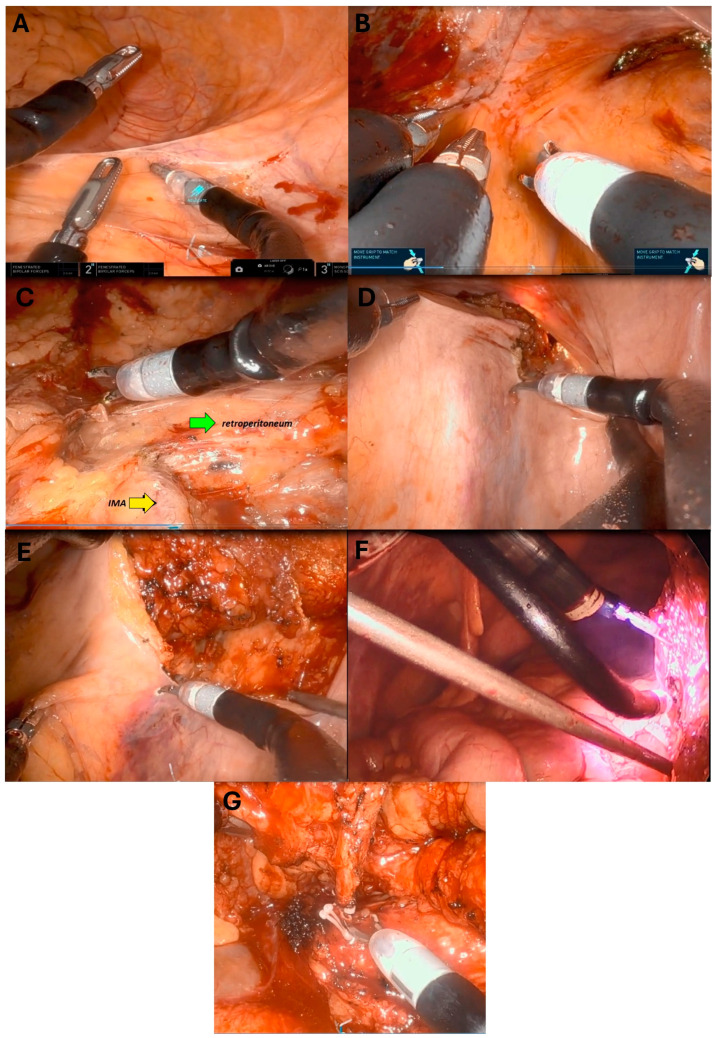 Figure 3
Figure 3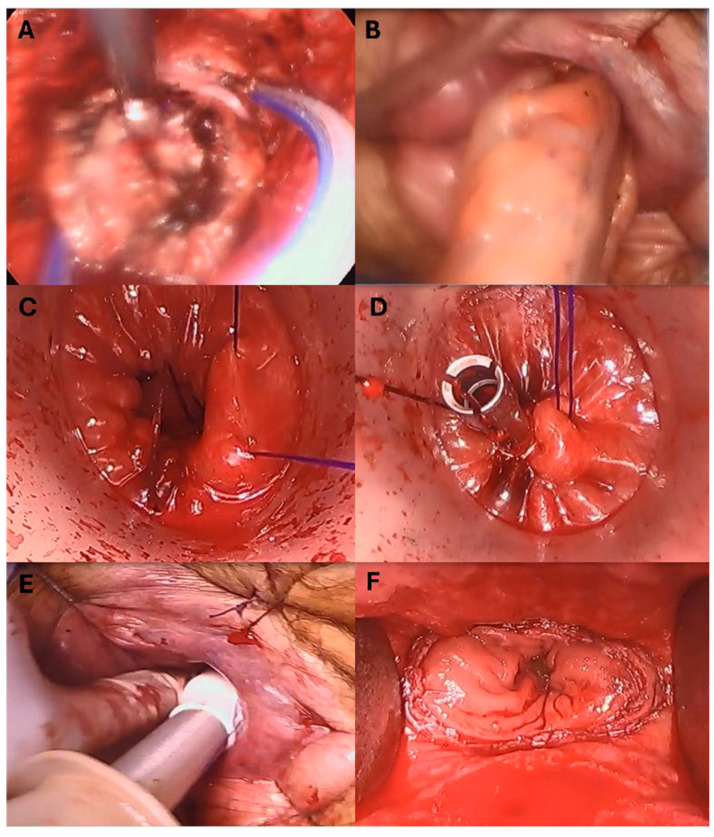 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsColorectal Cancer Surgical Treatments · Surgical Simulation and Training · Colorectal and Anal Carcinomas
1. Introduction
Rectal cancer treatment has evolved significantly over the past few decades, with surgical resection remaining a cornerstone of curative therapy. Among the various surgical approaches, total mesorectal excision (TME) has become the gold standard since its introduction in the early 1980s [1]. The TME approach involves the precise removal of the rectum and mesorectum, reducing local recurrence rates and improving overall survival [2,3,4,5]. Recent advancements in minimally invasive surgery, particularly robotic-assisted TME, have refined the procedure [6,7,8]. Minimally invasive approaches offer the benefits of reduced postoperative pain, shorter hospital stays, and faster recovery while maintaining oncological efficacy [9,10]. Robotic-assisted surgery for rectal cancer provides advantages over both open and laparoscopic surgery in terms of patient outcomes and reducing postoperative complications [11,12,13,14,15,16,17,18]. The single-port robotic abdominal approach (rSPa) for rectal cancer offers additional benefits compared to traditional multi-port robotic surgery or single-incision laparoscopic surgery, including shorter hospital stays, reduced operative times, lower pain, faster recovery, and improved cosmetic results, while maintaining oncologic outcomes [19,20]. For distal tumors, transanal total mesorectal excision (TaTME) facilitates a “bottom-up” dissection approach, which is particularly advantageous in patients with narrow pelvises. Transanal TME allows for excellent visualization of the distal anatomy to improve resection completeness and facilitates anastomosis in patients for whom an abdominoperineal resection might otherwise be required [21], with safe oncologic outcomes [22].
Combining the multi-port robotic abdominal and TaTME approaches for proctectomy has shown advantages in oncological safety and functional preservation EI [23,24,25,26]. By combining the rSPa approach for the abdominal portion of the proctectomy with TaTME for distal rectal cancers, patients have no abdominal incisions other than the SP site, which is used for refunctioning ileostomy. This hybrid approach has the potential to give patients the benefits of less pain, shorter hospital stays, and improved aesthetic outcomes while maintaining the oncologic outcomes of the resection of distal rectal tumors. Here, we report our experience using a combined rSPa and TaTME approach for rectal cancer resection in ten patients.
2. Materials and Methods
This is a descriptive report presenting the safety and feasibility of a new minimally invasive surgical approach combining transanal total mesorectal excision (TaTME) and a single-port (SP) robotic platform for managing distal resectable rectal cancer. We retrospectively reviewed our prospectively maintained database of patients undergoing rectal cancer resection. We evaluated the records from our initial ten patients who underwent rSPa TaTME from May 2022 to August 2024. The variables analyzed included demographics, pre- and post-operative tumor staging, tumor characteristics (including size and distance from the tumor’s distal margin to the anorectal junction), neoadjuvant and adjuvant therapy (chemoradiotherapy and/or radiotherapy), pathologic criteria (including resection completeness, resection margin status, and response to neoadjuvant treatment), the number of lymph nodes harvested, the average operative time, whether ileostomy was reversed, mean follow-up duration, recurrence rates, and 30-day postoperative morbidity. The descriptive statistics are presented as frequencies (percentages) for categorical variables and the mean ± standard deviation (SD) or median (interquartile range) for quantitative variables. All statistical analyses were conducted using SPSS^®^ (version 28; SPSS^®^, Inc., Armonk, NY, USA).
2.1. Surgical Technique and Operative Room Organization
The procedure consisted of 4 phases. The first was the perineal (TaTME) portion, followed by the abdominal portion. Subsequently, the specimen was retracted, usually transanally, and anastomosis was performed. Finally, a diverting loop ileostomy was created where the SP robot was docked. A drain was placed through an assistant AirSeal port, 8 mm. In 2 cases, where an en-bloc total abdominal hysterectomy was performed, the specimen was extracted through the stoma aperture and the anvil was placed in the colonic conduit prior to replacing the conduit in the abdominal cavity.
The patient was placed in the lithotomy position with both arms tucked at their sides to allow for simultaneous abdominal and transanal access. When the dual/simultaneous team approach was complete, the transperineal (TaTME) portion was commenced first, continuing until the desired surgical plane was reached. Subsequently, the stoma aperture was created, followed by docking the robot after positioning the operative table in the Trendelenburg position with a tilt to the right (Figure 1).
2.1.1. Perineal Phase
This portion commenced with placing anal effacement sutures to open the anus, as an alternative to other commercially available retractors. After gentle and gradual dilation of the anal canal, the access channel was placed inside it. An occlusive purse-string suture was placed in the rectum distal to the location of the tumor using 0 Prolene (Ethicon Inc., Somerville, NJ, USA) on an SH needle. Betadine (Atlantis Consumer Healthcare Inc., Bridgewater, NJ, USA) solution was applied to the distal rectum. The gel cap was assembled after placing 2 ports and an 8 mm AirSeal (ConMed Corporation, Largo, FL, USA) port in a triangular formation. Insufflation was established using the AirSeal. A full-thickness circumferential proctectomy was performed, with the TME plane entered posterolaterally and then connected at the midline. Subsequently, dissection was extended anteriorly, and the plane between the anorectal junction and the prostate/vagina was identified. Dissection was then resumed posteriorly, extending cephalad and then widening the dissection bilaterally toward the distal pelvic wall. At the level of S3, Waldeyer’s (rectosacral) fascia was incised sharply. Then, the dissection trajectory was directed upward, near a right angle and parallel to the upper sacrum, at the S1/S2 level. At this point, attention was turned toward the anterior plane, which had been initially identified. Dissection then ensued cephalad to the level of the peritoneal reflection, which was incised sharply, entering the cul-de-sac. Finally, the lateral rectal attachments between the distal rectum and distal pelvic side wall, including the levator ani muscle, were taken down with cautery until reaching the level of the peritoneal reflection. The dissection then extended above the reflection as much as possible using LigaSure (Medtronic, Minneapolis, MN, USA) (Figure 2).
2.1.2. Abdominal Phase
We placed a single port for robotic instruments (Da Vinci Single-Port System, Intuitive Surgical, Sunnyvale, CA, USA) at the lower right quadrant site, which was pre-planned for defunctioning the stoma. This 2.5 cm multi-channel port comprises a camera and three interchangeable arms (e.g., scissors, clippers, graspers, etc.).
The stoma aperture was created in the previously marked site, usually in the lower right quadrant: an assistant AirSeal port, 8 mm, was placed below the stoma aperture. The robotic SP (Da Vinci Single-Port System, Intuitive Surgical, Sunnyvale, CA, USA) wound protector was applied, where the outer ring was attached to the sealed tube/bag to contain the SP cannula. Subsequently, the robot was docked, and the instruments were assembled, with scissors in arm 1 and a fenestrated bipolar in arms 2 and 3. The camera was assembled in its channel of a single port. The port was introduced into the abdominal cavity through the stoma aperture, directed toward the left lower quadrant, after the abdomen was insufflated. Once the SP port was in the abdominal cavity, the instruments were extended through the channels.
The sigmoid and descending colon were typically mobilized from lateral to medial, up to and around the splenic flexure. Alternatively, a sub-inferior mesenteric vein approach was implemented to mobilize the splenic flexure. Once full medialization was accomplished, identified by reaching the midline, a medial-to-lateral approach was followed at the level of the rectosigmoid junction. This connected with the TaTME dissection plane in the upper pelvis and the lateral dissection plane. The superior hemorrhoidal vessels were identified and followed cephalad until the inferior mesenteric artery was identified. The artery was then skeletonized and secured with clips or an energy device introduced through the assistant port since there was no vessel sealer available for the SP robotic platform at the time. The inferior mesenteric vein was then divided using an energy device, followed by division of the left colic vessel. Then, the mesentery was dissected toward the future transection points in the colon. This was divided similarly until reaching the colonic wall. If the transanal approach failed to reach the upper sacrum, the superior hemorrhoidal vessels were again followed, but this time caudally, entering the TME plane. The final few centimeters of attachments between the upper rectum and the perirectal gutter were then dissected. Hemostasis was also performed once the dissection was deemed complete and tension-free reach was ensured. The robotic instruments were removed, and the robot was undocked (Figure 3).
2.1.3. Transanal Extraction and Anastomosis
In eight cases, the specimen was retrieved transanally without disruption, with a wound protector placed through the anal canal and residual rectum. The colon was transected, and the anvil was secured in the usual fashion. A silk suture (Ethicon Inc., Somerville, NJ, USA) was tied around the anvil to be able to pull on it while creating the end-to-end anastomosis. Then, the anvil with the colonic conduit was placed just beyond the rectal cuff, which was dissected from the surrounding structure, creating a lip in preparation for the second purse-string. Using 0 Prolene (Ethicon Inc., Somerville, NJ, USA), the second purse-string was placed. The anvil was then pulled through the rectum using the silk suture on the anvil with the guidance of a pick-up. The rectal purse-string was then tied tightly around the anvil while pulling on the silk suture to ensure appropriate opposition between the anvil inside the colon and the rectal cuff. The access channel was then removed, and the EEA spike was engaged with the anvil. The surgeon gloved index finger swept around the stapler to make sure no other structure was involved with the stapler interface. The stapler was then fired, and moved, and the donuts were checked for completeness.
In the two cases where the specimens were exteriorized through the stoma site, the colonic conduit was directed to the pelvis after insufflating the abdominal cavity. It was then retrieved transanally using a grasper through the anus after placing the second purse-string suture. The rest of the anastomosis was performed in a similar fashion (Figure 4).
2.1.4. Stoma Creation
A loop of the bowel was chosen to create the diverting loop ileostomy. A 19-French channel Blake drain (Ethicon Inc., Somerville, NJ, USA) was placed through the assistant port into the pelvis. The abdomen was then deflated while the loop of the bowel was held in an oriented fashion and brought through the stoma aperture. The wound protector was removed, and the stoma aperture was reduced in size to accommodate the loop of the bowel, accordingly, using 0 Vicryl (Ethicon Inc., Somerville, NJ, USA) on a UR6 needle. The ileostomy was then sutured to the skin in the usual fashion using 3–0 Vicryl (Ethicon Inc., Somerville, NJ, USA) sutures.
In situations where the specimen could not be accommodated through the anal canal, the specimen was exteriorized through the stoma aperture if deemed appropriate. In our cases, only two specimens, both from en-bloc TAH, were exteriorized through the stoma. After transection and securing the anvil in the colonic conduit, the colon was placed in the abdominal cavity. Insufflation was established, and the conduit was delivered to the distal pelvis in an oriented manner, while the transanal team retrieved it under vision. The anastomosis was then performed as described above.
Postoperative care was provided as per institutional protocols, according to individual needs.
3. Results
Ten consecutive patients who had rSPa TaTME dissection for rectal cancer resection were included in the analysis (six females and four males). All ten surgeries were performed consecutively, with eight conducted by one senior surgeon and the remaining two by the same senior surgeon alongside another senior surgeon. The median age at the time of surgery was 53 (range: 37–85), with a mean body mass index (BMI) of 26 kg/m^2^ (Table 1).
One patient (P1) was diagnosed with clinical stage I and went directly to surgery, followed by adjuvant chemotherapy. Of the three patients with clinical stage II, two (P3 and P10) were treated with neoadjuvant short-course radiation, followed by surgery, while the third patient (P5) went straight to surgery. The six patients with clinical stage III underwent total neoadjuvant therapy. Based on pre-operative MRI, the mean distance of the distal tumor border from the anorectal junction was 3.2 cm (range: 2–5.3 cm). All operations were completed as rSPa TaTME without any conversions to a different approach. The average operative time was 351 min. All patients had negative distal and circumferential margins. There were eight complete TME specimens, one near-complete specimen, and one incomplete specimen. The mean number of lymph nodes harvested was 24, and the lowest number of harvested lymph nodes was 13 (Table 2 and Table 3). Nine patients underwent ileostomy reversal. One patient did not undergo ostomy reversal due to functional decline after a stroke. The mean follow-up period was 20 months (4 to 30 months). Six patients experienced complications within 30 days post-surgery, including ileus, small bowel obstruction, acute kidney injury (AKI), deep vein thrombosis, anemia requiring transfusion, and stroke (Table 3). Five of our patients were classified as Clavien–Dindo grade I-II, one patient (P6) as Clavien–Dindo grade IIIA, and the remaining patients as Clavien–Dindo grade 0. Notably, none of our patients experienced symptoms of LARS or a significant increase in stool frequency after stomal reversal.
4. Discussion
Rectal cancer resection has witnessed advancement in surgical approaches and minimally invasive modalities, particularly with the emergence of robotic surgery and TaTME, both of which have facilitated surgical techniques for mid- and low-rectal cancers [8,27,28]. TaTME offers a “bottom-up” approach that provides surgeons with improved visualization and access to the distal rectum, addressing some of the limitations inherent in traditional methods, particularly in narrow pelvises. This technique has been successful in oncological outcomes, with studies showing at least equivalent resection margins and reduced local recurrence rates compared to conventional methods [29,30,31,32]. It is essential to remember that TaTME requires specialized training/expertise and is not universally available [33,34]. Single-port approaches to abdominal surgery have benefited patients in terms of omitting multiple incisions and reducing pain. In this series, we have combined these two innovative approaches to rectal cancer resection with rSPa TaTME.
In our initial experience, ten patients successfully underwent the rSPa TaTME approach, with no conversions to a different approach. Postoperative complications were consistent with those typically encountered for proctectomy, including venous thromboembolic events treated with anticoagulation, an abscess requiring antibiotics, a seroma that was drained, ileus or obstruction in three patients managed conservatively, a UTI requiring antibiotics, AKI managed with hydration, and anemia requiring transfusion. One patient did experience a stroke and did not have their defunctioning ileostomy reversed, while the remaining nine patients had their gastrointestinal continuity restored. The oncologic outcomes were reassuring, with eight complete TME specimens, one nearly complete, and one incomplete. All had adequate lymph node retrieval, with the lowest number being 13. With a mean follow-up of 20 months, no patient experienced cancer recurrence. At centers with robotic surgery and TaTME expertise, rSPa TaTME offers an innovative approach to distal rectal cancers. It is imperative to mention that the mean operative time was more than 5 h since most of these cases were performed consecutively, in addition to getting used to the SP ergonomics. These ergonomics are entirely different than the straight sticks and XI multi-port robotic platform. Unlike XI instruments, where 3-D movement is available at the used tip (scissors, fenestrated bipolar, etc.), the SP arms have an elbow that bends acutely, affecting the trajectory of instrument movement.
Furthermore, handling the camera with and without the cobra position is not initially easy. The cobra position is obtained by bending the camera shaft at its elbow, thus providing a semi-overview of the dissection. Finally, moving inside the abdominal cavity requires full pivot-like movement. This requires retracting the instruments in their respective channels, moving the port toward the desired location, and then reintroducing them accordingly. Collectively, this resulted in longer operative durations, in addition to the usual factors, such as visceral obesity and adhesions.
Limitations
The retrospective nature of our small cohort of patients presents limitations in the level of evidence. The case series nature of our study limits its comparability to other techniques. More extensive studies are required.
5. Conclusions
Combining the abdominal single-port robotic approach with transanal total mesorectal excision (rSpa TaTME) for the resection of distal rectal cancer showed acceptable surgical and oncologic outcomes in this initial series. However, this technically demanding procedure is still being explored and should be performed in high-volume centers, with appropriate experience and careful review.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Heald R.J. Husband E.M. Ryall R.D.H. The Mesorectum in Rectal-Cancer Surgery—The Clue to Pelvic Recurrence Br. J. Surg.19826961361610.1002/bjs.18006910196751457 · doi ↗ · pubmed ↗
- 2Gloor S. Pozza G. Troller R. Wehrli M. Adamina M. Surgical Outcomes, Long-Term Recurrence Rate and Resource Utilization in a Prospective Cohort of 165 Patients Treated by Transanal Total Mesorectal Excision for Distal Rectal Cancer Br. J. Surg.2023110 V 910.1093/bjs/znad 178.029PMC 995431236831531 · doi ↗ · pubmed ↗
- 3Bolmstrand B. Nilsson P.J. Eloranta S. Martling A. Buchli C. Palmer G. Survival after surgery beyond total mesorectal excision for primary locally advanced rectal cancer, a population-based study EJSO Eur. J. Surg. Oncol.20245010867310.1016/j.ejso.2024.10867339476462 · doi ↗ · pubmed ↗
- 4Lu F. Tan S.G. Zuo J. Jiang H.H. Wang J.H. Jiang Y.P. Comparative efficacy analysis of laparoscopic-assisted transanal total mesorectal excision laparoscopic transanal mesorectal excision for low-lying rectal cancer World J. Gastrointest. Surg.20251710036410.4240/wjgs.v 17.i 1.10036439872764 PMC 11757205 · doi ↗ · pubmed ↗
- 5Hellan M. Anderson C. Ellenhorn J.D.I. Paz B. Pigazzi A. Short-term outcomes after robotic-assisted total mesorectal excision for rectal cancer Ann. Surg. Oncol.2007143168317310.1245/s 10434-007-9544-z 17763911 · doi ↗ · pubmed ↗
- 6Piozzi G.N. Duhoky R. Przedlacka A. Di Giuseppe D.R. Khan J.S. Artificial intelligence real-time mapping with Eureka during robotic total mesorectal excision for rectal cancer: A video vignette Color. Dis.202527 e 1724010.1111/codi.1724039551959 · doi ↗ · pubmed ↗
- 7Guo Y.C. He L. Tong W.D. Chi Z.C. Ren S.Y. Cui B.B. Wang Q. A study of intersphincteric resection rate following robotic-assisted total mesorectal excision versus laparoscopic-assisted total mesorectal excision for patients with middle and low rectal cancer: Study protocol for a multicenter randomized clinical trial Trials 20242570310.1186/s 13063-024-08561-439434171 PMC 11495107 · doi ↗ · pubmed ↗
- 8Zhang X. Chen J. He F. Du W.C. Li X.H. Yu X.H. Comparing efficacy and safety of transanal vs. laparoscopic total mesorectal excision for middle and low rectal cancer: Updated meta-analysis EJSO Eur. J. Surg. Oncol.20255110955910.1016/j.ejso.2024.10955939765193 · doi ↗ · pubmed ↗